![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
625 Cards in this Set
- Front
- Back
|
What are the indications for a carotid endarterectomy? |
More than 70% stenosis & symptomatic |
|
|
What is the most common leukemia in kids?
|
ALL
|
|
|
What is the most common leukemia in adults (in the US)?
|
CLL |
|
|
Philadelphia Chr is almost always seen in this type of leukemia:
|
CML
|
|
|
Which type of leukemia:
Smudge cells on peripheral smear |
CLL
|
|
|
Which type of leukemia:
Peripheral blasts are PAS(+) and Tdt(+) |
ALL
|
|
|
Which type of leukemia:
Peripheral blasts are PAS(-), myeloperoxidase(+) and have Auer rods |
AML
|
|
|
Which type of leukemia:
Pancytopenia in a Down Syndrome pt |
ALL
|
|
|
What is the next step in management of testicular torsion confirmed with U/S?
|
Manual detorsion & bilateral testicular orchioplexy
|
|
|
What are the causes of hypovolemic hyponatremia?
|
Thiazide diuretics
Addison’s disease Fluid loss + H2O replacement |
|
|
Fever + rash + ↑ Cr + eosinophilia → what is the dx?
|
Acute Interstitial nephritis (AIN)
|
|
|
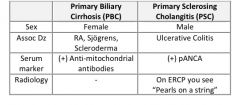
What distinguishes primary biliary cirrhosis from primary sclerosing cholangitis?
|
|
|
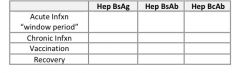
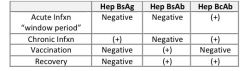
What type of current or past Hepatitis B exposure is present in each of the following scenarios?
|
|
|
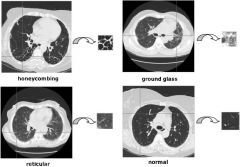
What is the differential dx of ground-glass infiltrates on CXR?
|
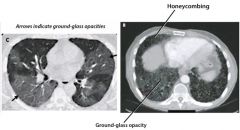
Interstitial pneumonia
PCP Pulmonary edema (ie CHF, ARDs) Pulmonary hemorrhage Hypersensitivity pneumonitis |
|
|
What is the treatment for Whipple disease?
|
TMP-SMX (Bactrim) for 1 yr
|
|
|
What medication is used to close a PDA?
|
Indomethacin
|
|
|
What complications can arise from electrical burns?
|
Cardiac dysrhythmias
Compartment syndrome Bony injuries Myoglobinuria → renal failure Neurologic disturbances |
|
|
What eye abnormality is seen with a lesion to the oculomoter nerve (CN 3)?
|
Fixed, dilated pupil with Down & out gaze
|
|
|
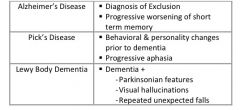
What are the differing presentations of Alzheimer’s dementia, Pick’s disease, and Lewy body dementia?
|
|
|
|
What's the derm term for:
Flat spot <1cm (non-palpable, just visible) |
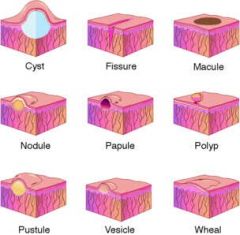
Macule
examples: Freckles, tattoos |
|
|
What's the derm term for:
Flat spot > 1cm |
Patch
examples: port-wine stain |
|
|
What's the derm term for:
Solid, elevated lesion < 1cm (palpable) |
Papule
mneumonic: "Palpable Papules" examples: Wart, acne, lichen planus |
|
|
What's the derm term for:
Same as papule but >1cm and flat-topped |
Plaque
example: psoriasis |
|
|
What's the derm term for:
Palpable, solid lesion > 1cm & not flat-topped |
nodule
ex: Small lipoma, erythema nodosum |
|
|
What's the derm term for:
Elevated, circumscribed lesion <5mm containing clear fluid (small blister) |
Vesicle
ex: Chickenpox, genital herpes |
|
|
What's the derm term for:
Same as vesicle but >5mm (large blister) |
bulla
ex: Contact dermatitis Pemphigus |
|
|
What's the derm term for:
Itchy, transiently edematous area |
wheal
ex: allergic reaction |
|
|
Describe the proper treatment for skin abscesses
|

|
|

What are some of the distinguishing characteristics of necrotizing fasciitis?
|
Unexplained, excruciating pain in the absence of or beyond areas of cellulitis
Erythema with blister and bullae formation & possible crepitus DM patient with foot cellulitis and signs of systemic toxicity Perineal cellulitis with abrupt onset & rapid spread (Fournier’s gangrene) |
|
|
What is the general treatment for necrotizing fasciitis?
|
Immediate, extensive surgical debridement
Antibiotics: General empiric polymicrobial coverage → imipenem (or meropenem) +/- vancomycin If streptococci → Penicillin G +/- Clindamycin If Clostridia → Penicillin G + Clindamycin Treatment for shock if it arises (IVF, dopamine) |
|
|
What are the distinguishing characteristics of gangrene?
|

|
|

What is the treatment for a limb with dry gangrene?
|
Autoamputation over time
Angiography to evaluate the extent & location of peripheral artery disease → distal bypass of stenotic areas → if circulation improves & healing is adequate, then amputation of the affected region |
|

What is the treatment for wet gangrene infection?
|

Emergency debridement or guillotine amputation of the infected portion of the foot then revision to a below or above the knee amputation 72 hours later
(antibiotics are indicated if cellulitis or gas gangrene is present) |
|
|
A 66 yo M with long-standing poorly controlled DM arrives at the ER c/o a horrid smell coming from his left foot. He denies pain, but admits to having lost the feeling in his feet a long time ago from the diabetes. On exam there is an open wound btw the 1st and 2nd toe on the left foot. Pus drains from the wound and some crepitus is felt in the area. The odor is atrocious. The pt is tachycardic and feverish. What tx does he need?
|
Dx: Wet gangrene
Tx: emergency surgical exploration & debridement; possible amputation |
|
|
A 44 yo AA woman is in the office for evaluation of an area of inflammation in her left axilla. She said that initially the area was simply itchy but has now become painful. On exam the area has about 6 papules and nodules that are erythematous, indurated and warm. The skin is fluctuant, and drainage is noted at some of the lesions. How will this patient need to be treated?
|
Dx: Hidradenitis
Tx: Incision & Drainage (I&D) + Antibiotics Note: Hydradenitis Suppurativa treatment: Tetracyclines Macrolides Intralesional steroids OCPs Spironolactone Isotretinoin |
|
|
A patient is admitted to the ICU for fluid resuscitation and monitoring following trauma with significant blood loss. A central line that was inserted into the right groin emergently in the ER has been in place for a few days, and now the surrounding skin is red and warm. Also, the pt’s temp is rising, and the WBC ct is elevated. What is the likely cause?
|
Central line infection
|
|
|
A 7 yo boy is brought to the county clinic with a rash. The mother denies that the child has acted ill. The exam is unremarkable besides perioral honey-crusted lesions & regional lymphadenopathy. What can be used to tx this pt?
|
Dx: uncomplicated impetigo
Tx: washing the area, removing the crusts, topical antibiotics +/- systemic antibiotics |
|
|
A 57 yo diabetic female has a severe infection in her right foot. An open purulent wound is draining from the top of her right foot and redness extends from the toes to just above the ankle. However, she has exquisite tenderness that extends beyond the redness to midway up the leg. CT scan of the extremity shows many small air collections in the fascia overlying the muscles what treatment is needed?
|
Dx: Necrotizing fasciitis
Tx; extensive surgical debridement, possible amputation Broad spectrum antibiotics with gram (+) and Gram (-) coverage & anaerobic coverage Wound culture prior to antibiotics administration |
|
|
What tx options are available for patients with acne vulgaris?
|

|
|
|
What are the treatment options for rosacea?
|

|
|
|
What treatments are available for children with chicken pox?
|

|
|
|
What is the treatment for an uncomplicated varicella zoster outbreak in an elderly patient?
|

|
|
|
Which acne medication is known for causing photosensitivity?
|
Tetracyclines
|
|
|
What should you know about oral isotretinoin (Accutane) in the treatment of acne?
|
Usually, try 2-3 other therapies prior to using this therapy
Check β-hCG, CBC, lipids, LFTs regularly (25% develop ↑ triglycerides: >800 = risk of pancreatitis) For dry skin – moisturizing soap, lotions, Chapstick, polysporin to nares PRN, eye drops PRN Screen for depression & suicidal ideation each visit Never use with tetracycline → combined risk of pseudotumor cerebri OCPs should be prescribed to women pts due to high risk of of teratogenic side effects |
|
|
HYQ: What is the classic presentation of rosacea?
|
Middle-aged patient
Facial erythema w/ telangiectasias starting at nose & cheeks Recurrent facial flushing provoked by various stimuli: hot or spicy foods, alcohol, temp extremes, emotional reactions Inflammatory papules, pustules, cysts and/or nodules similar in appearance to acne but without comedones Ocular blepharitis, conjunctivitis, and/or keratitis Rhinophyma (sebaceous gland hyperplasia of the nose) |
|
|
What are the clinical features of varicella chicken pox?
|
Prodrome of malaise, fever, pharyngitis, headache, and myalgia for 24 hours prior to rash onset
Pruritic evolving rash: red macules → teardrop vesicles → rupture & crusting over Vesicular rash starts on face & trunk then spreads to extremities Rash appears in successive crops of vesicles over 2-4 days Most all lesions are fully crusted by 6 days Skin bacterial superinfections may occur (group A strep pyogenes) Adults may also develop pneumonia and/or encephalitis |
|
|
What medications are used in the treatment of postherpetic neuralgia?
|
Gapapentin, Pregabalin, Lidocaine patches, Capsaicin cream
|
|
|
A 15 yo girl is brought to the dermatologist for tx of her acne. What is the causative organism in acne?
|
Propionibacterium acnes
|
|
|
An elderly woman presents with a rash on her right flank. She says that the rash appeared a few days ago and followed a recent cataract surgery. The rash is causing her terrible pain. On exam the rash extends from the spine past the mid-axillary line in a dermatomal distribution. The rash is composed of grouped erythematous vesicles. What can be used to treat this patient?
|
Dx: Herpes Zoster
Tx: acyclovir, valacyclovir, famciclovir Acetominophen (tylenol) or opioid analgesia |
|
|
A 41 yo woman with rosacea is seen in the clinic. It is a mild case, for which avoidance of the triggers of facial flushing would be an initial therapy. What are some examples of things to avoid?
|
Hot/spicy drinks or food, Alcohol, Caffeine
Extremes of temperature, Exercise, Wind Skin products that irritate Extreme emotions |
|
|
A friend of yours has significant allergies this season for which his doctor has given him the following treatment, “a shot, and pills that I take decreasing doses each day for about a week.” Your friend is concerned b/c he has noticed that his face suddenly has “as many zits as I did when I was 17.” What medication was likely in the shot & the pills he is taking?
|
Dx: acne triggered by steroids
|
|
|
A 25 yo man is in the office for cold sores. On exam he has a collection of 3 small vesicles at the vermillion border. He says that they are painful. This is the second time he has had these. He says he knew he was about to get them b/c he could feel a tingly sensation at that location for a few days before the lesions appeared. What studies might be helpful to diagnose this disease?
|
Dx: HSV 1
Test: Tzanck smear |
|
|
Which HPV types cause skin warts? Genital warts?
|
Skin warts: Type 1 – 4
Genital warts: Type 6, 11 |
|
|
What are the different treatment options for condyloma acuminata (genital warts)?
|
Spontaneous regression of small asymptomatic warts within 3 months occurs about 25% of the time
Podophyllotoxin (Self-administered) – for vulvar lesions in nonpregnant women Podophyllin – for vulvar lesions in nonpregnant women Trichloroacetic acid (TCA): often 1st line therapy Imiquimod: (self administered) – for vulvar lesions in nonpregnant women, induces interferon mediated antiviral response Cryoablation with liquid nitrogen |
|
|
What are the characteristic features of tinea versicolor?
|
Pale, velvety pink (“salmon-colored”), light-brown, or whitish hypopigmented macules
Usually limited to the upper trunk & extremities Lesions do not tan Lesions do not appear scaly, but scale when scraped Miscroscopic exam reveals both hyphae & spores (“spaghetti & meatballs”) in 10% KOH prep |
|
|
What are the treatments for tinea versicolor?
|
Topical OTC antifungal for 2 weeks
Terbinafine (Lamisil) Clotrimazole (Lotrimin) Selenium sulfide (foam, solution, shampoo) qd-BID daily to affected areas for 1 week → then q1-3 weeks for prophylaxis Ketoconazole 2% shampoo daily for 3 days Oral antifungal for extensive disease: ketoconazole, fluconazole, itraconazole |
|
|
What is the treatment for onychomycosis?
|

