Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
60 Cards in this Set
- Front
- Back
|
What are the acute metabolic complications of diabetes mellitus?
|
DIabetic ketoacidosis
Hyperglycemic, hyperosmolar state |
|
|
What is the definition of diabetic ketoacidosis?
|
A life-threatening state that results from a relative or absolute deficiency of insulin
|
|
|
What kinds of diabetics are more likely to develop ketoacidosis?
|
Type 1
|
|
|
What are the problems that result from too little insulin? Too much insulin?
|
Too little: DKA
Too much: hypoglycemic |
|
|
What, other than too little insulin, can push a type 1 diabetic into DKA?
|
Illness
Stress |
|
|
What hormones are found in high levels in DKA?
|
Stress hormones:
-Epi -Norepi -GH -Cortisol |
|
|
What are the precipitating factors for DKA?
|
Insufficient or no insulin
Physical stress Surgery, infections, heart attacks, etc. |
|
|
How does DKA develop in people who are insulin deficient?
|
Decreased activity of LPL inside cell (less incorporation of fat) and increased activity of HSL
As a result, more FFAs are present in the circulation, Also, stress hormones cause the release of FFAs. |
|
|
Where in the body are ketone bodies made?
|
LIVER.
|
|
|
What are the ketones present in diabetic ketoacidosis?
|
Acetoacetate
Beta-hydroxybutyrate |
|
|
What is the action of ketone bodies in diabetic ketoacidosis?
|
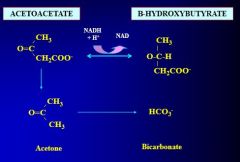
Weak acids; donate protons
|
|
|
What are the symptoms of hyperglycemia?
|
Polyuria, polydipsia
Severe volume depletion Electrolyte depletion Endpoint: renal hypoperfusion, prerenal azotemia, hypotension, shock |
|
|
What are the symptoms of ketones in the blood?
|
Acidosis
Compensatory respiratory alkalosis Hypotension Shock |
|
|
What's the clinical course of diabetic ketoacidosis?
|
1. Precipitating event
2. Polyuria, polydipsia, dehydration 3. Anorexia, nausea, vomiting, abdominal pain 4. Kussmal respirations, "juicy fruit" breath 5. Altered complications 6. CV collapse 7. Coma, death |
|
|
What's the cause of impairment of CNS function in DKA?
|
Hypertonicity
Hypotension Acidosis |
|
|
What is the diagnositc triad of DKA?
|
Increased blood glucose
"Gap" metabolic acidosis Increased serum ketones |
|
|
What's the formula for anion gap?
|

|
|
|
What's the cause of an increase in anion gap?
|
Increases in organic acids (ketone bodies, essentially) causes a decrease in HCO3, increasing the gap
|
|
|
If someone has a fever and is diabetic, what should you think?
|
DON'T ALWAYS ASSUME DKA!!!!
Think infection until proven otherwise |
|
|
What's the treatment for DKA?
|
1. IV insulin
2. IV fluids: RAPID 3. Replace electrolytes (Na, K, Mg, PO4) 4. Carbohydrate replacement once serum glucose is below 250 mg/dL 5. Diagnose and treat the PRECIPITATING EVENT! |
|
|
What should you not administer during DKA?
|
Bicarb.
|
|
|
What's the purpose of administering insulin in DKA?
|
1. Shut down lipolysis
2. Lower blood sugar. |
|
|
What shouldn't you do while treating DKA?
|
Shut off the insulin too early.
This is the MOST COMMON MISTAKE THAT PEOPLE MAKE WHILE TREATING PEOPLE WITH DKA!!!!!!!! |
|
|
What happens to potassium stores in DKA?
|
They're overall decreased, despite elevation in the serum.
During acidosis, you get a shift of H into cells, with K coming out. Increased serum load of K means peeing out K |
|
|
What's the effect of giving insulin on serum K?
|
Driving K back into cells
THIS IS BAD. |
|
|
What should you do as soon as you see someone peeing with DKA?
|
Give them K!
If the kidneys don't work, don't give them K. You'll kill them due to hyperkalemia! |
|
|
What should you follow when treating DKA? Why?
|
Anion gap, not ketone levels.
