Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
47 Cards in this Set
- Front
- Back
|
Toxoplasma gondii
|
|
|
Pneumocystis jiroveci
PCP |
|
|
What was the initial "AIDS test"?
|
CD4 count
|
|
|
Describe AIDS opportunistic infections
|
If you are in an area that is co-edemic for TB that is usually what comes first. The indicator is things like thrush. People who enter the hospital usually enter for PCP or for toxoplasma gondii. As people would progress they would develop disseminated mycobacterium.
|
|
|
Describe Pneumocystis jirovecii (PCP)
|
-Commensal organism and opportunistic pathogen
-Morphologically resembles protozoan -Difficult to grow in vitro |
|
|
Describe the life cycle of Pneumocystis jirovecii (PCP)
|
-Cyst stage: 5um in diameter with 4-8 sporozoites
-Trophozoite: 2-5um in diameter- attach to cell surfaces |
|
|
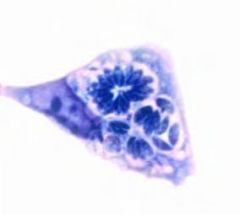
Cyst stage of PCP with individual sporozoites
|
|

|
A chest X-ray of a woman with PCP
|
|
|
Describe what occurs with PCP infections
|
-Organisms plug alveoli with proteinacious types of exudate
-PCP can be seen in sputum in severe cases -In less severe cases bronchoscopy and/or biopsy is used -PCP can also present as a lower lobe infection for patients who stop taking antiretrovirals |
|
|
How do you treat PCP infections?
|
Two Antifolates
Sulfonamide/Dapsone inhibits Dihydropteroate Synthetase Pyrimethamine/Proguanil inhibit Dihydrofolate reductase. |
|
|
How does PCP seem like a protozoon? How does it seem like a fungus? Why the similarity?
|
Protozoon
-Morphology -Inability to culture in vitro -Response to anti-protozoal drugs Fungus -Ribosomal rRNA sequence homology -ELF3 Early protozoa are similar to protozoon fungi |
|
|
Describe opportunistic infections in transplant patients
|
-Same type as in AIDS
-Occurs in 2-3 months of beginning immuno suppression -Use prophylaxis to prevent opportunistic infections |
|

|
Sporulated and unsporulated oocysts of Toxoplasma gondii
|
|
|
What is the definitive host of toxoplasma gondii?
|
The cat
|
|
|
What can toxoplasma gondii infect?
|
All mammalian nucleated cells
They particularly like muscles and the brain |
|
|
What are the stages of toxoplasma gondii?
|
Tachyzoite - Intracellular stage, similar to trophozoite stage of malaria. Acute, active infection
Bradyzoite- Cyst stage (latent infection) Sporozoite - In the intestine of the cat. Has a diploid stage that sporulates and develops into a haploid stage. |
|
|
Describe the life cycle of Toxoplasma gondii
|
-Cat passes oocyst in stool
-Can be picked up orally by any mammal through exposure to cat feces or eating dormant cysts in meat -Bradyzoites become active and turn into tachyzoites -Sporozoites from oocyst do the same and undergo asexual cycle -Then there is immediate illness of hepatitis, lymphadenopathy, and rarely active cerebritis -OR after a brief period of fever it differentiates into a pseudocyst -Asymptomatic but in half of peoples brains -Not a problem unless you are immunosuppressed - |
|
|
Describe the unsporulated stage of Toxoplasma gondii
|
Diploid, sexual stage coming from cat
|
|
|
Describe the sporulated stage of Toxoplasma gondii
|
produces sporozoites that become the infectious phase
|
|
|
What meat tends to have large amounts of toxoplasma pseudocysts?
|
Lamb
|
|
|
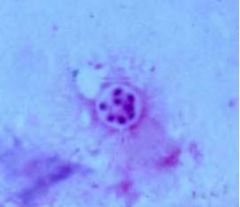
Pseudocyst of Toxoplasma gondii
|
|
|
What cell does Toxoplasma gondii infect in people?
|
Macrophage
Toxoplasma has adhesions and has serine and cysteine proteases to come to the cell and starts wrapping itself up with the macrophage membranes. It then encircles itself in a parasitopherous vacuole. This is a macrophage that is supposed to be picking up cells and presenting antigens to start the host response. The parasite is taking advantage of this particular hunter cell, encasing itself in host membranes, and doing very well. |
|
|
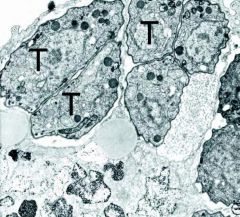
Toxoplasma gondii in culture
These are tachyzoites. They are encasing themselves and preventing what would normally happen which is fusion with lysosomes, thus escaping digestion. |
|
|
What are the types of clinical disease associated with Toxoplasma gondii?
|
-Congenital
-Adult-acquired -AIDS-related |
|

