Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
72 Cards in this Set
- Front
- Back
|
Hydroceles and _____ inguinal hernias are formed by a similar mechanism.
What is the mechanism? How does it differ? |
Hydroceles and INDIRECT inguinal hernias
Both caused by incomplete obliteration of processus vaginalis. Hydrocele occurs when there's a connection between scrotum and abdominal cavity that only allows leakage of fluid; whereas, a hernia occurs when the opening allows the protrusion of abdominal organs along the inguinal canal. |
|
|
What is effect modification?
Give an example. |
Effect modification occurs when effect of a main exposure of an outcome is modified by another variable.
Ex: Likelihood that asbestos exposure will result in lung cancer is significantly impacted by smoking status. Note that is not a form of bias. |
|
|
What are the molecular effects of smoking marijuana?
Presentation? |
Marijuana is a cannabinoid (not an opiate!) that contains tetrahydrocannabinol (THC).
THC stimulates cannabinoid receptors (CB1 and CB2 receptors) with effects lasting 1-4 hours. Presentation: tachycardia, conjunctival injection (redness of sclera). Note that marijuana is metabolized in the liver and then distributed and stored in lipophilic tissues and slowly released. Remains in the body for up to 30 days after use. |
|
|
34 year-old male
Pruritic skin rash after exposure to outdoor plants Erythematous linear eruption with vesiculations Diagnosis Pathophys |
Poison ivy contact dermatitis; skin lesion is usually linear because plant drags along skin
This is a delayed type hypersensitivy (Type IV) Two phases: -Sensitization: creation of hapten-specific T cells. Cutaneous dendritic cells take up haptens, express them on MHC-I and MHC-II molecules, travel to LN-->interact w/CD4's and CD8's causing activation and clonal expansion Elicitation (re-exposure) phase: Hapten taken up by skin cells (langerhans cells, DC's, keratinocytes) that express MHC-I/II molecules Activate the proliferated hapten-specific T-cells in dermis/epidermis. CD8 T CELLS ARE MAIN EFFECTOR in allergic contact dermatitis |
|
|
56 year-old female
h/o gallstones Cramping abdominal pain, abdominal distention, vomiting X-ray reveals air in biliary tree Diagnosis Pathophys |
Gallstone ileus--large gallstone obstructs ILEOCECAL valve
|
|
|
Normal bleeding time
Prolonged PT Notmal PTT Diagnosis (explain) |
Normal bleeding time means normal platelet function
Normal PTT means normal INTRINSIC pathway (Factors XI, IX, XII) Prolonged PT means abnormal EXTRINSIC PW (Factor VII deficiency) |
|

What is the anticodon of the tRNA that would insert the last amino acid into this polypeptide chain?
|
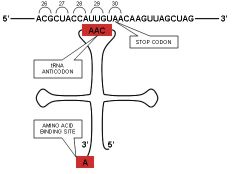
Remember that U goes with A in RNA.
Also remember the stop codons: UAA UAG UGA |
|
|
Which CCBs have the strongest effect on heart rate?
|
Verapamil>Diltiazem>Nifedipine
|
|
|
Which CCBs have the strongest effect on peripheral vasculature?
|
Nifedipine>Diltiazem>Nifedipine
|
|
|
Drug for atrial fibrillation
Causes constipation and second degree AV block |
Verapamil (may also cause bradycardia)
|
|
|
CCB
Causes peripheral edema Reflex tachycardia |
Amlodipine (selective for vascular smooth muscle)-->reflex tachycardia
|
|
|
When is Lidocaine used?
|
Arrhythmias post-MI
|
|
|
12 year0old male
Turbid plasma that forms creamy supernatant on standing Plasma lipoprotein lipase activity is low Diagnosis Pathophys Other symptoms |
Lipoprotein lipase deficiency resulting in increased concentrations of serum chylomicrons (body unable to clear dietary lipid loads due to defective hydrolysis of TGs in chylomicrons)
Pts present in childhood w/hyperlipidemia, pancreatitis (ABDOMINAL PAIN), eruptive skin (NOT TENDON) xanthomas and HSM. Note that tendon xanthomas are assocd w/familial hypercholesterolmia (high LDL); not highTG. |
|
|
Wernicke Encephalopathy:
Pathophys |
Lack of thiamine means lack of TRANSKETOLASE, ALPHA-KETOGLUTARATE DH, and PYRUVATE DH activity
alphta-ketoglutarate-->succinyl-CoA requires Thiamine! Of note, metabolism of EtOH by Alcohol DH and Aldehyde DH consumed NAD+ which further inhibits all pathways requiring NAD+ (Succinyl DH: Succinate-->Fumarate) So alcoholics lack NAD+ and thiamine dependent reactions. |
|
|
Molecular pathway by which E. coli results in septic shock.
|
ENDOTOXINS of outer membrane of Gram negative bacteria, composed of LIPOPOLYSACCHARIDE (LPS).