Acetone is produced during the regeneration of bicarb. Ketone levels are going to actually INCREASE during therapy. |
|
|
What happens in a hyperglycemic hyperosmolar state?
|
Life-threatening metabolic disorder of extreme hyperglycemia without ketosis
|
|
|
Who typically gets into a hyperglycemic hyperosmolar state?
|
Elderly with type 2 diabetes
30% haven't been diagnosed! |
|
|
What are common precipitating events causing a hyperglycemic hyperosmolar state?
|
MI
Stroke Sepsis |
|
|
What's the prognosis from a hyperglycemic hyperosmolar state?
|
>40% mortality
|
|
|
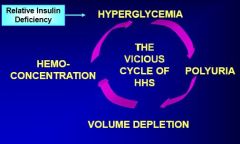
What is the cycle that happens in a hyperglycemic hyperosmolar state?
|
|
|
|
What are complications following volume depletion and hemoconcentration in a hyperglycemic hyperosmolar state?
|
Hyperviscosity --> increased thrombosis risk
Disturbed mentation and obtundation Neurologic signs |
|
|
What are some neurologic signs secondary to volume depletion in a hyperglycemic hyperosmolar state?
|
Focal signs: sensory/motor deficits or focal seizures
Motor abnormalities |
|
|
What are the levels of hyperglycemia in hyperglycemic hyperosmolar state?
|
1700-1800!
Super dooper high! |
|
|
Why is it that people go into a hyperglycemic hyperosmolar state instead of DKA?
|
They still have enough residual insulin to prevent lipolysis
However, they don't have enough insulin to control blood sugars |
|
|
What's the treatment for a hyperglycemic hyperosmolar state?
|
Volume correction with normal saline
Replacement of electrolytes IV insulin Diagnosis and tx of underlying cause |
|
|
What are the chronic complications of diabetes?
|
Retina
Kidneys Nerves Heart, brain, large vessels |
|
|
What organs are impacted by microvascular complications of diabetes?
|
Retina
Kidneys Nerves |
|
|
What organs are impacted by macrovascular complications of diabetes?
|
Heart
Brain Large vessels |
|
|
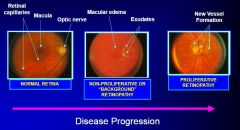
What is the progression of diabetic retinopathy?
|
|
|
|
What are hard exudates in the retina?
|
Areas of protein leakage with iscemia
|
|
|
What are the stages of diabetic retinopathy?
|
1. Non-proliferative
2. Proliferative |
|
|
What happens when there is chronic disease in the retina?
|
New vessel formation due to the edema.
These vessels can scar. Ultimately you get retinal detachment, which leads to blindness |
|
|
What's the leading cause of new adult blindness in the United States?
|
Diabetic retinopathy
|
|
|
What changes occur to the kidneys in diabetic nephropathy?
|
Basement membrane thickening and mesangial cell proliferation
Dropout of adipocytes |
|
|
How can you go about looking for early stages of diabetic nephropathy?
|
Albumin screening
Microalbuminuria is a sign of early nephropathic change |
|
|
What's the leading cause of renal failure leading to dialysis in the US?
|
DIBITUS!!!
|
|
|
Where are the first places that diabetic neuropathy shows up?
|
The extremities: stocking-glove distribution
|
|
|
What are the changes that happen with diabetic neuropathy?
|
Decreased vibration, temperature, proprioception
|
|
|
What are the early signs of diabetic neuropathy?
|
Parasthesias: burning, pins, etc.
|
|
|
What are complications that can occur to feet in diabetic neuropathy?
|
Foot ulcers
Charcot feet: people walk abnormally, causing bone remodeling that disfigures the feet. |
|
|
What are some other (other than distal, that is) neuropathies that happen in diabetes?
|
Gastroparesis-->constipation/diarrhea
Erectile dysfunction Urinary retention Chronic edema Postural hypotension Cardiac arrhythmias Abnormal sweating Increased callus formation |
|
|
What's the leading cause of non-traumatic lower extremity amputation in the US?
|
Diabetes
|
|
|
What are some macrovascular complications of diabetes?
|
Gangrene
Coronary heart disease Stroke |
|
|
What are the properties of MIs that happen in diabetes?
|
THEY OFTEN DON'T HAVE CHEST PAIN!!!
ALWAYS JUST GET AN EKG!!!!!!!!!! |
|
|
What are complications for the mother during pregnancy in diabetes?
|
Insulin requirements increase
Retinopathy, nephropathy worsen |
|
|
What are the complications for the baby in the pregnancy of a person with diabetes?
|
Infant mortality is increased
More congenital malformations Respiratory distress syndrome is more common Big babies - they're GIANT! |
|
|
What is the impact of hyperglycemia on wound healing?
|
Decreased:
-WBC motility -WBC opsinization of bacteria -Fibroblast collagen issues |
|
|
What are infectious complications of diabetes?
|
Complications from influenza are more common in diabetic individuals
Tb and pneumococcal pneumonia are common Yeast infections in women |