Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
91 Cards in this Set
- Front
- Back
|
Vasculitis is defined as ________________.
|
Inflammation of the blood vessel wall (arterial or veins)
|
|
|
The wall of a blood vessel is composed of what layers?
|
Tunica intima (endothelial cells sitting on basement membrane)
Tunica media (smooth muscle) Tunica adventitia (connective tissue layer) |
|
|
Most cases of vasculitidies are NOT ____________.
|
infectious
|
|
|
Etiology of vasculitis is usually __________.
|
unknown
|
|
|
Clinically we can get two types of symptoms when patients present with a vasculitis. Explain.
|
(1) Nonspecific symptoms
- Inflammation --> fever, weight loss, fatigue, myalgia etc. (seen in most vasculitides) (2) Symptoms of organ ischemia - Damage of wall --> Thrombus. After damage, healing results in fibrosis, narrowing wall with ischemia. |
|
|
Vasculitides are divided into what categories?
|
Large-, medium- small-vessel vasculitis
|
|
|
Large vessel vasculitis involves ___________.
|
the aorta or its branches
|
|
|
This is the MC form of vasculitis in older individuals. It usually affects ___________ (males/females)
|
Temporal (giant cell) arteritis.
Usually affects females |
|
|
Temporal (Giant cell) arteritis is classically seen in older adults age ________.
|
> 50 yo.
|
|
|
What arteries are classically involved in temporal arteritis?
|
Branches of carotid artery
|
|
|
Describe clinical symptoms in context of vessel involved in temporal arteritis. Also mention other symptoms.
|
(1) Headache (temporal)
(2) Visual disturbances (ophthalmic) (3) Arteries that feed the jaw or mm. of jaw giving us jaw claudication. Other: flu-like symptoms with joint and muscle pain. |
|
|
What is the disease called when a patient with temporal arteritis has joint and muscle pain with flu symptoms?
|
Polymyalgia Rheumatica. Seen in a subset of patients with temporal arteritis.
|
|
|
What lab parameter is elevated in temporal arteritis?
|
ESR (greater than 100)
|
|
|
What is seen on biopsy of an artery affected by temporal arteritis?
|
Inflamed vessel wall with giant cells (granulomatous vasculitis) and intimal fibrosis.
|
|
|
The lesions in temporal arteritis are ______________ (continuous/segmental).
|
segmental
|
|
|
What is something important to remember when performing biopsy of an artery in a patient with temporal arteritis?
|
Take a very long piece of the vessel, because lesions are segmental. Check each segment.
|
|
|
Temporal arteritis: You receive a negative biopsy. Does this exclude disease?
|
No. You've taken a piece of the vessel where disease is not present.
|
|

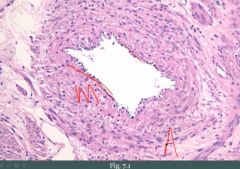
What is this?
|
Temporal arteritis. Look at all the fibrosis (F) separating intima (I) from the media (M). Lumen is narrowed. Also note inflammation and giant cells.
|
|
|
Treatment of temporal arteritis?
|
Corticosteroids.
|
|
|
Why should you give treatment as soon as you suspect (even if you don't have confirmation on biopsy) temporal arteritis.
|
There is a high risk of blindness without treatment.
|
|
|
Temporal (giant cell) arteritis is a _____________ (large/medium vessel) vasculitis.
|
Large vessel
|
|
|
Takayasu arteritis is a _____________ (large/medium vessel) vasculitis.
|
large
|
|
|
Takayasu arteritis is the same disease as temporal arteritis (it's a spectrum), however, there are some exceptions
|
(1) In temporal arteritis we see it in patients greater than 50, in takayasu we see it in patients less than 50 yo.
(2) Takayasu is more proximal than temporal. Involves the aortic arch at branch points. |
|
|
What type of inflammation do we have in takayasu?
|
Same as temporal; granulomatous inflammation.
|
|
|
How is takayasu and temporal arteritis similar?
|
(1) Granulomatous inflammation
(2) Large vessel vasculitis (3) ESR elevated (4) Treatment is corticosteroids |
|
|
Regarding Takayasu arteritis, involvement of the ____________ at _______ points results in ________ and _________ symptoms.
|
aortic arch; branch; visual; neurologic
|
|
|
What arteries are involved in Takayasu arteritis?
|
Aortic arch at branch points.
|
|
|
What does involvement of the aortic arch at branch points in Takayasu arteritis lead to?