|
|
|
What is the tx for pediculosis capitis and pediculosis pubis?
|

|
|
|
An obese, 42 yo diabetic woman c/o a pruritic rash underneath her breasts. Exam reveals an erythematous patchy rash underneath large, pendulous breasts. What diagnostic study would be helpful, and what would be seen?
|
Dx: Intertrigo (candida)
Study: KOH prep – see pseudohyphae |
|
|
A 30yo patient with a pruritic scaly lesion is evaluated. A KOH prep of the lesion shows hyphae. What oral agents are available to treat this condition in the case that it is refractory to topical treatment?
|
Dx: Dermatophyte/ tinea
Tx: one of the “azoles” (ketoconazole, fluconazole, itraconazole) |
|
|
A 13yo girl is brought to the county clinic with a rash on her wrists and hands, which becomes intensely pruritic when she bathes. On exam, the rash consists of narrow burrows and erythematous papules. What medication options are available for this rash?
|
Dx: Scabies
Tx: Primethrin Cream, Oral Ivermectin, Diphenhydramine Minimize contact, good hygiene, wash all lines & clothes in hot water |
|
|
A 22yo Asian patient comes to your office. She is concerned b/c she noticed small areas of hypopigmentation on her back. She says these areas are more noticeable in the summer. What is the organism that is likely causing her skin condition?
|
Dx: Tinea versicolor
Organism: Malassesia furfur |
|
|
When treating pediculosis with malathion, what symptoms might suggest malathion toxicity?
|
Cholinergic symptoms: lacrimation, salivation, diarrhea, muscle excitation
|
|
|
When should antibiotics be used in the tx of skin abscesses?
|
If abscess is > 5 cm
If patient is at high risk due to DM, Steroids, immunocompromised |
|
|
What medication is preferred in the tx of scabies?
|
Permethrin
|
|
|
What are the characteristic features of necrotizing fasciitis?
|
Unexplained excruciating pain in absence of cellulitis or beyond areas of cellulitis
Erythema with blistering or bullae Crepitus in the cellulitis Cellulitis of the perineum DM pt with foot cellulitis and signs of systemic toxicity |
|
|
What is the treatment for dry gangrene? Wet gangrene?
|
Dry: autoamputation or tx of vascular disease then amputation
Wet: debridement with possible amputation |
|
|
What medication options are available for the treatment of acne vulgaris?
|
1st line: topical retinoid
2nd line: benzoyl peroxide topical or oral antibiotics spironolactone OCPs Isoretinoin (Accutane) |
|
|
What is the time-frame in the treatment of varicella?
|
Need to start tx within first 72 hours
|
|
|
What side-effects can arise from the use of oral isotretinoin (Accutane)
|
Teratogenic
Drying of skin & mucous Hepatotoxicity ↑ triglycerides depression, suicidal ideation pseudotumor cerebri if given with tetracycline |
|
|
HYQ: What is the treatment of molluscum contagiosium?
|
Self-resolve
Laser or cryotherpay Imiquimod – gets the body to kill the virus itself |
|
|
What is the treatment for tinea capitis?
|
Oral Griseofulvin, Oral Itraconazole, Oral Terbinafine
|
|
|
What is the treatment for rosacea?
|
Topical sulfacetamide
Topical metronidazole Laser therapy for rhinophyma Systemic tx: tetracycline, doxycycline, minocycline, isoretinoin |
|
|
What are the characteristic features of erythema multiforme?
|
Skin lesions with a target appearance (dull red center, a pale zone, and a darker outer ring)
Lesions can take many different shapes (multiforme) Lesions develop over 10+ days: macule → vesicles/bullae in the center of the papule Common sites: hands/forearms, soles/feets, face, elbows & knees, penis & vulva Severe form (EM Major) always involves the mucus membranes → can become SJS/TEN |
|
|
What is the treatment for erythema multiforme?
|
Stop any inciting medication
Symptomatic tx with antipruritics If severe → systemic glucocorticoids (although no proven effectiveness) If patient also has h/o HSV → antiviral such as acyclovir or valacyclovir |
|
|
What is the distinction bwn Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN)?
|
SJS is the less severe form of TEN
SJS: skin sloughing (epidermal detachment) is limited to less than 10% of body surface area TEN: at least 30% of the skin is detaching there is overlap btw the two at 10-30% skin involvement |
|
|
What is the treatment for infantile seborrheic dermatitis (aka cradle crap)?
|
Selenium sulfide (Selsun Blue) shampoo 2x/wk until resolved
Massaging olive oil into the scalp and leaving for 15 min can help remove scales when washing +/- hydrocortisone 1% cream BID to affected area |
|
|
How does seborrheic dermatitis manifest in adults?
|
Erythema, scaling, and white flaking in areas of sebaceous glands including eyebrows, nasolabial folds, face, external ear, scalp, upper trunk, and body folds (axilla, groin)
|
|
|
What diseases are a/w an ↑ incidence of seborrheic dermatitis?
|
Parkinson’s, HIV, Psoriasis, immunocompromised pts (ie transplant pts)
Exacerbations are common in emotional stress & hositalizations Severe intractable SD may point to HIV infection |
|
|
What are the available tx for atopic dermatitis (aka eczema)?
|

|
|
|
What are the possible side effects of the calcineurin inhibitors (Elidel cream or Protopic ointment) in the treatment of atopic dermatitis?
|
Do not cause systemic effects or skin atrophy like topical steroids. Safe on face/ eyelids
Try to avoid in children younger than 2 years due to higher rates of URIs. However most dermatologists have no problems using these in those under 2 years b/c the alternative of using topical steroids would probably have more side effects Preliminary studies suggest possible slight ↑ in risk of lymphoma. Therefore keep duration as short as possible |
|
|
A 34 yo M is started on phenytoin to control his seizures. Shortly thereafter, he begins to have malaise, fever, headache, and a rash. On PE his skin is very red & sloughing off in some areas. How should this patient be treated?
|
Dx: Stevens Johnson Syndrome
Tx: D/c Phenytoin, give IVF & corticosteroids, analgesics Admit to burn unit, IVIG may be needed |
|
|
An infant is brought to the physician with an area of greasy scaling over part of her scalp. What recommendations can be given for this?
|
Dx: Seborrheic Dermatitis
Tx: Selenium Shampoo, Tar, ketoconazole, OTC topical hydrocortisone |
|
|
A 40yo patient has erythematous plaques covered with silver scales on his knees and elbows. He also c/o arthralgia. What do you expect to find on a skin biopsy?
|
Dx: Psoriasis
Labs: ↑ ESR & negative RF Biopsy: thickened epidermis with nucleated cells in stratum corneum, absent stratum granulosum |
|
|
A 27yo F c/o fatigue & muscle aches. She notes a recent recurrence of her cold sores. PE reveals a large plaque with a red center and perimeter but a paler inner region. What is the diagnosis, and the cause of the disease in this case? What can be given to treat her?
|
Dx: Erythema multiforme due to HSV
Tx: Acyclovir, Valacyclovir, Analgesics, corticosteroids |
|
|
What drugs are used in the treatment of Psoriasis?
|

|
|
|
What is the treatment for pityriasis rosea?
|
This is a self-limiting disease of 4-6 weeks, and no treatment is necessary. Sunlight is helpful
If significant itching, may use a moderate potency topical steroids If extensive disease or severe itching → phototherapy Possibly beneficial but unproven: Erythromycin 250mg 4x/day x 14days Acyclovir 800mg 5x/day x 7 days |
|
|
What are the characteristic features of lichen planus?
|
Skin involvement: pruritic, purple, polygonal papules and plaques that are shiny and flat and commonly occur on the flexor surface of the extremities (ie wrist)
Wickham’s striae: is a white, lacelike pattern on the surface of the papules/plaques Mucus membrane involvement: Wickham’s striae in the lateral buccal mucosa nd possible erosive lesions that may become infected with Candida Genital involvement: usually limited to violaceous papules on the glans penis in men and vulva of women |
|
|
What infections are a/w an ↑ likelihood of lichen planus?
|
Young patients: HIV
Older patients: Hepatitis C |
|
|
What is the treatment of Lichen Planus?
|
Corticosteroids of medium to high-potency – topical or intralesional (oral if topical unsuccessful)
Acitretin (or oral retinoid) |
|
|
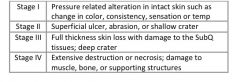
What are the different stages of decubitus ulcers?
|
|
|
|
What is the tx for the diff stages of sacral decubitus ulcers?
|

|
|
|
HY: What is the characteristic appearance of stasis dermatitis?
|
Eczematous dermatitis with inflammatory papules, scaly and crusted erosions, ↑ pigmentation, stippling with recent and old hemorrhages and possible ulceration
|
|
|
HY: What is the treatment for stasis dermatitis?
|
Compressive dressings or stocking with at leas 20-30 mmHg of pressure (usually 30-40mmHg)
Elevation of the legs above the heart whenever possible but for at least 30 min 3-4 times a day Topical steroids Consider horse chestnut seed extract – 300mg (50mg of aescin) BID esp if unwilling to wear compressive stockings Aspirin 300-325mg/day (may accelerate the healing of venous ulcers) (Treatment of ulceration from chronic venous insufficiency is not addressed here) |
|
|
A 70 yo pt has dry, scaly skin of the lower legs. It is also of a darker color than the rest of his skin. What is the pathophysiology of this disease?
|
Dx: Stasis Dermatitis
|
|
|
Target lesion
|
Erythema multiforme
|
|
|
Punctate bleeding when silvery scale is removed
|
Psoriasis
|
|
|
Christmas tree pattern rash
|
Pityriasis Rosea
|
|
|
Pruritic, dry rash of flexor surfaces
|
Eczema/ Atopic Dermatitis
|
|
|
Red plaques with silvery scale
|
Psoriasis
|
|
|
Greasy, yellow scales on scalp
|
Seborrheic Dermatitis
|
|
|
Pruritic, purple, polygonal papules and plaques
|
Lichen Planus
|
|
|
Tender erythematous pretibial nodules
|
Erythema nodosum
|
|
|
What are the 2 most important ways to both prevent and treat decubitus ulcers?
|
Maintain adequate nutrition
Relieve pressure by frequent positioning Use appropriate mattress & pillows |
|
|
A 26yo computer programmer c/o an itchy rash on his back, It started out as a single erythematous oval with a thin white scale over it. The rash then progressed and now forms a series of streaks in a roughly triangular shape on his back. The man is averse to taking medications. How can he be treated with this preference in mind?
|
Dx: Pityriasis Rosea
Self-limited disease, sunlight may help Meds: topical corticosteroids, acyclovir, erythromycin |
|
|
A 40yo woman arrives at the ER malnourished and c/o abdominal pain. She has a fever, tachycardia, and dehydration. Her skin is leathery from chronic sun exposure, but you especially notice nodules appearing on her anterior leg. The skin overlying these is reddish-purple and tender to palpation. The patient denies trauma to the area. Abdominal CT scan with constrast reveals obstruction with a string sign and skip lesions. What are the diagnoses for this patient?
|
Dx: Erythema nodosum & IBD (Crohn’s Disease)
|
|
|
A patient presents with erythema multiforme. What meds are the most common offenders?
|
Penicillins, Sulfonamides
NSAIDs Anticonvulsants OCPs |
|
|
What are the distinctions btw erythema multiforme, Stevens-Johnson Syndrome (SJS) and Toxic Epidermal Necrosis (TEN)?
|
EM: milder disease, most likely without mucous membrane involvement, no sloughing of skin
SJS: sloughing of skin < 10%, mucous membranes involved TEN: worst form, >30% of skin sloughing |
|
|
What is the classic presentation of pityriasis rosea?
|
Herald patch, followed by Christmas tree pattern rash several days later
|
|
|
What is the treatment for pityriasis rosea?
|
Self-limited, no tx needed
|
|
|
What are the clinical features of pityriasis versicolor?
|
Hypopigmented lesions with a transparent scale
KOH prep: spaghetti & meatball appearance |
|
|
What is the treatment for pityriasis versicolor?
|
Topical antifungal for 2 weeks
Ketoconazole Selenium sulfide |
|
|
What is the classic presentation of erythema nodosum?
|
Pretibial nodules (painful, erythematous)
|
|
|
What is the classic presentation of lichen planus?
|
Pruritic, Purple, Polygonal papules & plaques, Flexor surfaces & extremities
|
|
|
What is the treatment for seborrheic dermatitis?
|
Selenium sulfide, coal tar shampoo, ketoconazole shampoo
Steroids |
|
|
What are the treatment options for psoriasis?
|
Topical steroids |
|
|
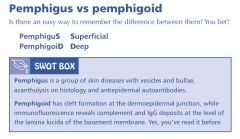
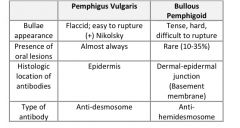
What are the distinctive features of pemphigus vulgaris & bullous pemphigoid?
|
|
|
|
What are the distinctive features of pemphigus vulgaris & bullous pemphigoid?
|
|
|
|
What is the treatment and prognosis for pemphigus vulgaris?
|
Steroids – high dose systemic (1 mg/kg/day) |
|
|
What is the treatment for bullous pemphigoid? |
steroids |
|
|
What is the classic presentation of porphyria cutanea tarda?
|
Chronic blistering lesions on sun-exposed areas of skin (usually dorsum of hands, face, forearms, legs)
Facial hypertrichosis and hyperpigmentation Pseudoscleroderma with cutaneous thickening, scarring and calcification Elevated LFTs (AST, ALT, GGT) Hepatitis C infection is common Elevated “total plasma porphyrin” |
|
|
What is the treatment for porphyria cutanea tarda?
|
Phlebotomy
Low-dose chloroquine or hydroxychloroquine Avoidance of alcohol, estrogens, iron supplements Sunscreen use |
|
|
Most common type of melanoma
|
Superficial spreading melanoma
|
|
|
Non-pigmented melanoma
|
Amelanotic melanoma
|
|
|
Dark papule on the legs or trunk that bleeds with minor trauma
|
Nodular melanoma
|
|
|
which type of melanoma occurs on palms, soles, or beneath the nail bed in pts with dark skin
|
Acral lentiginous melanoma
|
|
|
Dark lesion larger than 6mm with irregular, asymmetric borders
|
Superficial spreading melanoma
|
|
|
What do the antibodies target in bullous pemphigoid & pemphigus vulgaris?
|
PV: epidermis, anti-desmosome
BP: basement membrane, dermal-epidermal junction, anti-hemidesmosome |
|
|
Which type of melanoma:
Grows only vertically |
Nodular
|
|
|
Which type of melanoma:
Found on palms, soles and nail beds |
Acral Lentiginous
|
|
|
Which type of melanoma:
Most common type |
Superficial spreading
|
|
|
Which type of melanoma:
A longstanding precancerous lesion before dermal invasion |
Lentigo Maligna
|
|
|
Which type of melanoma:
Lateral growth occurs before vertical invasion |
Superficial spreading
|
|
|
What type of biopsy is appropriate for a pigmented skin lesion? A pale firm pearly heaped up area of epidermis? An erythematous, scaly lesion?
|
Punch or excisional, don’t use shave for pigmented lesion!
|
|
|
A hairy homeless man with blisters on the face & hands comes to the ER> Lab studies reveal elevated AST, ALT and GGT> What enzyme is deficient in this disease? What comorbid infection may also be present in this man?
|
Dx: Porphyria cutanea tarda
Deficient enzyme: Hepatic uroporphyrinogen decarboxylase Comorbid infection: Hepatitis C |
|
|
A 60 yo bald Caucasian man comes to the clinic with several reddish, sandpaper-like lesions on the top of his head each measuring less than 1 cm. How can these be treated?
|
Dx: Actinic Keratosis
Tx: topical 5-Fluorouracil, Imiquimod, Cryotherapy |
|
|
A 65yo M presents with a pearly papule with telagniectasia on the tip of his nose. What is the likely dx?
|
Dx: Basal Cell Carcinoma
|
|
|
What are the treatment options for melasma?
|
Hydroquinone (3% solution or 4% cream)
Azelaic acid 20% cream Flucinolone 0.01% + hydroquinone 4% + tretinoin 0.05% Prevention by minimizing sunlight exposure and by using an opaque sunblock (titanium dioxide or zinc oxide) |
|
|
What are the characteristic features of vitiligo?
|
Sharply demarcated patches of complete depigmentation (due to loss of melanocytes)
Borders are hyperpigmented More common at acral areas & around body orifices Skin is of normal texture (which excludes morphea & lichen sclerosus) Assoc with thyroid disease in 30% of pts (esp women) Most common at ages 20-30 |
|
|
What comorbidities are a/w vitiligo?
|
Autoimmune disorders: Graves Disease, autoimmune thyroiditis, pernicious anemia, type 1 DM, primary adrenal insufficiency, hypopituitarism, alopecia areata, autoimmune hepatitis
|
|
|
What is the treatment for vitiligo?
|

