![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
147 Cards in this Set
- Front
- Back
|
The longest and strongest bone in the body |
Femur |
|
|
The proximal femur consists of what four essential parts? |
The head, neck, greater trochanter, lesser trochanter |
|
|
The part of the femur that is rounded and smooth for articulation with the hip bones |
Head |
|
|
The depression near the center of the head of the femur |
Fovea capitis |
|
|
The major ligament that is attached to the head of the femur |
Ligament capitis femoris |
|
|
A strong pyramidal process of bone that connects the head with the body in the region of the trochanters |
Neck of femur |
|
|
Large prominence that is located superiorly and laterally to the femoral shaft and is palpable as a bony landmark |
Greater trochanter |
|
|
Small, blunt, conical eminence that projects medially and posteriorly from the junction of the neck and shaft of the femur |
Lesser trochanter |
|
|
A thick ridge that connects the trochanters posteriorly |
Intertrochanteric crest |
|
|
The angle of the femoral neck to the shaft on an average adult |
125 degrees, with a variance of 15 degrees depending on the width of the pelvis and length of the lower limbs |
|
|
The longitudinal plane of the femur is about how many degrees from vertical? |
10 degrees |
|
|
In relation to the body of the femur, what is the anterior angle of the head and neck? |
15 to 20 degrees |
|
|
What does the word pelvis mean? |
Basin |
|
|
What are the four bones of the pelvis? |
Two hip bones, one sacrum, one coccyx |
|
|
What is another name for the hip bones? |
Innominate bones |
|
|
What articulates to form the lumbosacral joint? |
The sacrum articulates superiorly with the 5th lumbar vertebrae |
|
|
What articulates to form the sacroiliac joints? |
The right and left iliac bones articulate posteriorly with the sacrum |
|
|
What are the three divisions of the hip bones? |
Ilium, ischium, pubis |
|
|
A deep, cup-shaped cavity that accepts the head of the femur to form the hip joint |
Acetabulum |
|
|
The ilium is composed of what two parts? |
A body and an ala (wing) |
|
|
The superior margin of the ala |
Iliac crest |
|
|
A less prominent projection below the ASIS |
Anterior inferior iliac spine |
|
|
The part of the hip bone that lies inferior and posterior to the acetabulum |
Ischium |
|
|
The two parts of the ischium |
A body and a ramus |
|
|
Projects anteriorly from the ischial tuberosity |
Ramus of the ischium |
|
|
The rounded roughened area near the junction of the lower body and the inferior rami |
Ischial tuberosity |
|
|
A bony projection posterior to the acetabulum. A small part of this is visible on a frontal view of the pelvis |
Ischial spine |
|
|
A deep notch directly superior to the ischial spine |
Greater sciatic notch |
|
|
A small notch inferior to the ischial spine |
Lesser sciatic notch |
|
|
Bears most of the weight of the body when an individual sits |
Ischial tuberosities |
|
|
The relation of the body of the pubis to the acetabulum |
Anterior and inferior |
|
|
Extending anteriorly and medially from the body of each pubis |
Superior ramus |
|
|
Formed when the two superior rami meet in the midline to form an amphiarthrodial Joint |
Symphysis pubis |
|
|
Passes down and posterior from the symphysis pubis to join the ramus of the respective ischium |
Inferior ramus |
|
|
A large opening formed by the ramus and body of each ischium and by the pubis |
Obturator foramen |
|
|
The largest foramen in the human skeletal system |
Obturator foramen |
|
|
Defined by the superior portion of the symphysis pubis anteriorly and by the superior prominent part of the sacrum posteriorly |
Pelvic Brim |
|
|
The bony portion of the pelvis |
False pelvis, or greater pelvis |
|
|
The part of the pelvis that is a cavity and is completely surrounded by bony structures |
True pelvis, or lesser pelvis |
|
|
This forms the actual birth canal |
True pelvis |
|
|
The oblique plane defined by the brim of the pelvis |
Inlet, or Superior aperture |
|
|
Define by the two ischial tuberosities and the tip of the coccyx |
