![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
38 Cards in this Set
- Front
- Back
Front (Term) |
Plateau is lower than peak Volume : of 500ml delivered, about 300mk not exhaled - large leak: cuff rupture |
|
|
Ischemic stroke sbp <220 Hemorrhage sbp < 140 |
Acute upper GI bleed Common - peptic ulcer Urea/creatinine ratio >100 - upper |
|
|
Variceal bleed : band ligation preferred over sclerotherapy |
Risk of recurrent bleed ulcer Active arterial bleed - 90% Non bleeding visible vessel - 50% |
|
|
Acute liver failure - cerebral edema is the common cause of death. Cautious with Peep as it can worse brain edema |
Seizures- Phenytoin better ICP: paco2 25-30, mannitol, barbiturates Hepatic encephalopathy- lactulose is controversial. No change in outcomes |
|
|
TIPS - dec mortality in severe variceal bleeds |
Tips CI: severe TR, PH >45, chf, poly cystic liver disease, sepsis, unrelieved biliary obstruction |
|
|
Quantity massive hemoptysis |
Definitions vary- 1. >100 ml/hr 2. >150 ml single time |
|
|
Life threatening hemoptysis |
1. hemodynamic instability 2. significant gas exchange defect 3. significant airway obstruction |
|
|
When can TXA be used in hemoptysis |
1. non massive hemoptysis- neb TID x 5 days 2. |
|
|
Inferior MI, which vessel and EKG pattern? |
1. RCA 2. Elevation II III aVF, depression V1-3 |
|
|
Left circumflex STEMI EKG? |
Elevation in 1, V5, V6 |
|
|
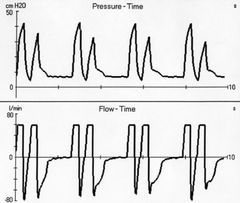
Causes for abrupt loss of tidal volume on p-cmv |
1. obstruction- volume loss and flow loss w/prolonged expiratory time (mucous plugging, tube kinking, foreign body, blood clot in the tube, or bronchospasm) 2. abrupt compliance reduction: inspiratory and expiratory time are shortened (flash edema, pneumothorax, pleural bleeding, or mainstem bronchus intubation)
|
|
|
RAP estimate from IVC measurement - spontaneously breathing pt |
IVC <1.5: 0-5 IVC 1.5-2.5 cm >50% collapse: 5-10 IVC 1.5-2.5 <50% collapse: 11-15 IVC >2.5 <50% collapse: 16-20 |
|
|
How does transducer affect a-line BP reading? |
Should be at the level of the heart. If higher- lower BP read d/t gravity effect. As long as transducer at heart level, arm position doesn't matter. |
|
|
Pressor of choice in takotsubo CM? |
alpha agonist - also don't volume deplete - can cause LV outflow tract obstruction |
|
|
Estrogen in pregnancy |
Upper airway issues - edema, nasal polyps. Difficult intubation LAM - estrogen responsible for inflammation |
|
|
Progesterone in pregnancy |
Central resp stimulation causing ventilation changes |
|
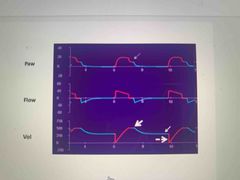
what is this? |
breath stacking or double stacking If on volume control > switching to pressure control will resolve the breath stacking but the delivered volume will be higher than the desired volume (but less the the increased volume that occurs with breath stacking). |
|
Can this patient get a VILI with these setting? (this is a brain bleed pt w/ nl CXR and ABG). |
Yes. This is SELF induced lung injury (SILI) due to excessive patient respiratory drive (likely bc of brain injury). What to do: address underlying causes of excessive patient respiratory drive (resp alk, liver dx, pain). Can consider suppressing resp drive |
|
|
what drugs are known to unmask or worsen myasthenia gravis symptoms |
macrolides, fluoroquinolones, aminoglycosides, magnesium, and β-blockers
|
|
|
what is End-inspiratory transpulmonary pressure |
Pplat − end-inspiratory pleural (esophageal) pressure. Values >30 cm H2O are generally considered excessive.