|
|
|
What treatment options are available for treating acanthosis nigricans?
|
Treat the underlying disorder which may require weight loss, discontinuation of an offending agent (ie glucocorticoids, OCPs) or identification and removal of a malignancy
Lightening agents may be used which often include Retin-A (tretinoin) and topical steroids Fish oil oral supplementation may also be used |
|
|
Purple-red on face that does not regress with age
|
Port Wine Stain
(Sturge Weber) |
|
|
Infant with bright-red lesion that regresses over mos-yrs
|
Strawberry Hemangioma
|
|
|
Benign small red papule that appears on skin with age
|
Cherry Hemangioma
|
|
|
Bright red papule with radiating blanching vessels
|
Spider angioma (Cirrhosis)
|
|
|
Blue compressible mass that does not regress
|
Cavernous Hemangioma
|
|
|
Red-pink nodule on a child that is often confused with melanoma
|
Spitz Nevis
|
|
|
What is the treatment for uncomplicated infantile hemangioma? When are infantile hemangiomas worrisome?
|
Since most uncomplicated infantile hamaniomas (aka strawberry hemangioma) gradually resolve within the first 2 years of life (or at least 10% resolution each year) observation is usually the best treatment
They are worrisome and require additional treatment (such as systemic steroids) if periorbital, in an airway, or associated with high-output heart failure |
|
|
What are the clinical features of alopecia areata?
|
Asymptomatic, non-inflammatory, non-scarring areas of complete hair loss
May be precipitated by stress Regrowth after 1st attack in 30% by 6 months, in 50% by 1 yr, in 80% by 5 years 10-30% will no re-grow hair, 5% progress to total hair loss Obtain syphilis screen, CBC, BMP, ESR, TSH, ANA (to rule out pernicious anemia, chronic active hepatitis, thyroid disease, SLE, Addison’s) R/o trichotillomania (pulling-out one’s hair) – look for broken hair shafts of different lengths, consider shaving a small patch and observe over a few weeks for growth |
|
|
What is the treatment for alopecia areata?
|