Outlet, or inferior aperture |
|
|
The area between the inlet and outlet of the true pelvis |
Cavity of the true pelvis |
|
|
Which gender has the wider pelvis, with the ilia more flared and more shallow from front to back? |
Female pelvis |
|
|
Which gender has the pelvis that is narrower, deeper, and less flared with a heart-shaped pelvic Inlet? |
Male pelvis |
|
|
What is the angle of the pubic arch in a female? |
Between 80 and 85 degrees |
|
|
What is the angle of the pubic arch in a male? |
50 to 60 degrees |
|
|
Which gender has a more protruding pelvic Inlet? |
Male |
|
|
What classification of joints is the SI joint? |
Synovial |
|
|
What is the mobility type of a sacroiliac joint? |
Amphiarthrodial, limited movement |
|
|
What is the classification of joints for the symphysis pubis? |
Cartilaginous joint |
|
|
What is the mobility type for the symphysis pubis joint? |
Amphiarthrodial, limited movement |
|
|
What is the classification of joints for the union of acetabulum? |
Cartilaginous |
|
|
What is the mobility type of the Union of acetabulum? |
Synarthrodial, non movable |
|
|
What is the classification of joints for the hip joint? |
Synovial |
|
|
What is the mobility type for the hip joint? |
Diarthrodial, ball and socket |
|
|
How much movement does the sacroiliac joint have? |
Limited movement |
|
|
How much movement does the symphysis pubis have? |
Limited movement |
|
|
How much movement does the union of the acetabulum have? |
No movement |
|
|
What is the traditional method used to locate the femoral head and neck? |
Draw an invisible line between the ASIS and the symphysis pubis, determine the midpoint between these two landmarks. The neck is approximately 2.5 inches and the head is 1.5 inches distal and at right angles to the midpoint of this line |
|
|
The greater trochanter are shown to be located on the same horizontal line as what landmark? |
Symphysis pubis |
|
|
What is a better way to find the femoral neck on an obese patient when you cannot locate the greater trochanters? |
Find the ASIS, and the level of the symphysis pubis should be between 3 and 4 in inferior to this. Therefore, the femoral neck can readily be located as being 1-2 inches medial and 3-4 in distal to the ASIS |
|
|
What is the degree that the head and neck of the femur project anteriorly with respect to the femur and the lower leg? |
15° - 20° |
|
|
What happens when the entire lower limb is rotated internally? |
The proximal femur and hip joint our position and a true AP projection. The neck of the femur is now parallel to the IR and will not appear foreshortened |
|
|
On a radiographic image, what is key in determining the correct leg and foot position? |
The lesser trochanter will not be visible at all, or is only slightly visible if the entire leg is rotated internally of full 15 to 20 degrees. If the leg is straight AP or when it is externally rotated, the lesser trochanter is visible |
|
|
A common fracture site for an older patient who has fallen |
Femoral neck |
|
|
What is the typical physical sign for a fracture of the femoral neck? |
External rotation of the involved foot |
|
|
What is the SID for femur and pelvic girdle projections? |
40 in |
|
|
What is the IR size for projections of the femur? |
14 x 17 in |
|
|
What is the kvp range for projections of the femur? |
75 to 85 |
|
|
How many degrees should the leg be rotated internally for an AP projection of the mid-distal femur? |
5 degrees internally |
|
|
What is the lower IR margin on an AP projection of the mid - distal femur? |
Approximately 2 in below knee joint |
|
|
What is the CR method for an AP projection of the mid to distal femur? |
CR perpendicular to femur and IR |
|
|
For a lateral projection of the mid - distal femur, do we usually use mediolateral or lateromedial? |
Mediolateral |
|
|
When is the lateromedial projection of the mid to distal femur done? |
For a trauma patient who cannot rotate their femur |
|
|
How is the medial lateral projection of the mid and distal femur positioned? |