LPS released during destruction of bacterial cell wall. LPS is heat stable and arranged into three regions: O antigen, core polysaccharide, and LIPID A. LIPID A causes activation of macrophages and granulocytes, releasing IL-1, TNF-alpha, IFN. LIPID A INDUCES SHOCK Note that it is not actively secreted by bacteria (it is released during cell division and by bacteriolysis) |
|
|
56 year-old woman
Just returned from cruise Fever, HA, cough Abdominal pain, watery diarrhea Smokes CXR reveals left lower lobe consolidation Diagnosis Other symptoms |
Legionella-pneumonia (won't appear on gram stain bc it's intracellular)
Will see HYPONATREMIA |
|
|
Which drugs can treat both bipolar disorder and tonic-clonic seizures?
|
Valproate
Carbamazepine Valproate increases inhibitory effect of GABA in CNS. |
|
|
Gastrointestinal ulcers
Renal sontes Psychiatric disorder Diagnosis Effects |
Bones stones, groans, and psychic moans-->PRIMARY HYPERPARATHYROIDISM
Will see SUBPERIOSTEAL THINNING |
|
|
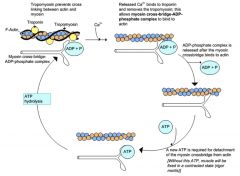
Describe the molecular events of muscle contraction. Begin with calcium.
|
|
|
|
Inotropic vs Metabotropic Receptors:
General Examples (be specific) |
Inotropic: ion channels that open directly upon ligand binding, ex: NICOTINIC cholinergic receptors (resulting in immediate Na and Ca2+ influx, and immediate K+ efflux)
Metabotropic: utilize second messengers to indirectly influence corresponding ion channels Ex: alpha1, M1, M3 (muscarinic)-->IP3 beta1, beta2-->cAMP and Protein Kinase A |
|
|
Where is intussusception most likely to occur?
|
Ileocecal valve (intermittent, severe, colicky abdominal pain, currant jelly stools, sometimes a palpable mass in RLQ)
|
|
|
HBV vs HCV:
Histologic Appearance |
In HBV, hepatocellular cytoplasm fills with granular, eosinophilic substance (HBV surface Ag)--"ground glass"
In HVC, there are lymphoid aggregates within portal tracts (lots of blue spots!) and focal areas of macrovesicular steatosis |
|
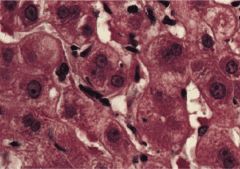
Hepatocytes
Diagnosis |
HBV (ground glass appearance due to accumulation of HB Surface Ag 'granules' in cytoplasm)
|
|
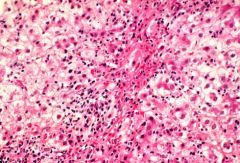
Hepatocytes
Diagnosis |
HCV (not lymphoid cells!)
|
|
|
63 year-old male
Muscle weakness, cramping Takes HCTZ Pathophys |
Decrease in intravascular fluid volume stimulates aldosterone secretion-->increased excretion of K+ and H+ in urine
Thus a hypokalemic metabolic ALKALOSIS Hypokalemia manifests w/muscle weakness and cramping |
|
|
Systolic pressure gradient between LV and aorta:
Diagnosis Effects |
Aortic stenosis-->Dilated CM
|
|
|
How does viral myocarditis result in dilated CM?
|
Patients with acute onset of heart failure in setting of recent viral infection should raise suspicion for dilated CM caused by viral myocarditis.
Caused by an autoimmune reaction to myocytes that have been altered by viral infection. Leads to dilatation of myocardium in all four chambers and resultant decrease in contractility. |
|
|
___gut derivatives rotate around the SMA.
|
Midgut (Duodenum, small intestine, ascending colon, proximal 2/3 transverse colon)