|
|
what is this? |
circuit leak |
|
|
what is rapidly reversible sedation-associated delirium (RRSAD)? and does it effect mortality like prolonged delirium does in the ICU? |
subtype of delirium with outcomes not different than that of patients never exhibiting delirium. |
|
|
acid/base problem and other symptoms that can hint at salicylates toxicity. |
HAGMA + respiratory alkalosis. If patient has tinnitus that can be a sign of ASA toxicity. Expected CO2 (winters formula) = (1.5 x HCO2) + 8 +- 2 |
|
|
formula for osmolar gap? and what is formula for calculated osmolality? |
osmolar gap = measured - calculated calculated Osm = 2xNa + BUN/2.8 + glucose/18 |
|
|
how to measure respiratory system compliance on ventilator if not given? |
TV/inflating pressure inflating pressure = Pplt - PEEP |
|
|
what drug is the only FDA approved reversal agent for NOAC dabigatran (directly inhibits thrombin)? what about for rivaroxaban, apixaban, and edoxaban (factor Xa inhibitors)? |
Idarucizumab (binds to where dabigatran binds to thrombin - higher affinity then thrombin) Andexanet alfa (looks similar to factor Xa - so it acts like a decoy and has factor Xa inhibitors bind to intself instead of real factor Xa) |
|

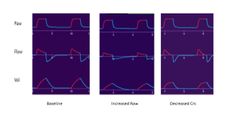
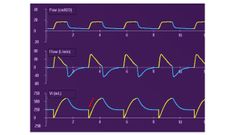
what happened in A, B, and C in a PRESSURE mode |
A: airway obstruction (bronchospasm, mucus plug, ETT kink, foreign body, clot on ETT). Drop in TV but SLOW expiratory flow pattern. B: stiff lung/low compliance (flash pulm edema, PTX, pleural effusion, parenchymal lung injury). Low TV, same set pressure, FAST expiratory flow pattern bc of low compliance. If pulm edema happened in VOLUME mode -> same TV with INCREASE in pressures C: TV is intact but expiratory vol is much less = circuit leak |
|
|
how to distinguish between sepsis fever/serotonin syndrome/neuroleptic malignant syndrome/and malignant hyperthermia |

look at reflexes vs rigidity vs GI disturbances to give clues |
|
|
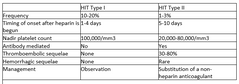
difference between HIT 1 and 2 |
|
|
|
what vent changes do you make in an ARDS pt when they are placed on VV ECMO |
Decrease TV - even to the point of anatomical dead space (3-5ml/kg) Decrease FiO2 Goal of above to decrease Pplt to 5-8 cm H20 Leave PEEP to prevent atelectal trauma |
|
|
Tx for GBS |
PLEX or IVIG |
|
|
Diagnosis and findings with heptatopulmonary syndrome (HPS) |
Triad: 1/ liver dx, 2/ increased A-a gradient on RA, 3/ intrapulm vascular dilatations (IPVD). Sx include: hypoxemia, platypnea, and orthodeoxia IPVDs cause a V/Q mismatch where blood streaming through center of capillary might not have time to get oxygenated. Dx: ECHO with bubble study (appearance of micro-bubbles in LA w/in 3-6 cycles). Tx: no medical therapy. May resolve after liver tx (but also puts pt at higher risk for problems/mortality during liver tx) |
|
|
results of the study using intensivist vs palliative care to talk to family. |
No difference in anxiety/depression score between two groups. Increased PTSD in palliative care group No difference in mortality/HLOS |
|
|
what happens to the BP reading when the arterial line transducer is not at the level of the heart? |
if above level of heart > lower BP (and vica versa) |
|
|
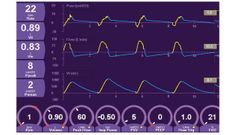
what is and what are causes of: High peak and plt presures? High peak and lower plt pressures? |
High peak/plt = change in compliance/parenchymal issue (PTX, pleural effusion, RMS intubation [severe atelectasis], flash pulm edema, increase in extrathoracic pressures). Expiratory flow would be faster and shorter. High peak/normal plt = airway resistance (mucus plug, bronchospasm, Kinked ETT). you ALSO will see reduced expiratory flow with prolonged expiration (you will ONLY see this if it is a pressure mode) |
|
|
which oral anticoagulation has been shows to be effective for VTE and malignancy |
edoxaban (Lixiana). |
|
|
what are some of the things that happen in ARDS when you do lung protective strategies |
1) decrease lung injury 2) decrease proinflammatory cytokines 3) decrease alveolar edema by active transport of Na/Cl across alveolar epithelium |
|
|
what is the leading cause of death for patients with neurofibromatosis |
The intrathoracic lesions are plexiform neuroblastomas, which can undergo malignant transformation. Any patient with neurofibromatosis type 1 (NF1) who develops new onset symptoms not otherwise explained, with a change in size of a neurofibroma, should be evaluated for malignancy. Malignant transformation of benign neurofibromas to malignant peripheral nerve sheath tumors (MPNSTs) is the leading cause of mortality. FIRST prove it is malignant (w/ bx) THEN you can do surgical excision |