Flex knee approximately 45 degrees with patient on affected side and align femur to mid-line of table or IR. Place on affected leg behind affected leg. Adjust IR to include knee joint. A second IR to include the proximal femur and hip generally will be required on an adult |
|
|
How is a trauma lateromedial projection of the mid and distal femur positioned? |
Play support under affected leg and knee and support foot and ankle in true AP position. Place IR on edge against medial aspect of thigh to include knee, with horizontal x-ray beam directed from lateral side |
|
|
How is a mediolateral projection of the mid and proximal femur positioned? |
Flex affected knee about 45 degrees and align femur to mid-line of table. Extend and support unaffected leg behind affected knee and have patient roll back about 15 degrees to prevent superimposition of proximal femur and hip joint. Adjust IR to include hip joint |
|
|
What is the kvp range for projections of the pelvis? |
80 to 90 kvp |
|
|
What is the IR size for projections of the pelvis? |
14 x 17 |
|
|
How is an AP pelvis projection positioned? |
Ensure that pelvis is not rotated by making sure that the ASIS's on each side are equal. Separate legs and feet, then internally rotate feet and entire lower limb 15 to 20 degrees. |
|
|
What is the CR method for an AP pelvis projection? |
CR is perpendicular to IR. Directed midway between level of ASIS and the symphysis pubis. This is approximately 2 in inferior to level of ASIS |
|
|
What Anatomy is demonstrated an AP pelvis projection? |
Pelvic girdle, L5, sacrum and coccyx, femoral head and neck, and greater trochanters |
|
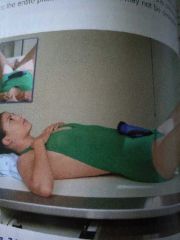
What method is this? |
Modified Cleaves Method |
|
|
What is the modified Cleaves method, or the AP bilateral frog leg projection, used to find? |
Developmental dysplasia of hip, also known as congenital hip dislocation |
|
|
How is the AP bilateral frog leg projection positioned? |
Flex both knees approximately 90 degrees. Place the plantar surfaces of feet together and abduct both femora 40 to 45 degrees from vertical. Ensure that both femora are abducted the same amount and that pelvis is not rotated |
|
|
What Anatomy is demonstrated on the modified Cleaves method? |
Femoral heads and necks, acetabulum, and trochanteric areas are visible |
|
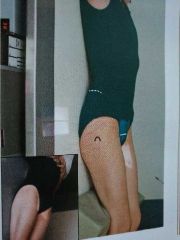
What method is this? |
Taylor Method |
|
|
What is the Taylor method, or AP axial Outlet projection of the pelvis, done to demonstrate? |
Bilateral view of the bilateral pubis and ischium to allow assessment of pelvic trauma for fractures and displacement |
|
|
What is the CR method for the modified Cleaves method? |
CR is perpendicular to IR. Directed to a point 3 in below level of ASIS above symphysis pubis |
|
|
How is the Taylor method positioned? |
Patient lays supine, with legs extended. Place support under knees for comfort. |
|
|
What is the CR method for the Taylor method? |
CR is cephalad 20 to 35 degrees for males, and 30 to 45 degrees for females. CR is directed to a midline point 1 to 2 in distal to the superior border of the symphysis pubis/greater trochanters |
|
|
What is the respiration method for the modified Cleaves method? |
Suspend respiration during exposure |
|
|
What is the respiration method for the Taylor method? |
Suspend respiration during exposure |
|

What method is this? |
Clements-Nakayama Method |
|
|
What is the Clements Nakayama method done to demonstrate? |
Possible hip fracture or with arthroplasty when patient has limited movement in both lower limbs and the inferosuperior projection cannot be obtained |
|
|
What is the IR size for the Clements Nakayama method? |
10 x 12 landscape |
|
|
What is the kvp range for the Clements Nakayama method? |
80 to 90 |
|
|
How is the Clements Nakayama method positioned? |
Legos maintained in neutral position. Rest I are on extended Bucky tray, or use grid. Tilt IR about 15 degrees from vertical and adjust alignment of IR to ensure that face of IR is perpendicular to CR. |
|
|
What is the CR method for the Clements Nakayama method? |