|
|
|
What is the treatment for androgenic alopecia?
|

|
|
|
What is the term for the malar hyperpigmentation that can occur during pregnancy?
|
Melasma
|
|
|
A 31yo woman has patches of hypopigmentation on her skin. Considering the associated comorbidities with this condition, what endocrine test might you order initially?
|
Dx: Vitiligo
Labs: Check TSH (Vitiligo is a/w thyroid disease in 30% of pts, esp women) |
|
|
Name the common plastic surgery procedure done for drooping eyelids
|
Blepharoplasty
|
|
|
What treatment is indicated for a newborn with an uncomplicated strawberry hemangioma on the face?
|
Usually no tx – will regress with time
|
|
|
A 30 yo woman comes to the medical clinic b/c she has noticed a few small areas of complete absence of hair on her scalp. What are some labs that would help narrow the diagnosis of the cause of this skin condition?
|
Suspect: Alopecia Areata (an idiopathic condition)
Labs (to r/o secondary causes of hair loss): VDRL, RPR, CBC, Metabolic panel, ESR, TSH, ANA, LFTs (to rule out pernicious anemia, chronic active hepatitis, thyroid disease, SLE, Addison’s) Don’t forget to ask about stress, nutrition |
|
|
What is the most imp prognostic indicator in cases of melanoma?
|
Depth of lesion
|
|
|
a/w obesity, diabetes, or malignancy (esp if over age 50)
|
Acanthosis Nigricans
|
|
|
Pigmented plaques that appear to be stuck onto the skin
|
Seborrheic Keratosis
|
|
|
Black velvety plaques on flexor surfaces and intertriginous areas
|
Acanthosis Nigricans
|
|
|
Rough lesions on sun exposed skin that are easier to feel than see
|
Actinic Keratosis (AK)
|
|
|
Circular rash with central clearing on the trunk or arms
|
Tinea Corporis
|
|
|
What is the classic appearance of basal cell cancer (BCC)?
|
Pearly papule with Telangiectasias
|
|
|
What is the classic appearance of squamous cell cancer (SCC)?
|
Papule or ulcer with scaling or keratinization
Regular or disorderly appearance Painful or painless |
|
|
What is the classic appearance of porphyria cutanea tarda?
|
Chronic blistering lesion on sun exposed areas
Hypertrichosis & hyperpigmentation of the face |
|
|
HYQ: From the presentation, how might pemphigus vulgaris be distinguishable from bullous pemphigoid?
|
PV: (+) Nikolsky sign, flaccid, sloughs easy with light pressure
BP: (-) Nikolsky sign, thick, tense, difficult to rupture |
|
|
What are the treatment options for actinic keratosis?
|
Topical 5-fluorouracil
Cryotherapy Imiquimod |
|
|
Purple-red on face that does not regress with age
|
Port Wine Stain
(Sturge Weber) |
|
|
Infant with bright-red lesion that regresses over mos-yrs
|
Strawberry Hemangioma
|
|
|
Benign small red papule that appears on skin with age
|
Cherry Hemangioma
|
|
|
Bright red papule with radiating blanching vessels
|
Spider angioma (Cirrhosis)
|
|
|
Blue compressible mass that does not regress
|
Cavernous Hemangioma
|
|
|
Red-pink nodule on a child that is often confused with melanoma
|
Spitz Nevis
|
|
|
What treatments are available for androgenic alopecia?
|
Finasteride, Minoxidil, Spironolactone
|
|
|
What are the possible underlying causes of alopecia areata?
|
Syphilis, pernicious anemia, Lupus, chronic active hepatits, thyroid disease, Addison’s
|
|
|
Q001. Ankylosing Spondylitis - What is it; Risk factors
|
A001. Chronic inflammatory disease of spine and pelvis; sacroilitis => fusion of affected joints; 20's - 30's; seronegative; HLA-B27; risk factors – male, family History
|
|
|
Q002. Ankylosing Spondylitis - History/PE
|
A002. History - hip and low back pain, worse with inactivity, worse in mornings, better with activity, thru day; PE - hip pain and stiffness; limited chest expansion; loss of lumbar lordosis; positive Schober test - decreased spine flexion; may have anterior uveitis,; 3rd degree heart block; aortic insufficiency => CHF
|
|
|
Q003. Ankylosing Spondylitis - Dx
|
A003. Dx based on clinical & XR; HLA-B27; ESR - may be elevated; RF & ANA - negative; spine and pelvic XR - "bamboo spine"
|
|
|
Q004. Ankylosing Spondylitis - Tx
|
A004. NSAIDs; exercise; physical therapy
|
|
|
Q005. Reiter's - What is it
|
A005. "Can't see, can't pee, can't climb a tree"; conjunctivitis; uveitis; urethritis; arthritis; may also have - keratoderma blennorrhagicum, circinate balanitis; after infection with – campylobacter, Shigella, salmonella, chlamydia, ureaplasma; seronegative; HLA-B27; young men
|
|
|
Q006. Psoriatic Arthritis - What is it
|
A006. Chronic inflammatory arthritis; psoriasis of skin; psoriatic nail lesions; DIP joints; sausage-shaped digits; "mushroom caps"; HLA-B27; seronegative
|
|
|
Q007. Rheumatoid Arthritis - What is it
|
A007. Chronic autoimmune diseases; peripheral joints - symmetrically inflamed; progressive destruction of articular tissue; erosion of - cartilage, bones, tendons; systemic Sxs; atlanto-axial subluxation; ruptured Baker's cyst; MC females 35-50; HLA-DR4; T cell activation - why HIV improves pre-existing
|
|
|
Q008. Rheumatoid Arthritis - History/PE |
A008. Insidious onset of morning stiffness > 1 hr; painful, warm swelling of multiple symmetric joints > 6 wks; MC - wrist, MCP, PIP, any joint may be involved; axial rare except upper cervical spine; ulnar deviation; MCP joint hypertrophy, swan-neck, boutonniere; subq, painless Baker's cysts
|
|
|
Q009. Rheumatoid Arthritis - Dx
|
A009. RF (anti-Fc IgG Ab); ESR; synovial fluid aspiration - slightly turbid, decreased viscosity, WBC 3,000-50,000 |
|
|
Q010. Rheumatoid Arthritis - Tx
|
A010. NSAIDs; COX-2 inhib; severe – corticosteroids, methotrexate, hydroxychloroquine sulfate, gold, azathioprine; operative may be necessary.
|
|
|
Q011. Felty's Triad - What is it
|
A011. RA; splenomegaly; neutropenia
|
|
|
Q012. Juvenile Rheumatoid Arthritis - What is it
|
A012. Nonmigratory, nonsuppurative, mono- and poly-arthropathy; bony destruction; < 16 y/o; lasts > 6 wks; 95% - disease resolves by puberty
|
|
|
Q013. Juvenile Rheumatoid Arthritis - History/PE
|
A013. 3 patterns; all patterns may have – fever, nodules, erythematous rashes, pericarditis, fatigue; pauciarticular - MC form, < 4 joints, weight-bearing joints; ANA type - MC subtype, asymm involvement of lg. joint, iridocyclitis – insidious, if not treated => blind; RF type - poor prognosis, HLA-B27 - boys also have spondyloarthropathies,; polyarticular - > 5 joints, similar to adult RA, symmetric, may develop iridocyclitis; Still's disease (systemic) - least common, daily high spiking fever, evanescent salmon-colored rash, hepatosplenomegaly, serositis
|
|
|
Q014. Juvenile Rheumatoid Arthritis - Dx
|
A014. No diag tests; XR; RF - positive in 15%; ANA - may be positive; RBC decreased; elevated – ESR, WBC, platelets; normal ESR doesn't exclude Dx
|
|
|
Q015. Juvenile Rheumatoid Arthritis - Tx
|
A015. NSAIDs; corticosteroids; ROM and strength exercises; methotrexate; monitor iridocyclitis
|
|
|
Q016. Scleroderma - What is it
|
A016. Progressive systemic sclerosis; multisys disease; thickening of skin from; accumulation of connective tissue; MCC of death - pulmonary; CREST - better prognosis; MC - females 30-50
|
|
|
Q017. Scleroderma - History/PE
|
A017. All have thick skin & Raynaud's; Lung - pulmonary fibrosis => restrictive lung disease and cor pulmonale; GI - esophageal dismotility, achalasia, decreased motility of small intestines, dilation of large intestines, large diverticula; renal - malignant HTN => ARF; CREST - limited form
|
|
|
Q018. CREST - What is it
|
A018. Calcinosis; Raynaud's; esoph dysmotility; sclerodactyly; telangiectasias
|
|
|
Q019. Scleroderma - Dx
|
A019. RF; ANA; eosinophilia; anticentromere Ab - CREST; anti-Scl-70 - systemic |
|
|
Q020. Scleroderma - Tx |
A020. Systemic glucocorticoids; Ca2+ channel blockers - Raynaud's; ACE inhibitor - renal disease, HTN |
|
|
Q021. SLE - What is it |
A021. Multisys autoimmune; women - especially Black; Ab-mediated cellular attack; deposits of Ag-Ab complexes; lupus-like syndrome - drug-induced lupus, Hydralazine, penicillamine, Procainamide, INH, methyldopa; rash only, anti-histone Ab, resolves when drug discont. |
|
|
Q022. SLE - History/PE
|
A022. DOPAMINE RASH; Discoid rash; Oral ulcers; Photosensitivity; Arthritis; Malar rash; Immunologic criteria; Neuro Sxs - lupus cerebritis, seizures; Elevated ESR; Renal disease; ANA positive; Serositis; Hematologic abnormalities; Sxs exacerbated - sun exposure, pregnancy
|
|
|
Q023. SLE - Dx
|
A023. Anemia; leukopenia; TCP; ANA; anti-dsDNA; anti-Sm Ab; active attacks - decreased C3 and C4; antihistone Ab - drug-induced; anti-Ro (SSA) - neonatal lupus, neonatal congenital heart block if pregnant, screen; antiphospholipid Ab – hypercoagulability, thromboembolic disease, recurrent spontan abortions, stillbirths; Tx - LMWH
|
|
|
Q024. SLE - Tx
|
A024. Arthritis - NSAIDs; major organ involvement - steroids; flare-ups - steroids; antimalarials - rash; nephritis – cytotoxics, cyclophosphamide, azathioprine
|
|
|
Q025. SLE - Complications
|
A025. Infections; progressive impairment of – brain, heart, lungs, kidney; increased risk - spontaneous abortion (antiphospholipid Ab); neonates - increased risk of congenital complete heart block (anti-Ro/SSA)
|
|
|
Q026. Temporal Arteritis - What is it
|
A026. Giant cell arteritis; women 2x's > men; > 50 y/o; subacute granulomatous inflamm; large vessels – aorta, external carotid - especially temporal, vertebral a; blindness - occlusion of central retinal; polymyalgia rheumatica - 50%
|
|
|
Q027. Temporal Arteritis - History/PE
|
A027. Headache; temporal tenderness; scalp pain; jaw claudication; fever; monocular blindness - transient or permanent; weight loss; malaise; myalgia; arthralgia
|
|
|
Q028. Temporal Arteritis - Dx
|
A028. ESR; ophthalmologic evaluation; Biopsy - temporal artery
|
|
|
Q029. Temporal Arteritis - Tx
|
A029. If suspect TA - start steroids before Biopsy; hi-dose prednisone - 1-2 mos. before taper; monitor eye exams
|
|
|
Q030. Henoch-Schönlein Purpura - What is it
|
A030. Immune-mediated vasculitis; IgA immune complexes; small arteries - GI tract; skin; joints; kidney; 2-11 y/o; degree of renal involvement; det. prognosis
|
|
|
Q031. Henoch-Schönlein Purpura - History/PE
|
A031. Palpable purpura - buttocks and legs; asymmetric, migratory; periarticular swelling; abdominal pain; preceding URI
|
|
|
Q032. Henoch-Schönlein Purpura - Tx
|
A032. Usually self-limited; Tx supportive; steroids - Sxs
|
|
|
Q033. Henoch-Schönlein Purpura - Complications
|
A033. GI bleeding; intussusception; glomerulonephritis
|
|
|
Q034. Polymyalgia Rheumatica - What is it
|
A034. Elderly females; close association with; temporal arteritis
|
|
|
Q035. Polymyalgia Rheumatica - History/PE
|
A035. Pain and stiffness – shoulder, pelvic girdle; especially severe in morning or after inactivity; minimal joint swelling; fever, malaise, weight loss; hard to - get out of chair, lift arms above head; muscles not weak; pain limits muscle effort
|
|
|
Q036. Polymyalgia Rheumatica - Dx
|
A036. Clinical; anemia; ESR high
|
|
|
Q037. Polymyalgia Rheumatica - Tx
|
A037. Low-dose prednisone
|
|
|
Q038. Inflammatory Myopathies - What Are They
|
A038. Inflammatory muscle diseases; progressive muscle weakness; polymyositis; dermatomyositis; inclusion body myositis
|
|
|
Q039. Inflammatory Myopathies - History/PE
|
A039. Difficulty with proximal muscles - lifting objects, combing hair, getting up from chair; difficulty with distal later - writing; dermatomyositis - heliotrope rash, Grottron's papules
|
|
|
Q040. Inflammatory Myopathies - Dx
|
A040. Most sensitive test - CK - elevated; aldolase - elevated; anti-jo-1 autoAb; EMG; muscle Biopsy - confirms
|
|
|
Q041. Inflammatory Myopathies - Tx
|
A041. Steroids - polymyositis; dermatomyositis; inclusion body myositis - resistant to immunosuppressives
|
|
|
Q042. Fibromyalgia - What is it
|
A042. Connective tissue d/o; myalgia; weakness; fatigue; no inflammation; associated with – depression, anxiety, IBS; MC women > 50
|
|
|
Q043. Fibromyalgia - History/PE
|
A043. Pain when palpate at least 11 of 18 tender points; palpate "trigger point"=> pain, body aches; fatigue; sleep disorders
|
|
|
Q044. Fibromyalgia - Dx
|
A044. Dx of exclusion; myofascial pain syndrome - < 11 tender points or nonfibromyalgia-associated tender points
|
|
|
Q045. Fibromyalgia - Tx
|
A045. Stretching; heat application; hydrotherapy; transcutan electrical; nerve stimulation; patient education; stress reduction; low-dose antidepressants
|
|
|
Q046. Sjogren's - What is it
|
A046. Chronic autoimmune disease; lymphocytes infiltrate exocrine glands; can become progressive => systemic => lymphoproliferative (malignant lymphome)
|
|
|
Q047. Sjogren's - History/PE
|
A047. Xerostomia; dry eyes; keratoconjunctivitis sicca; "sandy feeling under eyes"; dental caries; parotid enlargement
|
|
|
Q048. Sjogren's - Dx
|
A048. Schirmer's test - decreased tear production; rose bengal stain - corneal ulcers; anti-Ro (SSA) & anti-La (SSB); Biopsy - lymphocytes infiltrate salivary gland
|
|
|
Q049. Sjogren's - Tx
|
A049. None; symptomatic Tx - artificial tears
|
|
|
Q050. What drugs can induce SLE?
|
A050. Procainamide; Hydralazine; Isoniazid; Chlorpromazine; Methyldopa; Quinidine
|
|
|
Q051. What are the features of SLE?
|
A051. Fever, anorexia, malaise, weight loss; Butterfly rash; Nail fold infarcts; Splinter hemorrhages; Raynaud's Phenomenon
|
|
|
Q052. What is the diagnostic criteria for SLE?
|
A052. Requires 4 of 11 criteria:; Malar rash; Discoid rash; Photosensitivity; Oral ulcers; Arthritis; Serositis; Renal disorder; Seizures, psychosis; Hematologic; Immunologic; Positive ANA
|
|
|
Q053. How do you treat SLE?
|
A053. Refer to rheumatologist; NSAIDS; Antimalarial drugs; Steroids; Immunosuppressive drugs; Anticoagulation
|
|
|
Q054. What is antiphospholipid antibody syndrome?
|
A054. Recurrent venous or arterial occlusions; Recurrent fetal loss; Thrombocytopenia; Antiphospholipid antibodies; No other features of SLE