|
(1) Visual and neurologic symptoms
(2) Weak or absent pulse in an upper extremity ('pulseless disease') |
|
|
Medium-vessel vasculitides involve what?
|
Muscular arteries that supply organs.
|
|
|
What defines a medium-sized vessel?
|
Muscular arteries (e.g. renal artery)
|
|
|
What "type" of vasculitis occurs in polyarteritis nodosa?
|
Necrotizing vasculitis
|
|
|
What organ(s) are involved in polyarteritis nodosa?
|
Most organs (polyarteritis = many arteries)
|
|
|
What organ is spared in polyarteritis nodosa?
|
Lungs
|
|
|
Polyarteritis nodosa is a ______________ (large/medium/small sized vessel) vasculitis.
|
medium
|
|
|
Polyarteritis nodosa typically presents in ___________.
|
young adults
|
|
|
Polyarteritis nodosa affecting the renal artery would present as _________.
|
HTN
|
|
|
Polyarteritis nodosa affecting the mesenteric artery would present as _________.
|
Abdominal pain with melena
|
|
|
What are classic findings in Polyarteritis nodosa?
|
(1) HTN
(2) Abdominal pain with melena (3) Neurologic disturbances (4) Skin lesions |
|
|
PN is associated with what serum molecule?
|
HBsAg
|
|
|
An early lesion in PN is?
|
Transmural inflammation with fibrinoid necrosis of a vessel
|
|
|
Why is the disease called polyarteritis NODOSA?
|
When lesions heal after inflammation, massive fibrosis in that particular segment makes the artery seem hard (like a node).
|
|
|
True or false: In PN all the lesions are of the same stage.
|
False, lesions of varying stage are present.
|
|
|
What is a consequence of lesions of varying stage in PN in clinical diagnosis?
|
'String-of-pearl' appearance on imaging.
In areas where inflammation is present, we may weaken the wall and get an aneurysm. Aneurysm-fibrosis-aneurysm-fibrosis may form this appearance. |
|
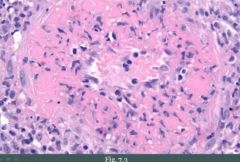
What is seen?
|
Example of fibrinoid necrosis.
|
|
|
Treatment of PN?
|
(1) Corticosteroids
(2) Cyclophosphamide |
|
|
Kawasakis disease is a _____________ (medium/small vessel) vasculitis.
|
medium
|
|
|
Kawasaki's disease classically affects ___________ children _____ years old.
|
asian; < 4 yo
|
|
|
How do children with Kawasaki's disease present?
|
Non-specific vague symptoms.
(1) Fever (2) Conjunctivitis (3) Erythematous rash on palms and soles (4) Enlarged cervical lymph nodes |
|
|
The preferential artery that is involved in Kawasaki's is the _________.
|
coronary artery (it is common)
|
|
|
What is a dreaded complication(s) of Kawasaki's?
|
(1) Thrombosis with MI.
(2) Aneurysm with rupture. |
|
|
Treatment of Kawasaki's disease?
|
(1) Aspirin (prevent thrombosis)
(2) IV IG |
|
|
Kawasaki's disease is ______________ (pervasive/self-limited).
|
self-limited
|
|
|
Memory help: How could you think about Kawasaki's disease?
|
Picture a 4-yo on a Kawasaki motorcycle. They would be using their palms and soles to drive (rash). Heart rate goes up when you drive a motorcycle (MI).
|
|
|
Buerger's disease is a ______________ (small/medium/large vessel) vasculitis.
|
medium
|
|
|
What is Buerger's disease (short)?
|
Necrotizing vasculitis involving the digits.
|
|
|
How does Buerger's disease present?
|
Presents with ulceration, gangrene, and autoamputation of fingers and toes.
|
|
|
This vasculitis is highly associated with smoking.
|
Buerger's disease.
|
|
|
Treatment of Buerger's disease?
|
Smoking cessation
|
|
|
A girl experiences pale digits some time after she first started smoking. What is it called? What is it associated with?
|
Raynaud's syndrome.