CR is angled mediolaterally as needed so that it is perpendicular to and centered to femoral neck. Angled posteriorly 15 to 20 degrees from horizontal |
|
|
What is the AP axial Inlet projection of the pelvis done to find? |
Assessment of pelvic trauma for posterior displacement or inward / outward rotation of the anterior pelvis |
|
|
How is the AP axial Inlet projection of the pelvis positioned? |
Patient is supine with legs extended, support placed under knees for comfort. |
|
|
What is the CR method for the AP axial Inlet projection? |
CR angled 40° caudad (near perpendicular to plane of Inlet). CR directed to a midline point at level of ASIS |
|
|
What Anatomy is demonstrated in the AP axial Inlet projection? |
The pelvic ring in its entirety |
|

What method is this? |
Judet Method |
|
|
What is the Judet method done to find? |
Acetabular fracture or pelvis injury. Right and left oblique projections are generally taken for comparison |
|
|
What is the IR size for the Judet method? |
10 x 12 portrait, or 14-17 landscape if both hips must be seen on each projection |
|
|
How is the posterior oblique projection of the acetabulum positioned? |
Patient supine, placed in a 45-degree posterior oblique, with both pelvis and thorax 45° from tabletop. Affected side up or down. Align femoral head and acetabulum of interest to midline of tabletop and IR |
|
|
What is the CR method for the right posterior oblique projection of the acetabulum? |
Affected side down. Direct CR perpendicular and centered to 2in distal and 2 inches medial to downside ASIS |
|
|
What is the CR method for a left posterior oblique projection of the acetabulum? |
Affected side up. Direct CR perpendicular and centered to 2 in directly distal to upside ASIS |
|
|
What is the respiration method for the AP axial Inlet projection? |
Suspend respiration during exposure |
|
|
What is the respiration method for the Judet method? |
Suspend respiration for the exposure |
|

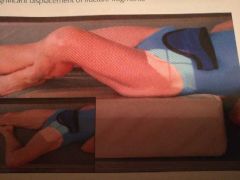
What method is this? |
Teufel Method |
|
|
What is the Teufel method done to find? |
Acetabular fracture, especially the superoposterior wall of the acetabulum |
|
|
How is the PA axial oblique projection of the acetabulum positioned? |
Patient is laying prone at a 35 to 40 degree anterior oblique, with both pelvis and thorax 35 to 40 degrees from tabletop. Align femoral head and acetabulum of interest to midline of tabletop |
|
|
What is the CR method for the Teufel method? |
CR is angled 12° cephalad. CR is directed perpendicular and center to 1 inch superior to the level of the greater trochanter, approximately 2 inch lateral to the midsagittal plane |
|
|
What is demonstrated in the PA axial oblique projection of the acetabulum? |
The superoposterior wall of the acetabulum |
|
|
What is the AP unilateral hip projection taken to find? |
Post-op or follow-up exam to demonstrate the acetabulum, femoral head, neck, and greater trochanter. Also to evaluate condition and placement of any existing orthopedic Appliance |
|
|
How is the AP unilateral hip projection positioned? |
Affected leg is rotated internally 15 to 20 degrees |
|
|
What is the CR method an AP unilateral hip projection? |
CR is perpendicular to the femoral head. Femoral neck can also be localized about 1-2 in medial and 3-4 in distal to ASIS |
|
|
What anatomy should be demonstrated in an AP unilateral hit projection? |
Proximal 1/3 of the femur, acetabulum, and adjacent parts of the pubis, ischium, and ileum |
|
|
What is the IR size for the DM Hip? |
10 x 12 landscape |
|
|
What is the kvp range for the DM hip method? |
85 to 95 kvp |
|
|
What is the Danelius-Miller method done to find? |
Fracture or dislocation assessment in trauma hip situations when affected leg cannot be moved |
|
|
What is another name for the Danelius Miller method? |
Axiolateral inferiosuperior projection of the hip and proximal femur |
|
|
How's the Danelius Miller method positioned? |