|
|
|
Q055. What is scleroderma?
|
A055. diffuse fibrosis of the skin and internal organs
|
|
|
Q056. What are the two forms of scleroderma?
|
A056. Limited - CREST; Diffuse - Renal failure, intersitial lung disease, cardiac disease
|
|
|
Q057. What is CREST syndrome?
|
A057. Calcinosis; Raynaud's syndrome; Esophageal dysmotility; Sclerodactyly; Telangiectasia
|
|
|
Q058. What are the clinical findings of scleroderma?
|
A058. Polyarthralgia, Raynaud's phenomenon; Thickened skin, with loss of normal folds; telangiectasia, pigmentation, depigmentation; Dysphagia; Restrictive lung disease; Pericarditis, heart block; Renal disease
|
|
|
Q059. What labs do you see with scleroderma?
|
A059. mild anemia; normal ESR; positive ANA; SCL-70; Anticentromere antibody (50% w/ CREST)
|
|
|
Q060. How do you treat scleroderma?
|
A060. Severe Raynaud's phenomenon - nifedipine, losartan; Esophageal reflux - H2 blockers, PPI, antacids; Bacterial overgrowth and pseudoobstruction - octreotide; Malabsorption d/t bacterial overgrowth - tetracycline
|
|
|
Q061. True or False: Prednisone is commonly used in the treatment of scleroderma.
|
A061. False
|
|
|
Q062. What is Sjogren's Syndrome?
|
A062. chronic dysfuction of exocrine glands
|
|
|
Q063. What are the clinical findings of Sjogren's Syndrome?
|
A063. keratoconjunctivitis; burning, itching, FB sensation in eye; Dry mouth; Loss of taste and smell; Parotid enlargement; Desiccation of nose, throat, larynx, vagina, skin; Dysphagia; Pancreatitis
|
|
|
Q064. What labs do you see with Sjogren's syndrome?
|
A064. Mild anemia; Leukopenia; Eosinophilia; Polyclonal hypergammaglobulinemia; Positive RF; ANA; Anti-SS-a and Anti-SS-b; Thyroid-associated autoimmunity; Schirmer test; Lip biopsy; Parotid gland biopsy
|
|
|
Q065. What does a Schirmer test measure?
|
A065. quantity of tears secreted
|
|
|
Q066. How do you treat Sjogren's syndrome?
|
A066. Supportive and symptomatic
|
|
|
Q067. What drug can relieve xerostomia?
|
A067. Pilocarpine
|
|
|
Q068. People with Sjogren's are at risk for developing what?
|
A068. lymphoma
|
|
|
Q069. What is polymyalgia rheumatica?
|
A069. pain and stiffness in neck, shoulder, and pelvic girdle
|
|
|
Q070. What are the characteristics of polymyalgia rheumatica?
|
A070. pain and stiffness in neck, shoulder, and pelvic girdle; symmetrical symptoms; more prolonged in the morning; low-grade fever, fatigue, weight loss
|
|
|
Q071. Does PMR have muscle weakness?
|
A071. No
|
|
|
Q072. What labs do you see with polymyalgia rheumatica?
|
A072. ESR and CRP elevated; Anemia and mild thrombocytosis
|
|
|
Q073. How do you treat polymyalgia rheumatica?
|
A073. Prednisone 10-20 mg/day for 6 months-2 years
|
|
|
Q074. Know about Giant Cell Arteritis.
|
A074. Symptoms; Treatment
|
|
|
Q075. What is polyarteritis nodosa?
|
A075. medium-sized necrotizing arteritis
|
|
|
Q076. What can cause polyarteritis nodosa?
|
A076. Idiopathic; Hep B or C; Drugs
|
|
|
Q077. What drugs can cause polyarteritis nodosa?
|
A077. PTU; Hydralazine; Allopurinol; Penicillamine; Sulfasalazine
|
|
|
Q078. What are the signs and symptoms of polyarteritis nodosa?
|
A078. fever, malaise, weight loss; pain in extremities; Foot drop; livedo reticularis; HTN
|
|
|
Q079. What labs do you see in polyarteritis nodosa?
|
A079. anemia; elevated ESR; Leukocytosis; Hep B or C
|
|
|
Q080. How do you confirm a diagnosis of polyarteritis nodosa?
|
A080. tissue biopsy
|
|
|
Q081. How do you treat polyarteritis nodosa?
|
A081. corticosteroids (up to 60mg/day); immunosuppressive agents (cyclophosphamide); refer to rheumatologist
|
|
|
Q082. What is a complication of polyarteritis nodosa?
|
A082. mesenteric vasculitis
|
|
|
Q083. What is Reiter's syndrome?
|
A083. Reactive arthritis
|
|
|
Q084. What causes Reiter's syndrome?
|
A084. dysentery - Shigella, Salmonella, Yersinia, Campylobacter; STD - Chlamydia
|
|
|
Q085. What are the clinical findings of Reiter's syndrome?
|
A085. Urethritis; Conjunctivitis; Mucocutaneous lesions; Aseptic arthritis; Fever, weight loss; Aortic regurgitation
|
|
|
Q086. With Reiter's syndrome, what do you see on x-ray?
|
A086. permanent or progressive joint disease (sacroiliac or peripheral joints)
|
|
|
Q087. How do you treat Reiter's syndrome?
|
A087. NSAIDS; antibiotics at time of infection; tetracycline; sulfasalazine; methotrexate; anti-TNF agents
|
|
|
Q088. True or False: Once symptoms of Reiter's syndrome develop, antibiotics can reduce the severity of the disease.
|
A088. False
|
|
|
Q089. Sjogren's si/sx
|
A089. triad - keratoconjuctivitis sicca, xerostomia, arthritis; also, pancreatitis, fibrinous pericarditis
|
|
|
Q090. Sjogren's labs
|
A090. + ANA, antiRo/antiLa abs, 70% RF +; a/w HLA-DR3
|
|
|
Q091. Behcet's si/sx
|
A091. 20 yo; oral/genital ulcers; uveitis, arthritis, other derm disease
|
|
|
Q092. Dermatomyositis si/sx
|
A092. young kids, old peeps; symmetric weakness of proximal muscles (can see dysphonia/dysphagia) look for trouble getting out of chair. skin involvement = heliotrope rash around eyes + periorbital edema
|
|
|
Q093. Dermatomyositis labs
|
A093. high ESR, high CPK, abnormal EMG, muscle biopsy --> inflammation + ANA
|
|
|
Q094. Kawasaki's si/sx
|
A094. <5 yo; truncal rash, fever >104x(>5d), conjunctival injection, cervical LAD, strawberry tongue, skin desquamation. -> coronary vessel vasculitis, aneurysms, MI
|
|
|
Q095. Kawasaki Tx
|
A095. NOT STEROIDS; aspirin + IVIG
|
|
|
Q096. Polyarteritis nodosa si/sx
|
A096. Associated with hepatitis B + cryoglobulinemia; fever, abdominal pain, weight loss, renal disorder, peripheral neuropathies.
|
|
|
Q097. Polyarteritis nodosa labs
|
A097. high ESR, leukocytosis, anemia, hematuria/proteinuria. Biopsy of medium-sized vessels --> vasculitis
|
|
|
Q098. Scleroderma si/sx
|
A098. C - calcinosis; R - raynaud's; E - esophageal dysmotility; S - sclerodactyly; T- telangectasia; heartburn, mask-like leathery facies.
|
|
|
Q099. Scleroderma labs
|
A099. Positive ANA; positive anticentromere Abs = CREST; positive antitopoisomerase = scleroderma
|
|
|
Q100. What drugs can cause secondary SLE?
|
A100. procainamide; hydralazine; dilantin (phenytoin); sulfanomide; INH
|
|
|
Q101. What is the dx lab in secondary SLE?
|
A101. Positive antihistone Abs
|
|
|
Q102. What are the dx labs in SLE?
|
A102. Positive ANA screen; positive antiSm or anti-ds-DNA
|
|
|
Q103. What are other lab findings in SLE?
|
A103. false positive for VDRL or RPR for syphilis; PTT falsely elevated; (SLE actually thrombogenic)
|
|
|
Q104. Takayasu's arteritis si/sx
|
A104. East Asian women 15-30yo; "pulseless" in 1 or both arms. carotid involve --> neuro sign, stroke; CHF
|
|
|
Q105. Wegener's granulomatosis si/sx
|
A105. old peep; nose bleeds, nasal perforation, hemoptysis, dyspnea, hematuria, ARF
|
|
|
Q106. What's the diff between Wegener's and Goodpasture?
|
A106. Weg = old peep, +ANCA; Goodpasture = young peep, positive antiglomerular antibody
|
|
|
Q107. Polymyalgia Rheumatica si/sx
|
A107. Women >50yo; Pectoral and pelvic girdles, neck involvement; a/w temporal arteritis
|
|
|
Q108. Polymyalgia Rheumatica labs
|
A108. Really high ESR; normal muscle biopsy/EMG
|
|
|
Q109. Rheumatoid factor
|
A109. It is an antibody against the Fc portion of IgG = RF & IgG form immune complexes. which is itself an antibody, IgM or IgA type.
|
|
|
Q110. RF or RhF positive in:; is often determined in patients suspected in any form of arthritis
|
A110. High levels RF: generally > 20 IU/mL; rheumatoid arthritis: present in 80%; Sjögren's syndrome: present in 60%
|
|
|
Q111. false (+) RF or RhF; Blood test performed in patients with suspected rheumatoid arthritis (RA)
|
A111. Chronic hepatitis; Any chronic viral infection; Leukemia; Dermatomyositis; Infectious mononucleosis; Scleroderma; Systemic lupus erythematosus (SLE)
|
|
|
Q112. Sjögren's syndrome; * antibodies to Ro(SSA) or La(SSB) antigens, or both; * > 40 years old at the time of diagnosis & Woman >> Man
|
A112. an autoimmune disorder in which immune cells attack and destroy the exocrine glands that produce tears and saliva with Schirmer test(+); A lip biopsy can reveal lymphocytes clustered around salivary gland
|
|
|
Q113. Spondyloarthropathies
|
A113. Group of related INFLAMMATORY JOINT Ds associated with the MHC class I molecule HLA-B27
|
|
|
Q114. Seronegative spondylarthropathy
|
A114. Spondylarthropathy & (-)rheumatoid factor (RhF)
|
|
|
Q115. Non-specific spondylarthropathy
|
A115. Indicator of other rheumatological disease (in particular rheumatoid arthritis)
|
|
|
Q116. Subgroups (with increased HLA-B27 frequency)
|
A116. ankylosing spondylitis Caucasians (AS, 92%),; ankylosing spondylitis African-Americans (AS, 50%),; reactive arthritis (Reiter's syndrome) (RS, 60-80%),; enteropathic arthritis associated with inflammatory bowel disease (IBD, 60%),; Psoriatic arthritis (60%),; isolated acute anterior uveitis (AAU, iritis or iridocyclitis, 50%), and; undifferentiated SpA (USpA, 20-25%).
|
|
|
Q117. Buergers
|
A117. thromboangiitis obliterans;; idiopathic, segmental, thrombosing vasculitis of intermed/small peripheral arteries and veins; seen in heavy smokers (tx- stop smoking)
|
|
|
Q118. Buerger's findings
|
A118. intermittent claudication, superficial nodular phlebitis, cold sensitivity, pain
|
|
|
Q119. Takayasu's arteritis
|
A119. pulseless disease;; granulomatous thickening of aortic arch and/or proximal great vessels;; associated with elevated ESR; primarily affects Asian females < 40 y/o
|
|
|
Q120. Takayasu's sxs
|
A120. fever,; arthritis,; night sweats,; myalgia,; skin nodules,; ocular disturbances,; weak pulses in upper extremities
|
|
|
Q121. Temporal arteritis (giant cell)
|
A121. most common vasculitis that affects medium and small arteries, usually branches of carotid; focal, granulomatous; unilateral HA, jaw claudication, impaired vision (occlusion of opthalmic artery- blindness); half of patients have systemic involvement and polymyalgia rheumatica; elevated ESR
|
|
|
Q122. Temporal arteritis treatment
|
A122. steroids
|
|
|
Q123. young male smoker
|
A123. buergers
|
|
|
Q124. young asian female with weak pulses in upper extremities
|
A124. takayasus
|
|
|
Q125. PAN
|
A125. necrotizing immune complex inflammation of medium sized muscular arteries typically involving renal and visceral vessels; sxs: weight loss, malaise, fever, abdominal pain, melena, HA, myalgia, HTN, neuro dysfunction, cutaneous eruptions
|
|
|
Q126. PAN association
|
A126. hep B;; multiple aneurysms and constrictions on arteriogram; not associated with ANCA (P maybe)
|
|
|
Q127. Tx of PAN
|
A127. corticosteroids, cyclophosphamide (hemorrhagic cystitis)
|
|
|
Q128. Wegener's granulomatosis
|
A128. traid of focal necrotizing vasculitis,; necrotizing granulomas in the lung and upper airway and necrotizing GN
|
|
|
Q129. Wegener's sxs
|
A129. perforation of nasal septum,; chronic sinusitis,; otitis media,; mastoiditis,; cough,; dyspnea,; hemoptysis,; hematuria; looks like goodpastures but upper respiratory tract is also involved
|
|
|
Q130. findings in wegeners
|
A130. CANCA,; CXR- may reveal large nodular densities,; hematuria and red cell casts; tx: cyclophosphamide, corticosteroids
|
|
|
Q131. Churg Strauss
|
A131. granulamatous vasculitis with eosinophilia;; involves lung, heart, skin, kidneys, and nerves; often seen in atopic pts; tx: steroids
|
|
|
Q132. Kawasaki's disease
|
A132. acute, self limiting disease of infants and kids;; acute necrotizing vasculitis of small/medium sized vessels; fever, congested conjunctiva, changes in lips/oral mucosa,; LAD, may develop coronary aneurysms,; skin rash,; strawberry tongue; tx: high dose aspirin
|
|
|
Q133. HSP
|
A133. most common childhood vasculitis;; skin rash (palpable purpura) below legs,; arthralgia,; intestinal hemorrhage,; abdominal pain,; melena
|
|
|
Q134. telangiectasia
|
A134. AV malformation in small vessels;; looks like dilated capillary; hereditary hemorrhagic telangiectasia-AD inheritance; presents with nosebleeds and skin discolorations
|
|
|
Q135. What is arthrocentesis?
|
A135. Arthrocentesis is a needle aspirate of synovial fluid for microscopic analysis. The cell count is the most accurate way of telling immediately if there is an infection versus inflammation. Counts from 0 to 2,000 are normal; from 2,000 to 20,000 are from inflammatory disorders such as gout. Counts above 50,000 are from infections. Counts between 20,000 and 50,000 are indeterminate.
|
|
|
Q136. Anti-Scl-70
|
A136. Scleroderma
|
|
|
Q137. Anti- Microsomal; (2)
|
A137. 1. Hashimoto's; 2. Autoimmune Hepatitis
|
|
|
Q138. Anti-b islet cell
|
A138. IDDM; type I diabetes
|
|
|
Q139. Anti-Acetylcholine receptor
|
A139. Myasthenia gravis
|
|
|
Q140. Anti-Adrenal
|
A140. Addison's
|
|
|
Q141. Anti-Basement membrane
|
A141. Goodpasture's
|
|
|
Q142. Anti-Centromere
|
A142. CREST
|
|
|
Q143. Anti-ds DNA
|
A143. SLE [specific]
|
|
|
Q144. Anti-Epithelial
|
A144. Pemphigus vulgaris
|
|
|
Q145. Anti-Gliadin
|
A145. Celiac disease
|
|
|
Q146. Anti-Histone
|
A146. Drug induced lupus
|
|
|
Q147. Anti-IgM
|
A147. Rheumatoid arthritis
|
|
|
Q148. Anti-Intrinsic Factor
|
A148. Pernicious anemia
|
|
|
Q149. Anti-Mitochondrial
|
A149. Primary biliary cirrhosis
|
|
|
Q150. Anti-Neutrophil
|
A150. Vasculitis
|
|
|
Q151. c-ANCA
|
A151. Wegener's granulomatosis
|
|
|
Q152. p-ANCA
|
A152. Polyarteritis nodosa
|
|
|
Q153. Anti-Nuclear
|
A153. SLE
|
|
|
Q154. Anti-Thyroglobulin
|
A154. Hashimoto's
|
|
|
Q155. Anti-Thyroid peroxidase
|
A155. Hashimoto's
|
|
|
Q156. Anti-TSH receptor; (2)
|
A156. Graves' or Hashimoto's
|
|
|
Q157. Anti-Jo-1
|
A157. Polymyositis;; dermatomyositis
|
|
|
Q158. Anti-parietal cell
|
A158. Pernicious anemia
|
|
|
Q159. Anti-platelets
|
A159. ITP
|
|
|
Q160. Anti-smith
|
A160. SLE
|
|
|
Q161. B27
|
A161. PAIR; Psoriasis,; Ankylosing spondylitis,; Inflammatory bowel diseas,; Reiter's syndrome