Associated with Burger's. |
|
|
What is the color changes seen in Raynaud's phenomenon?
|
White (compromised blood flow) to blue (cyanosis) to red (reperfusion)
|
|
|
Small vessel vasculitis involves ________, ________ and _________.
|
arterioles; capillaries; venules
|
|
|
Wegener's granulomatosis is a _______________ (small/medium/large vessel) vasculitis.
|
small
|
|
|
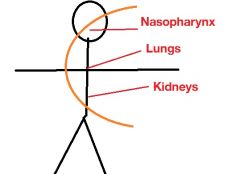
What is Wegener's granulomatosis?
|
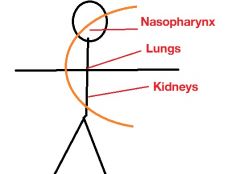
Necrotizing granulomatous vasculitis involving the nasopharynx, lungs, kidneys.
|
|
|
Mnemonic version of the name of Wegener's granulomatosis?
|
weCener's granulomatosis
("The C disease") (1) C-ANCA (2) C-distribution (3) Cyclophosphamide |
|
|
Wegener's granulomatosis classically presents in what subgroup of patients?
|
Middle-aged males
|
|
|
Wegener's granulomatosis classically presents as?
|
(1) Sinusitis or nasopharyngeal ulceration
(2) Hemoptysis with bilateral nodular lung infiltrates (3) Hematuria due to RPGN |
|
|
The hematuria that may be present in Wegener's granulomatosis is due to what pattern of disease in the kidney?
|
RPGN
|
|
|
What molecule could tell you something about Wegener's granulomatosis?
|
C-ANCA. Levels correlate with disease activity.
|
|
|
On biopsy in a patient with Wegener's granulomatosis you would see what?
|

Large necrotizing granulomas with adjacent necrotizing vasculitis.
|
|
|
Key treatment in Wegener's granulomatosis?
|
Cyclophosphamide and corticosteroids
|
|
|
After treatment, Wegener's usually ____________ (remain in remission/relapse).
|
Relapse (relapses are common)
|
|
|
Microscopic polyangiitis is a ____________ (small/medium/large vessel) vasculitis.
|
small (microscopic)
|
|
|
What is microscopic polyangiitis?
|
Necrotizing vasculitis involving multiple organs, especially lung and kidney.
|
|
|
What is the difference in the pattern of involvement of organs in microscopic polyangiitis and wegener's?
|
Wegener's: Nasopharynx, lung, kidney
Microscopic: Especially lung and kidney |
|
|
Microscopic polyangiitis is similar to Wegener's, however, two things are absent in this disease. What is it?
|
(1) Nasopharyngeal involvement is absent
(2) Granulomas are absent (3) P-ANCA instead of C-ANCA (Wegener's) |
|
|
What molecule could tell you something about microscopic polyangiitis?
|
Serum P-ANCA levels correlate with disease severity.
|
|
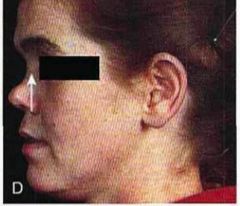
She has a vasculitis. What could it be?
|
Saddle nose deformity in Wegener's (Another C!)
|
|
|
Treatment of Microscopic polyangiitis?
|
Similar to Wegener's. Cyclophosphamide and corticosteroids.
|
|
|
What is a common occurrence after treatment of Microscopic polyangiitis.
|
Same as for Wegener's, recurrence is common.
|
|
|
Churg-Strauss syndrome is a ____________ (small/medium/large vessel) vasculitis.
|
small
|
|
|
What is Churg-Strauss syndrome?
|
Necrotizing granulomatous vasculitis with eosinophils.
|
|
|
Churg-strauss syndrome involves what organs?
|
Multiple organs, especially lungs and heart.
|
|
|
A patient has a vasculitis. You observe a P-ANCA in her blood. What vasculitides could this be? How to differentiate?
|
Churg-strauss or Microscopig polyangiitis.
Differentiation: - CS has granulomas, MP not. - CS usually has asthma and peripheral eosinophilia |
|
|
What is HSP?
|
Henoch-Schönlein purpura.
Vasculitis due to IgA IC deposition. |
|
|
HSP is the MC vasculitis in what age group?
|
Children
|
|
|
Classical presentation of HSP?
|

(1) Palpable purpura on buttocks and legs
(2) GI pain and bleeds (3) Hematuria (IgA nephropathy) |
|
|
In HSP, Ig__ deposits in the ___________ of the kidneys.
|
IgA; mesangium
|
|
|
HSP usually follows what?
|
URT infection
|
|
|
HSP is ___________ (pervasive/self-limiting).
|
self-limiting
|
|
|
A boy has HSP that abates. Can it recur?
|
It may recur
|
|
|
HSP is treated with?
|
Steroids if severe, but it is self-limited.
|