|
Skull x-ray of a child with congenital toxoplasmosis
There are calcifications throughout and an overly large skull |
|
|
What does congenital toxoplasmosis cause?
|
A spectrum of illness that is dependent on when in the pregnancy the mother experienced the acute infection. The earlier in the pregnancy the infection the worse the outcome
-Still birth -Hydrocephale -Macrocephale with the rest of the body being small -Chorioretinitis (intermediate) -Subtle cognitive defects (3rd trimester) |
|
|
Describe the calcifications in the brain in congenital toxoplasmosis
|
There are necrotic areas that become calcified and nonactive.
There is active toxoplasma infection, necrotic areas, a pus filled area which then resolve. There is bleeding into the area and with the bleeding you get calcification. |
|
|
What causes congenital toxoplasmosis?
|
An acute infection in the mother followed by transplacental spread
It is easier to infect the mother as pregnancy progresses |
|
|
Describe toxoplasma ocular disease
|
Usually from congenital infection manifesting in adults
-Episodic flares may destroy retinal tissue -Specific treatment necessary -Occurs when a mother is infected in the third trimester |
|
|
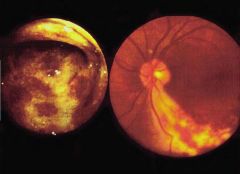
Toxoplasma ocular disease
Hemorrhagic areas with a lot of exudate around it This leads to scarring of the retinas |
|
|
Describe adult-acquired toxoplasmosis
|
-Infection by blood or organ transplant
-Parasitemia (WBC's) for up to 1 year post infection (esp in immunocompromised individuals) -Heart, bone marrow, liver, kidney donors -Dangerous when recipient toxo (-) -Myocarditis, diffuse lymphadenopathy -TORCH infections are screened in all transplant situations |
|
|
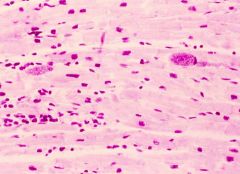
Adult-acquired toxoplasmosis (heart)
|
|
|
What are the signs and symptoms of adult-acquired toxoplasmosis?
|
Lymphadenopathy
Fever Headache Chronic malaise This is what would occur in a more severe case in a normal host. You can develop diffuse lymphadenopathy. In normal host this can be a debilitating and severe illness. |
|
|
What distinguishes the differentials of toxoplasmosis, inf. mono, and lymphoma?
|
Inf mono uniquely has pharyngitis, atypical lymphocytes, positive heterophil, and strong altered liver function
Toxoplasmosis uniquely has normal liver function Lymphoma uniquely has strong anemia and hilar lymphadenopathy Biopsies are only useful for lymphoma |
|
|
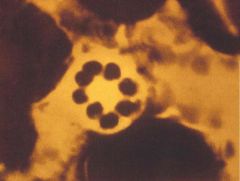
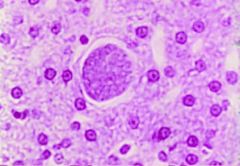
Pseudocyst of Toxoplasma gondii in liver
|
|
|
Describe self Toxoplasma gondii reactivation in a transplant situations
|
You can reactivation from your own pseudocysts but it tends to be a milder illness than if you are a negative recipient of a positive organ.
|
|
|
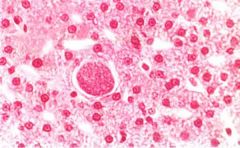
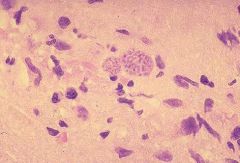
Pseudocysts of Toxoplasma gondii in a microglial nodule with a variety of inflammatory cell types in an HIV/AIDS patient
|
|
|
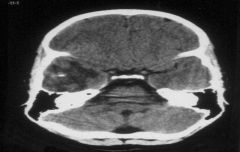
Ring enhancing lesion of a CAT scan
Usually this is toxoplasmosis, but TB and lymphoma can both do this. |
|
|
Describe AIDS related Toxoplasma gondii infection
|
1. CD4<200 and reactivation of latent infection
2. Encephalitis a. Diffuse inflammation and swelling b. Localized ring enhancing lesions of CT scan c. Herniation d. Death if untreated |
|
|
Why do you get ring enhancing lesions in Toxoplasmosis gondii?
|
You have toxoplamosis infection with lots of inflammation and swelling which is controlled with some bleeding in the area will lead to calcification. The enhancement is just showing the presence of active inflammation.
|
|
|
Describe the serological correlates in acute and chronic Toxoplasmosis gondii infection
|
Early on in about a week there is a rise in IgM. Then that peaks and goes away in 8-10 weeks. In about 2 weeks you have a rise of IgG which then goes down. This will be positive for life. In the case of pregnancy you are looking for a positive IgG when you would then not have to worry about the rest of the pregnancy. If it is negative you have to be more careful. Even more risky is the litter box for cats where you have those sporocysts that are contaminating other things or if you get it on your hands and accidentally ingest the form from the cat. .
|
|
|
How can diagnosis of Toxoplasma gondii infection be made?
|
-Serology
-Lymph node biopsy + immunofluorescence |
|
|
Describe treatment of Toxoplasma gondii infection
|
If there is little swelling in brain
-Antifoltes -Wait 7-10 days for clinical response -Lesion shrinks in toxoplasmosis, but not in lymphoma or TB In case of severe intracranial pressure -Steroids + Antifolate -Steroids reduce inflammation, but obscure the diagnosis -Both toxo and lymphoma shrink -Stereotactic needle biopsy for diagnosis |
|
|
What drugs are used for Toxoplasma gondii infections
|
Antifolates
|
|
|
How do you prevent toxoplasma gondii infection?
|
1. Prevent pregnant women from handling cat litter
2. Avoid eating raw or undercooked meats |
|
|
Compare the host status in PCP and toxoplasma condi
|
PCP:
-No life cycle -Lung disease in AIDS -Malnourished children -Organ transplants Toxoplasma gondii -Cat definitive host -Disease: Host status -CNS disease in AIDS -Congenital infections -Organ transplants |
|
|
What parasites are on their way out?
|
Onchoerciasis and Trachoma
|