|
|
|
Q162. B8
|
A162. Graves Disease, Celiac Sprue
|
|
|
Q163. DR2
|
A163. Mulitple sclerosis,; hay fever,; SLE,; Goodpastures
|
|
|
Q164. DR3
|
A164. DM Type 1
|
|
|
Q165. DR4
|
A165. Rheumatoid Arthritis, DM Type 1
|
|
|
Q166. DR5
|
A166. Pernicious anemia = B12 deficiency,; Hashimoto's thyroiditis
|
|
|
Q167. DR7 |
A167. Steroid-responsive nephrotic syndrome |
|
|
Q168. Compartment Syndrome - What is it |
A168. Increased pressure in a confined space; compromises nerve, muscle & soft tissue perfusion; MC - ant. compartment of lower leg & forearm; causes – fractures, crush injuries, burns, ischemic- reperfusion after an injury, casts
|
|
|
Q169. Compartment Syndrome - History/PE |
A169. The 6 P's:; Paresthesias; Palpation - tense compartment; Pallor; Poikilothermia; Pulselessness; Paralysis; Pain - out of proportion with passive motion of fingers & toes; Volkmann's contracture |
|
|
Q170. Compartment Syndrome - Dx
|
A170. Measure compartment pressure - > 30 mmHg not good; delta pressure - diastolic minus compartment; should be > 30 to be OK
|
|
|
Q171. Compartment Syndrome - Tx
|
A171. Surgical emergency; immediate fasciotomy of all compartments; do in < 6 hrs.
|
|
|
Q172. Low Back Pain - What is it
|
A172. Paraspinous; strains - muscle injury; sprain - ligament injury
|
|
|
Q173. Low Back Pain - History/PE
|
A173. If malignancy - pain worse at night; pain not relieved by rest; pain not relieved by changing positions; if point tenderness over vertebral body – osteomyelitis, fracture, malignancy; cauda equina syndrome - bladder or bowel dysfunction, saddle-area anesthesia, impotence, surgical emergency
|
|
|
Q174. Low Back Pain - L4 Associated Deficits:; Motor; Reflex; Sensory
|
A174. Motor - foot dorsiflexion, tibialis anterior; reflex - patellar; sensory - medial aspect of leg
|
|
|
Q175. Low Back Pain - L5 Associated Deficits:; Motor; Reflex; Sensory
|
A175. Motor - big toe dorsiflexion, extensor hallucis longus; reflex - none; sensory - medial forefoot & lateral aspect of leg
|
|
|
Q176. Low Back Pain - S1 Associated Deficits:; Motor; Reflex; Sensory
|
A176. Motor - foot eversion; peroneus longus/brevis; reflex - achilles; sensory - lateral foot
|
|
|
Q177. Low Back Pain - Dx
|
A177. Mainly clinical; XR; MRI; electrodiagnostic studies - nerve conduction velocity test
|
|
|
Q178. Low Back Pain - Tx
|
A178. Sprains & strains - NSAIDs; physical therapy; continue activities as tolerated; rest > 1-3 days unnecessary. 90% recover spontaneously in 6 weeks; surgery - if correctable spinal disease, cauda equina syndrome - surgical emergency: immediate decompression, laminectomy
|
|
|
Q179. Herniated Disk - What is it
|
A179. Nucleus pulposus herniates posteriorly => nerve root or cord compression; neck/back pain; sensory & motor deficits; causes - degenerative changes, trauma, neck/back strain, neck/back sprain; middle-aged & older men after strenuous activity; L4-L5 & L5-S1
|
|
|
Q180. Herniated Disk - History/PE
|
A180. Several months of aching pain => sudden onset of severe, electricity-like LBP; pain exacerbated by straining; sciatica: tingling - lower extremities, numbness, muscle weakness, atrophy, contractions, spasms, pain increased by - passive straight leg, crossed straight leg raises, large midline herniations => cauda equina syndrome
|
|
|
Q181. Herniated Disk - Dx
|
A181. MRI
|
|
|
Q182. Herniated Disk - Tx
|
A182. Most cases - bed rest; NSAIDs; physical therapy; localized heat; resolved in 2-3 weeks; if no neuro deficit - bed rest not advised, early mobilization; muscle relaxant, NSAIDs; diskectomy - if persistent or disabling Sxs
|
|
|
Q183. Spinal Stenosis - What is it
|
A183. Stenosis of cervical or lumbar spinal canal => compression of nerve roots; usually from degenerative joint disease; middle-aged or elderly
|
|
|
Q184. Spinal Stenosis - History/PE
|
A184. Neck pain; back pain - radiates to butt & legs, leg numbness, leg weakness, "spaghetti legs", "walks like a drunken sailor"; leg cramping - at rest, standing, walking; sitting gives relief; leaning forward gives relief (flexing at hips decreased pain)
|
|
|
Q185. Spinal Stenosis - Dx
|
A185. XR; MRI or CT
|
|
|
Q186. Spinal Stenosis - Tx
|
A186. Mild to moderate - NSAIDs; abdominal muscle strengthening; advanced - epidural steroid injection; surgical laminectomy - short-term, will recur
|
|
|
Q187. Developmental Dysplasia of Hip; What is it
|
A187. Congenital hip dislocation => dislocated femoral heads due to - lax musculature; excessive uterine packing (breech) => poor development of acetabulum, hip; will progress if not corrected; MC - 1st born breech females
|
|
|
Q188. Developmental Dysplasia of Hip; History/PE
|
A188. Barlow's - hip adducted; Ortolani's - thighs abducted; Allis' (Galeazzi's) sign - knees unequal when hip & knees flexed, dislocated side is lower; asymmetrical skin folds; limited abduction of affected hip
|
|
|
Q189. Developmental Dysplasia of Hip; Dx
|
A189. Early detection; evaluate clinical; US - if after 10 weeks old; XR - unreliable until 4 mos. old, neonatal femoral head radiolucent
|
|
|
Q190. Developmental Dysplasia of Hip; Tx
|
A190. Start Tx early; < 6 mos. - Pavlik harness; 6-15 mos. - spica cast; 15-24 mos. - open reduction; if no Tx started by 24 mos. - significant defect
|
|
|
Q191. Developmental Dysplasia of Hip; Complications
|
A191. Complications - joint contractures; AVN of femoral head
|
|
|
Q192. Limp - What is it
|
A192. 1 of the MC musculoskeletal disorder of kids; MC cause - trauma
|
|
|
Q193. Limp - History/PE
|
A193. May be associated with pain or fever; ask about - history of trauma, recent infections, contact with TB- positive patients; young kids & toddlers - infected joint; adolescent & teens – JRA, slipped capital femoral epiphyses (SCFE), Legg-Calve-Perthes (LCP); disruption in normal gait – Trendelenburg, antalgic gait; infection – erythema, edema, limited ROM; trauma or tumor - point tenderness; always evaluate for – fever, signs of systemic infection, neuro involvement – reflexes, muscle atrophy, changes in sensation, bowel & bladder function
|
|
|
Q194. Limp - Differential Dx
|
A194. STARTSS HOTT; Septic joint; Tumor; Avascular necrosis (LCP); RA/JRA; TB; Sickle cell disease; SCFE; HSP; Osteomyelitis; Trauma; Toxic synovitis
|
|
|
Q195. Limp - Dx
|
A195. Thorough H&P; XR; CBC; ESR; CRP; bone scan; nerve conduction studies; joint aspirate & culture - if suspect septic joint
|
|
|
Q196. Limp - Tx
|
A196. Depends on cause
|
|
|
Q197. Legg-Calve-Perthes - What is it
|
A197. AVN of femoral head; UNK etiology; boys 4-10; can be bilateral
|
|
|
Q198. Legg-Calve-Perthes - History/PE
|
A198. Usually asymptomatic at first => painless limp or => pain, referred to knee; limited abduction; limited internal rotation; atrophy
|
|
|
Q199. Legg-Calve-Perthes - Tx
|
A199. Self-limited; observation; if disease extensive or ROM impaired – brace, hip abduction with Petrie cast, osteotomy; prognosis dependent on – age, ROM, extent of involvement, joint stability
|
|
|
Q200. Slipped Capital; Femoral Epiphysis - What is it
|
A200. Separation of proximal femoral epiphysis through growth plate => fem head displaced; medial & posterior to fem neck; can be bilateral; obese Black 11-13 y/o boys; if < 11 y/o, may be associated with endocrinopathies; may be due to imbalance between GH & sex hormones
|
|
|
Q201. Slipped Capital; Femoral Epiphysis - History/PE
|
A201. Thigh or knee pain; painful limp; acute or insidious; acute - restricted ROM, inability to bear weight. limited internal rotation; limited abduction; hip tenderness; flexion => obligatory external rotation
|
|
|
Q202. Slipped Capital; Femoral Epiphysis - Dx
|
A202. TSH; XR both hips – AP, frog-leg lat
|
|
|
Q203. Slipped Capital; Femoral Epiphysis - Tx
|
A203. Start promptly; no weight on limb until; surgical stabilized with screws; acute slip - gentle closed reduction
|
|
|
Q204. Slipped Capital; Femoral Epiphysis - Complications
|
A204. Chondrolysis; AVN of fem head; premature hip OA => hip arthroplasty
|
|
|
Q205. Shoulder Dislocation - Mechanics
|
A205. MC - anterior dislocation, axillary artery & nerve, hold arm in external. rotation; posterior dislocations, radial artery, seizures & electrocutions, hold arm in int. rotation
|
|
|
Q206. Shoulder Dislocation - Tx
|
A206. Closed reduction; followed by sling & swath; recurrent - surgery
|
|
|
Q207. Hip Dislocation - Mechanics
|
A207. MC - posterior dislocation, compress sciatic nerve., can cause AVN, posterior directed force on, internal rotated, flexed, adducted hip, "dashboard injury"; anterior dislocation - obturator nerve compromises.
|
|
|
Q208. Hip Dislocation - Tx
|
A208. Closed reduction followed by abduction; pillow/bracing; CT after reduction
|
|
|
Q209. Colles' Fracture - Mechanics
|
A209. MC wrist fracture; distal radius; fall onto outstretched hand => dorsally displaced/angle Fracture; common in elderly (osteoporosis), kids
|
|
|
Q210. Colles' Fracture - Tx
|
A210. Closed reduction; then long arm cast; intra-articular - open reduction
|
|
|
Q211. Scaphoid (Carpal Navicular) Fracture; Mechanics
|
A211. MC fractured carpal bone; can be 1-2 weeks for XR to show; assume if tenderness in anatomical snuff box; proximal 3rd scaphoid fractures can => AVN
|
|
|
Q212. Scaphoid (Carpal Navicular) Fracture; Tx
|
A212. Thumb spica cast; open reduction - displacement; nonunion common
|
|
|
Q213. Boxer's Fracture - Mechanics
|
A213. Fracture of 5th metacarpal neck; forward trauma of closed fist
|
|
|
Q214. Boxer's Fracture - Tx
|
A214. Closed reduction & ulnar gutter splint; excessive angulation - percutan pinning; skin broken - assume infection by human oral pathogens; "fight bite"; surgical irrigation; debridement; IV Antibiotics to cover Eikenella
|
|
|
Q215. Humerus Fracture - Mechanics
|
A215. Direct trauma; radial nerve. wrist drop; loss of thumb abduction
|
|
|
Q216. Humerus Fracture - Tx
|
A216. Hanging arm cast or coaptation splint & sling; functional bracing
|
|
|
Q217. Nightstick Fracture - Mechanics
|
A217. Ulna shaft fracture; from self-defense - arm against blunt object
|
|
|
Q218. Nightstick Fracture - Tx
|
A218. ORIF; open reduction & int. fixation
|
|
|
Q219. Monteggia's Fracture - Mechanics
|
A219. Diaphyseal Fracture; proximal ulnar; subluxation of radial head
|
|
|
Q220. Monteggia's Fracture - Tx
|
A220. ORIF - shaft fracture; closed reduction - radial head
|
|
|
Q221. Galeazzi's Fracture - Mechanics
|
A221. Diaphyseal Fracture; radius; dislocation of distal radioulnar joint; from direct blow to radius
|
|
|
Q222. Galeazzi's Fracture - Tx
|
A222. ORIF - radius; cast forearm in supination
|
|
|
Q223. Hip Fracture - Mechanics
|
A223. MC in osteoporotic women who fall; shortened, ext rotated leg; at risk for DVTs; displaced fem neck fractures - high risk of AVN, fracture nonunion
|
|
|
Q224. Hip Fracture - Tx
|
A224. ORIF; parallel pinning of femoral neck; anticoagulant; > 80 y/o - may need hip hemiarthroplasty
|
|
|
Q225. Femur Fracture - Mechanics
|
A225. Direct trauma (MVA); fat emboli; fever; scleral & axillary petechiae; confusion; dyspnea; hypoxia
|
|
|
Q226. Femur Fracture - Tx
|
A226. Intramedullary nailing; open fractures - thorough irrigation; debridement
|
|
|
Q227. Tibial Fracture - Mechanics
|
A227. Direct trauma; car bumper & pedestrian injury; compartment syndrome
|
|
|
Q228. Tibial Fracture - Tx
|
A228. Casting vs. intramedullary nailing
|
|
|
Q229. Open Fracture - Mechanics
|
A229. Orthopedic emergency; must go to OR in < 6 hrs. (risk of infection)
|
|
|
Q230. Open Fracture - Tx
|
A230. OR emergently to repair; Antibiotics
|
|
|
Q231. Achilles Tendon Rupture - Mechanics
|
A231. MC in unfit men in sports; hear sudden "pop"; sounds like rifle shot; limited plantar flexion; pos Thompson test - pressure on gastrocnemius; doesn't => ft plantar flexion
|
|
|
Q232. Achilles Tendon Rupture - Tx
|
A232. Long-leg cast for 6 wks
|
|
|
Q233. ACL Injury - Mechanics
|
A233. From forced hyperflexion; positive anterior drawer sign; Lachman's test; rule out meniscal or MCL injury
|
|
|
Q234. ACL Injury - Tx
|
A234. Surgery; graft from patellar or hamstring tendons
|
|
|
Q235. PCL Injury - Mechanics
|
A235. From forced hyperextension; positive posterior drawer test
|
|
|
Q236. PCL Injury - Tx
|
A236. Operative PCL repair - for highly competitive athlete
|
|
|
Q237. Meniscal Tears - Mechanics
|
A237. Clicking or locking; joint line tenderness; positive McMurray's test
|
|
|
Q238. Meniscal Tears,; MCL/LCL Injuries - Tx
|
A238. Conservative; unless associated with Sxs or ligament injuries
|
|
|
Q239. Clavicular Fracture - What is it
|
A239. MC fractured long bone in kids; birth-related (lg infants); brachial n. palsies; usually middle 3rd of clavicle; proximal end displaced superiorly; from pull of sternocleidomast
|
|
|
Q240. Clavicular Fracture - Tx
|
A240. Figure-of-8 sling vs. arm sling
|
|
|
Q241. Greenstick Fracture - What is it
|
A241. Incomplete fracture; cortex of one side of bone
|
|
|
Q242. Greenstick Fracture - Tx
|
A242. Reduction with casting; order films at 7-10 days
|
|
|
Q243. Nursemaid's Elbow - What is it
|
A243. Radial head subluxation; from being pulled or lifted by hand; kid will not bend elbow
|
|
|
Q244. Nursemaid's Elbow - Tx
|
A244. Manual reduction - gentle supination of elbow; at 90 degrees of flexion; no immobilization necessary.
|
|
|
Q245. Torus Fracture - What is it
|
A245. Buckling of cortex of long bone; secondary to trauma; usually distal radius or ulna
|
|
|
Q246. Torus Fracture - Tx
|
A246. Cast immobilization; 3-5 wks - dep. on age
|
|
|
Q247. Supracondylar Humerus Fracture - What is it
|
A247. 5-8 y/o; proximal to brachial a. risk of Volkmann's contracture
|
|
|
Q248. Supracondylar Humerus Fracture - Tx
|
A248. Cast immobilization; closed reduction; percutan pinning - if significant displaced
|
|
|
Q249. Osgood-Schlatter Disease - What is it