Pelvis is elevated 1 to 2 in by placing supports under pelvis. Flex and elevate unaffected leg so that size near vertical position and outside collimation field. Place IR in crease above iliac crest and adjust so that it is parallel to femoral neck and perpendicular to CR. Use cassette holder if available. Internally rotate affected leg 15 to 20 degrees unless contraindicated by possible fracture |
|
|
What is the CR method for the DM hip? |
CR is perpendicular to femoral neck and to IR. |
|
|
What is the respiration method for the DM hip? |
Suspend respiration during exposure |
|
|
What anatomy is demonstrated in a DM hip? |
Entire femoral head and neck, trochanter, and acetabulum |
|

What method is this? |
Danelius-Miller method |
|
What method is this? |
Modified Cleaves Method |
|
|
What is the modified Cleaves method done to find? |
A lateral view to assess hip joint in proximal femur for non-traumatic hip situations |
|
|
What is the IR size for the modified Cleaves method? |
10 by 12 landscape |
|
|
What is the kvp range for the modified Cleaves method? |
75 to 85 |
|
|
How is the unilateral frog leg projection of the hip and proximal femur positioned? |
Flex knee and hip on affected side of the sole of foot against in side of opposite leg, near me if possible. Abduct femur 45 degrees from vertical for general proximal femur region. Center affected femoral neck to CR and midline of IR on table top |
|
|
What is the CR method for the modified Cleaves method? |
CR is perpendicular to IR, directed to mid femoral neck |
|
|
What anatomy is demonstrated on the modified Cleaves method? |
Lateral views of acetabulum and femoral head and neck, trochanteric area, and proximal 1/3 of femur |
|
|
How can you tell when you have a good AP projection of the distal femur? |
Femoral and tibial condyles should appear symmetric in size and shape with the outline of the patella slightly toward medial side of femur. Medial half of fibular head should be superimposed by tibia. |
|
|
How can you tell when you have a good lateral projection of the distal femur? |
Knee joint will not appear open, and distal margins of the femoral condyles will not be superimposed because of Divergent x-ray beam. Anterior and posterior margins of medial and lateral femoral condyles should be superimposed and aligned with open patellofemoral joint space. |
|
|
How can you tell when you have a good lateral projection of the proximal femur? |
Superimposition of the greater and lesser trochanter is by the femur, with only a part of the trochanter is visible on medial side. |
|
|
How can you tell when you have a good AP pelvis projection? |
Lesser trochanter is not visible at all, or only the tips are visible. Greater trochanter is equal in size and shape. Symmetric appearance of the allae, ischial spines, and the two obturator foramina |
|
|
How can you tell when you have a good modified Cleaves method projection? |
The femoral heads and necks , and greater and lesser trochanter should appear symmetric if both thighs were abducted equally. |
|
|
How can you tell when you have a good Taylor method projection? |
Superior and inferior ramus of pubis and body are demonstrated well, with minimal foreshortening or superimposition. Obturator foramina and bilateral ischia are equal in size and shape. Midpoint of symphysis joint should be at Center of collimated field |
|
|
How can you tell when you have a good AP axial Inlet projection of the pelvis? |
Ischial spines fully demonstrated and equal in size and shape. Superimposed anterior and posterior portions of the pelvic ring |
|
|
How can you tell when you have a good AP unilateral hip projection? |
Greater trochanter and femoral head and neck should be in full profile without foreshortening. Lesser trochanter should not project beyond medial border of femur |
|
|
How can you tell when you have a good DM hip projection? |
Entire femoral head and neck, trochanter, and acetabulum should be visualized along with any Orthopedic prosthetic device. |
|
|
How can you tell when you have a good Clements Nakayama projection? |
Femoral head and neck should be seen in profile with only minimal superimposition by greater trochanter. Lesser trochanter is seen projecting posterior to femoral shaft |