|
A249. Overuse apophysitis of tibial tubercle; localized pain; especially with quadriceps Ctx; active young boys
|
|
|
Q250. Osgood-Schlatter Disease - Tx
|
A250. Decreased activity 1-2 yrs; neoprene brace
|
|
|
Q251. Salter-Harris Fractures - What are they
|
A251. Fractures of growth plate of kids; classified by fracture location; I - physis; II - metaphysis & physis; III - epiphysis & physis; IV - epi-, meta- & physis; V - crush injury of physis
|
|
|
Q252. Salter-Harris Fractures - Tx
|
A252. I & II - nonoperatively; others & unstable fractures-operatively; prevents leg-length inequality
|
|
|
Q253. Osteosarcoma - What is it
|
A253. 2nd MC primary malignant; bone tumor; metaphyses - distal femur; proximal tibia; proximal humerus; can metas to lungs; men; 20s-30s; Paget's can precede development of secondary osteosarcoma
|
|
|
Q254. Osteosarcoma - History/PE
|
A254. Progressive pain => intractable pain; worse at night; constitutional Sxs; at site of tumor - erythema; enlargement
|
|
|
Q255. Osteosarcoma - Dx
|
A255. MRI; CT; XR - Codman's triangle, sunburst pattern
|
|
|
Q256. Osteosarcoma - Tx
|
A256. Limb-sparing surgical proc; pre- and postop chemo – methotrexate, doxorubicin, cisplatin, ifosfamide; amputation - may be necessary if big
|
|
|
Q257. Paget's (Osteitis Deformans) - What is it
|
A257. Osteoclasts accelerate bone turnover in local areas => hyper osteoblastic repair => abnorm structure that weakens bone; may be associated with paramyxovirus infection; mainly disease of elderly
|
|
|
Q258. Paget's (Osteitis Deformans) - History/PE
|
A258. Often asymptomatic; if Sx occur, develop insidiously; deep bone pain; bone softening => tibial bowing, kyphosis, freq fractures; increased in cranial diameter - (frontal bossing); deafness - CN8 compressed
|
|
|
Q259. Paget's (Osteitis Deformans) - Dx
|
A259. Alkaline phosphatase; increased urinary hydroxyproline; serum Ca2+ & phosphate- normal; XR - bony cortex very expanded, jigsaw/mosaic bone pattern, thick trabeculae
|
|
|
Q260. Paget's (Osteitis Deformans) - Tx
|
A260. NSAIDs; calcitonin; alendronate
|
|
|
Q261. Paget's (Osteitis Deformans) - Complications
|
A261. Fracture; hi-output cardiac failure; arthritis; deafness; secondary osteosarcoma; vertebral collapse => spinal cord compression
|
|
|
Q262. Gout - What is it
|
A262. Recurrent attacks - acute monoarticular arthritis; monosodium urate crystals; middle-aged, obese men, Pacific Islanders; hyperuricemia - secondary to uric acid underexcretion; other causes - Lesch-Nyhan, diuretics (furosemide, HCTZ), trauma, surgery, infections, steroid withdrawal, cyclosporine, malignancy, excessive red meat or red wine, hemoglobinopathies
|
|
|
Q263. Pseudogout - What is it; Dx; Tx
|
A263. MC - elderly or preexisting joint damage; if < 50 y/o - metabolic abnorm, hyperparathyroidism, hypophosphatasia, hypomagnesemia, hemochromatosis; knee - #1, also ankle, wrist, shoulder; Dx - fluid aspiration, Positive birefringent rhomboid crystals; XR - chondrocalcinosis; Tx - same as gout; low dose of colchicine - prevents recurrence
|
|
|
Q264. Gout - History/PE
|
A264. 1st episode - awakened from sleep; sudden onset of joint pain; podagra; usually 1st MTP joint, knee, ankle, DIP & PIP; joint – erythematous, swollen, tender; as becomes chronic - multiple joints involved; urate crystals deposited in connective tissue (tophi), kidneys
|
|
|
Q265. Gout - Dx
|
A265. Joint-fluid aspirate - needle-shaped, negative birefringent crystals; yeLLow when paraLLel to condenser; increased WBC; advanced - "rat bite" = punched-out erosions - of long- standing tophus, "overhanging margin"
|
|
|
Q266. Gout - Tx
|
A266. Acute - decrease inflammation; NSAIDs (indomethacin); IV colchicine or steroids - if elderly maintenance - decrease uric acid level:; probenecid if underexcrete, inhibits reabsorb of uric acid; allopurinol if overproduce or have RF or have kidney stones, can precipitate acute attack
|
|
|
Q267. Osteoarthritis - What is it; Risk Factors
|
A267. Degen joint disease; deterioration of articular cartilage of moveable, weight- bearing joints; MCC- idiopathic; secondary - any diseases that causes stress or trauma to joint; knee OA - MCC of chronic disability in elderly in West; risk factors – obesity, family History, history of joint trauma; especially intra-articular fractures, repetitive stress
|
|
|
Q268. Osteoarthritis - History/PE
|
A268. History - joint stiffness - insidious onset; pain - insidious onset; worse by activity & weight-bearing; relieved by rest; crepitus; decreased ROM; PE - weight-bearing joint involved; DIP - heberden nodes; PIP - bouchard nodes; MTP joint of 1st toe; cervical spine
|
|
|
Q269. Osteoarthritis - Dx
|
A269. Based on clinical & XR; XR - irregular joint space narrowing, osteophytes, subchondral sclerosis, subchondral bone cysts; ESR normal; synovial fluid aspiration - straw-colored fluid, normal viscosity, WBC < 3000
|
|
|
Q270. Osteoarthritis - Tx
|
A270. Weight reduction; physical therapy; NSAIDs; intra-articular corticosteroid injections; elective joint replacement - total hip/knee arthroplasty
|
|
|
Q271. Duchenne Muscular Dystrophy - What is it; What is Becker's
|
A271. XLR; defect of dystrophin - cytoskeletal protein; MC muscular dystrophy; most lethal; ages 2-6; Becker – milder, XLR, abnormal-sized dystrophin
|
|
|
Q272. Duchenne Muscular Dystrophy - History/PE
|
A272. History - axial and proximal before distal muscles; progressive clumsiness; fatigability; hard to stand or walk; hard to walk on toes; waddling gait; Gower's maneuver; PE - pseudohypertrophy of gastrocnemius; possible MR
|
|
|
Q273. Duchenne Muscular Dystrophy - Dx
|
A273. CK - always high; EMG; muscle Biopsy; DNA; diagnostic - immunostain for dystrophin
|
|
|
Q274. Duchenne Muscular Dystrophy - Tx
|
A274. No cure; Tx supportive; physical therapy; achilles tendon release; wheelchair by 13 y/o; death in 20s
|
|
|
Q275. what is the defect in Bruton's agammaglobulinemia?
|
A275. X-linked recessive defect in a tyrosine kinase gene associated with low levels of all classes of Igs
|
|
|
Q276. this disorder occurs in boys and is associated with recurrent bacterial infections after 6 months of age, when levels of maternal IgG antibody decline
|
A276. Brutons agammaglobulinemia (B cells)
|
|
|
Q277. this immune deficiency presents with tetany owing to hypocalcemia and recurrent viral and fungal infections
|
A277. DiGeorge syndrome/thymic aplasia (T cells)
|
|
|
Q278. this immune deficiency is associated with congenital defects of heart and great vessels
|
A278. DiGeorge syndrome
|
|
|
Q279. what ist eh chromosomal abnormality associated with DiGeorge syndrome?
|
A279. 22q11 deletion
|
|
|
Q280. this is a defect in early stem cell differentiation and presents with recurrent viral, bacterial, fungal, and protozoal infections
|
A280. SCID - B and T cell deficiency
|
|
|
Q281. failure to synthesize MHC II antigens, defective IL-2 receptors, and adenosine deaminase deficiency can all lead to what immune deficiency?
|
A281. SCID
|
|
|
Q282. what does IL-12 receptor deficiency (decreased activation of T cells) present with?
|
A282. disseminated mycobacterial infections
|
|
|
Q283. defect in CD40 ligand on CD4 T helper cells leads to inability to class switch; presents early in life with severe pyogenic infections
|
A283. hyper-IgM syndrome (decreased activation of B cells)
|
|
|
Q284. this disorder is characterized by high levels of IgM and very low levels of IgG, IgA, and IgE
|
A284. hyper-IgM syndrome
|
|
|
Q285. this syndrome is characterized by an X-linked defect in the ability to mount an IgM response to capsular polysaccharides of bacteria
|
A285. Wiskott-Aldrich syndrome (decreased activation of B cells)
|
|
|
Q286. what is the triad of symptoms associated with Wiskott- Aldrich syndrome?
|
A286. infections, thrombocytopenic purpura, eczema (WIPE)
|
|
|
Q287. this syndrome is associated with elevated IgA levels, normal IgE levels, and low IgM levels
|
A287. Wiskott-Aldrich syndrome
|
|
|
Q288. this syndrome presents with recurrent 'cold' (noninflamed) staphylococcal abscesses, eczema, coarse facies, retained primary teeth, and high IgE levels
|
A288. Job's syndrome (decreased activation of macrophages)
|
|
|
Q289. this syndrome is characterized by failure of gamma- interferon production by helper T cells; neutrophils fail to respond to chemotactic stimuli
|
A289. JOb's syndrome
|
|
|
Q290. what is the defect in leukocyte adhesion deficiency syndrome?
|
A290. defect in LFA-1 adhesion proteins on phagocytes
|
|
|
Q291. this syndrome presents early with severe pyogenic and fungal infections and delayed separation of umbilicus
|
A291. leukocyte adhesion deficiency syndrome
|
|
|
Q292. how is Chediak-Higashi inherited?
|
A292. autosomal recessive
|
|
|
Q293. this disease is marked by a defect in microtubular function and lysosomal emptying of phagocytic cells
|
A293. Chediak-Higashi disease
|
|
|
Q294. this disease presents with recurrent pyogenic infections by staph and strep, partial albinism, and peripheral neuropathy
|
A294. Chediak-Higashi disease
|
|
|
Q295. defect in phagocytosis of neutrophils owing to lack of NADPH oxidase activity or similar enzymes
|
A295. chronic granulomatous disease
|
|
|
Q296. how is the diagnosis of chronic granulomatous disease confirmed?
|
A296. negative nitroblue tetrazolium dye reduction test
|
|
|
Q297. this disease presents with marked susceptibility to opportunistic infections with bacteria, especially S. aureus, E. coli, and Aspergillus
|
A297. chronic granulomatous disease
|
|
|
Q298. what is the defect in chronic mucocutaneous candidiasis present?
|
A298. idiopathic dysfunction of T cells specifically against candida albicans
|
|
|
Q299. what is the most comon selective immunoglobulin deficiency? how does it present?
|
A299. selective IgA deficiency - presents with sinus and lung infections;; milk allergies and diarrhea are common
|
|
|
Q300. ataxia-telangiectasia is an idiopathic dysfunction of what type of cells?
|
A300. B cells
|
|
|
Q301. defect in DNA repair enzymes with associated IgA deficiency; presents with cerebellar problems and spider angiomas
|
A301. ataxia-telangiectasia
|
|
|
Q302. deficiency of what leads to hereditary angioedema?
|
A302. C1 esterase inhibitor
|
|
|
Q303. deficiency of which complement protein leads to severe, recurrent, pyogenic sinus and RT infections?
|
A303. C3
|
|
|
Q304. deficiency of what complement proteins leads to Neisseria bacteremia?
|
A304. C6-C8
|
|
|
Q305. deficiency of what leads to paroxysmal nocturnal hemoglobinuria?
|
A305. decay-accelerating factor
|
|
|
Q306. patients with what deficiency have an increased susceptibility to recurrent bacterial infections, especially with encapsulated bacteria
|
A306. C3 deficiency;; not detected until later in life
|
|
|
Q307. what is the most important immunological protective mechanism against blood-borne encapsulated organisms?
|
A307. IgG-mediated opsonization in the spleen
|
|
|
Q308. Warthin-Finkeldy giant cell is pathognomonic for what?
|
A308. measles or the live attenuated measles vaccine
|
|
|
Q309. Lyme arthritis is associated with what HLA?
|
A309. HLA-DR4
|
|
|
Q310. patients with Wiskott-Aldrich syndrome have a 12% chance of developing what?
|
A310. non-Hodgkin's lymphoma
|
|
|
Q311. test of choice to determine presence of circulating anti-Rh antibody?
|
A311. indirect Coombs test to measure IgG anti-Rh antibody
|
|
|
Q312. low levels of all antibody classes
|
A312. common variable immunodeficiency
|
|
|
Q313. spleen is important for removing what type of organisms? list 3
|
A313. strep pneumo,; H. flu,; Neisseria
|
|
|
Q314. what is defective in leukocyte adhesion deficiency?
|
A314. integrins - function both in adhesion of leukocytes to other cells and in the phagocytosis of complement-coated material
|
|
|
Q315. HLA types associated with SLE?
|
A315. HLA-DR2 and HLA-DR3
|
|
|
Q316. most likely sequelae of rheumatic fever?
|
A316. mitral valve disease
|
|
|
Q317. antitopoisomerase antibodies?
|
A317. scleroderma/systemic fibrosis - likely to develop diffuse systemic fibrosis & death from consequences of systemic disease such as pulmonary fibrosis or malignant hypertension
|
|
|
Q318. what is responsible for strong binding between monocytes, T lymphocytes, macrophages, neutrophils, and dendritic cells, and injured epithelium?
|
A318. LFA-1; interacts with ICAM-1
|
|
|
Q319. an increased level of what cytokine would decrease the likelihood of a delayed-type hypersensitivity reaction?
|
A319. IL-10
|
|
|
Q320. what 2 molecules exert the most powerful chemotactic effect on neutrophils?
|
A320. C5a and C8
|
|
|
Q321. what are the best markers for identification of B cells?
|
A321. CD19, CD20, CD21
|
|
|
Q322. IgG subclass deficiency is associated with a deficiency with what other substrate?
|
A322. IgA
|
|
|
Q323. what is C-reactive protein a marker of?
|
A323. non-specific inflammation - one of the most commonly measured acute-phase reactants
|
|
|
"stuck-on" appearance
|
seborrheic keratosis
|
|
|
red plaques with silvery-white scales and sharp margins
|
psoriasis
|
|
|
the most common type of skin cancer; the lesion is a pearly-coated papule with a translucent surface and teleangiectasias
|
basal cell carcinoma
|
|
|
honey-crusted lesions
|
impetigo
|
|
|
febrile patient with a history of diabetes presents with a red, swollen, painful lower extremity
|
cellulitis
|
|
|
positive Nikolskys sign
|
pemphigus vulgaris
|
|
|
negative Nikolskys sign
|
bullous pephigoid
|
|
|
a 55 year old obese patient presents with dirty, velvety patches on the back of the neck
|
acanthosis nigricans --> check fasting blood sugar to rule out diabetes
|
|
|
dermatomal distribution
|
varicella zoster
|
|
|
flat-topped papules
|
lichen planus
|
|
|
iris-like target lesions
|
erythema multiforme
|
|
|
a lesion characteristically occurring in a linear pattern in areas where skin comes into contact with clothing or jewelry
|
contact dermatitis
|
|
|
presents with a herald patch, Christmas-tree like pattern
|
pityriasis rosea
|
|
|
a 16 year old presents with an annular patch of alopecia with broken-off, stubby hairs
|
alopecia areata (autoimmune process)
|
|
|
pinkish, scaling, flat lesions on the chest and back; KOH prep has a "spaghetti-and-meatballs" appearance
|
pityriasis versicolor
|
|
|
four characteristics of a nevus suggestive of melanoma
|
asymmetry, border irregularity, color variation, large diameter
|
|
|
premalignant lesion fro sun exposure that can lead to squamous cell carcinoma
|
actinic keratosis
|
|
|
"dew-drop on a rose petal"
|
lesions of 1st degree varicella
|
|
|
"cradle cap"
|
seborrheic dermatitis; treat with antifungals
|
|
|
associated with propionbacterium acnes and changes in androgen levels
|
acne vulgaris
|
|
|
a painful, recurrent, vesicular eruption of mucocutaneous surfaces
|
herpes simplex
|
|
|
inflammatoin and epithelial thinning of anogenital area, predominantly in postmenopausal women
|
lichen sclerosis
|
|
|
exophytic nodules on the skin with varying degrees of scaling ulceration; the second most common type of skin cancer
|
squamous cell carcinoma
|
|
|
what vitamin do you supplement for a measles infection?
|
vitamin A
|
|
|
normal skin at birth that gradually progresses to dry, scaley skin = ??
|
ichthyosis vulgaris, aka lizard skin
|
|
|
dry, rough skin over extensor surfaces + horny plates = ??
|
ichthyosis
|
|
|
what vitamin supplement should be give for measles?
|
vitamin A
|
|
|
normal birth at skin that gradually progresses to dry, scaley skin = ??
|
ichythyosis vulgaris, aka lizard skin
|
|
|
dry, rough skin over extensor surfaces + horny plates = ??
|
ichthyosis
|
|
|
virus that causes measles
|
paramyxovirus
|
|
|
name of red spots with bluish specks over buccal mucosa and what disease it is associated with?
|
Koblik spots, measles
|
|
|
cough + coryza + conjunctivitis = ??
|
measles
|
|
|
well-circumscribed areas of depigmentation over arms/legs
|
vitiligo
|
|
|
autoimmune disease that attacks melanocytes and is associated with other AI diseases?
|
vitiligo
|
|
|
most common metal causing contact dermatitis
|
nickel
|
|
|
how do you rule out melanoma?
|
excisional biopsy
|
|
|
if a melanoma is >1mm deep what else must you do besides excise it?
|
sentinal lymph node study
|
|
|
poison ivy is what type of hypersensitivity exposure and what causes it? does it require prior exposure?
|
type IV hypersensitivity, cell-mediated which means you need prior exposure
|
|
|
what causes molluscum contagiosum?
|
pox virus
|
|
|
best method for photo-protection (avoiding sun burn)
|
sun avoidance
|
|
|
numerous umbilicated vesicles over healing atopic dermatitis = ??
|
eczema herpeticm
|
|
|
name the SIRS criteria
|
1. fever/hypothermia2. tachypnea3. tachycardia4. leukocytosis, leukopenia or bandemia
|
|
|
what is the normal course for impetigo?
|
erythmatous macule --> vesicle --> pustule --> honey-colored, crusted exudates
|
|
|
what causes hereditary angioedema?
|
C-1 inhibitor deficiency
|
|
|
what virus causes rubella?
|
RNA togovirus
|
|
|
what is the chronology for rubella?
|
1. exposure2. fever, malaise3. suboccipital adenitis4. maculopapular rash on face then trunk and extremities
|
|
|
treatment for tinea corporis
|
terbinafine
|
|
|
most common viral infection of hand
|
herpetic whitlow; common in healthcare workers
|
|
|
most common cause of acquired angioedema
|
ACEI use
|
|
|
what dermatological disorder is commonly seen with Parkinsons?
|
seborrheic dermatitis
|
|
|
which types of hypersensitivity are anti-body mediated?
|
types I, II, III
|
|
|
name the different types of hypersensitivity?
|
type I - anaphylactic, atopictype II - cytotoxictype III - immune complex, serum sickness, arthus reactiontype IV - delayed, cell-mediated
|
|
|
polygonal + purples + pruritic + papules = ??
|
lichen planus
|
|
|
what type of hypersensitivity is psoraisis?
|
T-cell mediated
|
|
|
yellow, greasy, erythematous scaling patches/plaques = ??
|
seborrheic dermatitis
|
|
|
young person with severe seborrheic dermatitis --> what must you rule out?
|
HIV
|
|
|
what BSA defines Stevens-Johnsons and what is the treatment?
|
<10% BSA, treat with analgesia and IVIG
|
|
|
what skin disorder is commonly associated with other autoimmune disorders?
|
vitiligo
|
|
|
what is the most common cause of cellulitis and what is the treatment of choice?
|
staph, treat with keflex
|
|
|
what causes hot tub folliculitis?
|
pseudomonas aeruginosa
|
|
|
what is a kerion?
|
inflammatory granulomatous reaction in children to tinea capitus
|
|
|
bullseye rash
|
Lyme disease
|
|
|
treatment for lice
|
permethrin shampoo
|
|
|
dome-shaped with central umbilication
|
molluscum contagiosum
|
|
|
christmas-tree pattern with herald patch
|
pityriasis rosea (HHV-6)
|
|
|
what causes cervical CA?
|
usually HPV 16, 18, 31, 33
|
|
|
Shagreen patches with ashleaf spots
|
tuberous sclerosis
|
|
|
cafe-au-lait spots
|
neurofibromatosis
|
|
|
hemangioma/port-wine stain on face
|
Sturge-Weber syndrome
|
|
|
what are hemangiomas often indicative of?
|
von Hippel-Lindau disease
|
|
|
what is the sign of Leser-Trelat?
|
multiple seborrheic keratoses erupting at once associated with underlying malignancy, often gastric cancer
|
|
|
most common skin CA associated with sun exposure
|
basal cell CA
|
|
|
ABCD of melanoma
|
Asymmetric shapeBorders irregularColor variationDiameter >6mm
|
|
|
what are strawberry hemangiomas and what do they indicate?
|
they are benign vascular tumors of children that usually regress on their own at 5-8 years old
|
|
|
what rash on the body does not appear scaly but will scale with scraping?
|
tinea versicolor
|
|
|
rosey-hue with teleangiectasias over cheeks, nose, chin
|
rosacea
|
|
|
treatment for moderate to severe acne, predominantly nodulocystic and firm
|
oral isotretinoin
|
|
|
what nail problems is psoriasis associated with?
|
onycholysis and nail pitting
|
|
|
what is erysipelis? what bacteria commonly causes it?
|
commonly seen in patients with impaired lymph drainage who develop a rash that looks like "orange peels"; caused by strep pyogenes
|
|
|
what are strong risks for a mole that is maligant?
|
changes in size/shape/color/borders
|
|
|
what anesthestic is used for suturing vessel-rich areas?
|
1% lido with 1:100,000-1:400:000 epi
|
|
|
what rash do you need to look for with warfarin?
|
look for warfarin-induced necrosis that can occur within 1 week of beginning warfarin therapy; well-demarcated erythematous lesion that progresses to necrosis
|
|
|
what is bullous pemphigoid? what do you see on immunoflorescence?
|
it is an autoimmune bullous disorder in patients over 60 that present with wide-spread blistering over flexor and perianal surfaces; immunoflorescence will show epidermal basement membrane antibodies
|
|
|
what is the most important factor in determining the resectable margins with a melanoma?
|
depth of the tumor
|
|
|
what is the most effective means to prevent death from melanoma?
|
early clinical detection
|
|
|
what is the most preventable risk factor for developing melanoma?
|
chronic sun exposure
|
|
|
what condition presents as a macular scaling behind the ears, on the scalp, eyebrow, nasal-labial folds? who commonly gets it?
|
serborrheic dermatitis; common with patients that have neurological disorders or HIV
|
|
|
what presents with erythematous plaques with silvery-white scales on the extensor surfaces?
|
psoriasis
|
|
|
what solution should be given during the first 24 hours following a burn injury?
|
lactated ringers
|
|
|
what is pemphis vulgaris? what do you see on immunoflorescence?
|
it is an autoimmune disease of the skin that presents with painful, fragile blisters of the oropharynx, chest, face and perianal regions; look for antibodies to adhesion desmoglein molecules
|
|
|
this disease results from a deficiency of hepatic uroporphyinogen decarboxylase and presents with chronic blistering of sun exposed regions and skin hyperpigmentation? who is it associated with?
|
porphyria cutanea tarda; seen with alcoholics and hepatitis
|
|
|
this disease presents with vesicular lesions and crusting erythematous plaques over the genital region, chest, neck and axilla with an malodorous discharge
|
familial benign pemphigus
|
|
|
what is Groves disease?
|
it is a transient acantholytic dermatosis in men >50; appears as small red papules on back/chest
|
|
|
Where does atopic dermatitis present in infants?
|
Face, scalp, extensor surfaces. Diaper area is spared
|
|
|
What is the treatment for atopic dermatitis?
|
Topical steroids- but not longer than 2-3 weeks
|
|
|
How does seborrheic dermatitis present in an infant?
|
Red diaper rash with yellow scale, erosions, and blisters. A thick crust may be seen on the scalp.
|
|
|
What kind of people can develop severe seborrheic dermatitis?
|
HIV and Parkinson's patients
|
|
|
How do you treat seborrheic dermatitis?
|
Selenium sulfide or zinc pyrithione shampoos for the scalp; Topical antifungals or steroids for other areas in adults
|
|
|
When does a drug eruption occur?
|
7-14 days after exposure
|
|
|
What is erythema multiforme?
|
Targetoid lesions that can be on the palms and soles and associated with systemic symptoms. Can lead to TEN or SJS
|
|
|
What is erythema nodosum?
|
Panniculitis that can be triggered by infection (STREP, histo, cocci, yersinia, TB), drug reactions (sulfonamides, OCPs, abx), and chronic inflammatory disease (IBD, sarcoidosis, Behcet's)
|
|
|
How does erythema nodosum present?
|
Painful, erythematous nodules on the lower legs. Patients may have a false positive VDRL
|
|
|
What is bullous pemphigoid?
|
Antibodies to the BMZ that presents as firm, tense, stable blisters with NO Nikolsky sign or mucosal involvement. Linear immunofluorescence pattern. Treated by steroids
|
|
|
What is pemphigus vulgaris?
|
Antibodies to desmoglein (keratinocyte adhesion), lace-like/fishnet immunofluorescence, flaccid bullae, POSITIVE Nikolsky sign, common mucosal involvement (starts in mouth), treated by high-dose steroids + IVIG
|
|
|
What are triggers for pemphigus vulgaris?
|
ACEIs, penacillamine, phenobarbital, penicillin
|
|
|
What is erysipelas?
|
Starts out as a small red patch on the cheek or extremities that turns into a painful shiny red plaque. patients often have a history of cutaneous ulcers, pharyngitis, or lymphedema
|
|
|
What does scarlet fever look like?
|
Sunburn with goosebumps
|
|
|
What does the rash of Salmonella typhi look like?
|
Small pink papules on the trunk (rose spots) in groups of 10-20 plus fever and GI involvement. Treat with Rocephin and possible cholecystectomy for chronic carrier state
|
|
|
What is Ludwig's angina?
|
Bilateral cellulitis of the submental, submaxillary, and sublingual spaces from an infected tooth
|
|
|
How does necrotizing fasciitis present?
|
Sudden onset of pain and swelling at the site of trauma or recent surgery. Erythema spreads quickly over the course of hours to days and the skin becomes dusky and purplish. There is undermining of the skin and subcutaneous layer, bullae, gas production
|
|
|
How is necrotizing fasciitis treated?
|
Early and aggressive surgical debridement followed by Pen G + Flagyl or Rocephin
|
|
|
What monthly blood tests do patients on isotretinoin require?
|
LFTs, TGs, cholesterol, and B-hCGs
|
|
|
What is tinea versicolor?
|
Small, scaly patches of varying color on the chest or back that are hypopigmented. Treat with ketoconazole or selenium sulfide
|
|
|
How does gas gangrene present?
|
Around a site of recent injury or surgery. Swelling around the injury with skin that turns pale and then dark red
|
|
|
How can gas gangrene be treated?
|
Hyperbaric oxygen, surgical debridement, abx
|
|
|
What does lichen planus look like?
|
Violaceous, flat-topped, polygonal papules with prominent Koebner's phenomena (lesions at the site of trauma) with a shiny surface with fine white lines (Wickham's striae). Tx with steroids
|
|
|
How do you treat rosacea?
|
Flagyl
|
|
|
What needs to be ruled out when pityriasis rosea is suspected?
|
Fungal infection (KOH stain)Syphilis (RPR)
|
|
|
How is melanoma treated?
|
Lesions confined to the skin are treated by excision with margins
|
|
|
What is tinea capitis?
|
Infection of the scalp; mainly affects children with scaly patches of hair loss and possible inflamed, boggy granuloma of the scalp. REQURES SYSTEMIC Antifungals
|
|
|
What infection can cause erythema multiforme?
|
Herpes
|
|
|
What is heratoacanthoma?
|
Rapidly growing (grows to full size in 1-2 months) flesh-colored lesion with a central crater that contains keratinous material, usually on the face. Spontaneously involutes but observe in those with a history of it
|
|
|
What's the derm term for:Flat spot <1cm (non-palpable, just visible)
|
Maculeexamples: Freckles, tattoos
|
|
|
What are some of the distinguishing characteristics of necrotizing fasciitis?
|
Unexplained, excruciating pain in the absence of or beyond areas of cellulitisErythema with blister and bullae formation & possible crepitusDM patient with foot cellulitis and signs of systemic toxicityPerineal cellulitis with abrupt onset & rapid spread (Fournier’s gangrene)
|
|
|
What is the treatment for a limb with dry gangrene?
|
Autoamputation over time Angiography to evaluate the extent & location of peripheral artery disease → distal bypass of stenotic areas → if circulation improves & healing is adequate, then amputation of the affected region
|
|
|
What is the treatment for wet gangrene infection?
|
Emergency debridement or guillotine amputation of the infected portion of the foot then revision to a below or above the knee amputation 72 hours later (antibiotics are indicated if cellulitis or gas gangrene is present) |