|
|
|
___gut derivates rotate around the IMA.
|
Hindgut (transverse colon, descending, sigmoid colon)
|
|
|
2 day-old neonate
Persistent bilious vomiting Cecum fixed to RUQ Pathophys Associated Risks |
Malrotation of midgut around SMA--entire midgut fixed to superior mesenteric artery
Leads to intestinal obstruction, hence, bilious vomiting , and midgut VOLVULUS with intestinal perforation and gangrene as possible sequelae. Note that intestinal twisting leading to ischemia = Volvulus |
|
|
5 year-old male
Receiving treatment for allergic rhinitis Presents with fever, flushed cheeks, dilated pupils Explain presentation |
Likely receiving H1 receptor (histamin) antagonist such as diphenhydramine for allergic rhinitis (has anticholinergic effects)
Fever is a result of inhibition of eccrine sweat glands Flushing is a result of compensatory cutaneous vasodilation (to cool off) Dilated pupils a result of inhibition of pupillary constrictor and ciliary mm. |
|
|
Bipolar I vs Bipolar II
|
Bipolar I: h/o at least 1 manic episode with or without major depressive episodes (SIGECAPS: Sleep disorder, loss of Interest [anhedonia], Guilt, Energy deficit, Concentration deficit, Appetite disorder, Psychomotor retardation/agitation, Suicidality--needs at least 5 of these for major depression)
Bipolar II: at least 1 major depressive episode and at least one hypomanic episode |
|
|
29 year-old women
4 year h/o fatigue, "not happy" Negative anhedonia, guilt Denies suicidal ideation Diagnosis |
Dysthymic disorder (syx must last more than 2 years!)
|
|
|
7 month-old male
Thrush 2 episodes otitis media 3 episodes bronchiolitis Low serum gamma-globulin CXR reveals absent thymic shadow Diagnosis--explain reasoning |
Severe combined immonudeficiency:
Recurrent otitis media (bacterial) Bronchiolitis (Viral) Candidiasis Suggests primary defect in both cell mediated (T cell) and humoral (B cell) immunity Thymic hypoplasia common among infants w/combined T and B cell deficiencies Hypogammaglobulinemia and recurrent bacterial infections suggest concomitant B cell deficiency Together, this forms the diagnosis of SCID Note: Less than 1% of pts with DiGeorge have complete absence of thymus. Also, lack of characteristic DiGeorge findings (Facial abnlts, hypoparathy, and cardiac defects) makes DiGeorge less likely in this presentation. |
|
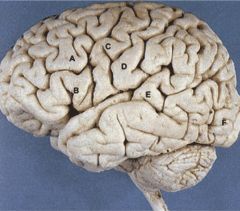
Label and include effect of damage
|
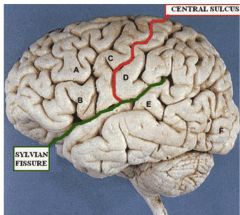
A - Brodmann area 8--frontal eye field. Damage-->eyes deviate to ipsilateral side
B - Broca's area--comprehension intact, but can't formulate motor commands C - Precentral Gyrus (Primary Motor Cortex)--Damage-->dysarthria due to paresis of skeletal mm involved in mvmt of mouth, tongue, larynx D - Postecentral gyrus (Primary Somatosensory Cortex)--sensation loss E - Wernicke's area--word salad, lack comprehension |
|
|
35 year-old alcoholic
Severe abdominal pain, vomiting Laparotomy reveals swollen and partially necrotic pancreas Pathophys |
In acute pancreatitis, inflammation leads to acinar cell damage-->abnormal activation of trypsin inside acinar cells
Trypsin then activates other proteolytic enzymes and starts a self-sustaining (it can also activate trypsinogen) cycle of digestion of pancreatic tissues Autodigestion (autolysis) of pancreas = acute necrotizing pancreatitis |
|
|
40 year-old female
Worsening fatigue Normal vitals, no other medical problems Labs show elevated alkaline phosphatase What blood test should be ordered next and why? |
Bone and liver are primary sources of alkaline phosphatase (although there are other sites)
To clarify the importance of a moderately elevated alk phos, the hepatic gamma-glutamyl transpeptidase (GGTP) should be evaluated GGTP is an enzyme predominantly present in hepatocytes and biliary epithelia GGTP not present to a significant extent in bone. So it's useful in determining whether an elevated alk phos is of hepatic or bony origin. |
|
|
Male Pattern Baldness (androgenetic alopecia):
Mode of Inheritance |
Polygenic (influenced by multiple genes); also presents with variable penetrance
|
|
|
Describe the phases of atrial mycoyte action potential (in pacemaker cells).
Which drugs affect which phase? What are their effects? |
Phase 0 (upstroke): Opening of L-type (long lasting) dihydropuyridine-sensitive Ca2+ channels, slow influx of Ca2+ into cell
Phase 3 (repolarization): Opening of K+ channels, and efflux of K+; closure of L-type Ca2+ channels Phase 4 (pacemaker potential): slow influx of Na+ at end of repolarization; slow K+ efflux as K+ channels continue to close Once membrane ~-50, T-type (Transient) Ca2+ channels open allowing Ca2+ to enter cell and contribute to depolarization Drugs: Phase 4: -NE facilitates opening of L-type Ca2+ channels and Na+ channels-->rapid depolarization -Adenosine and ACh: also act on phase 4; reduce rates of spontaneous depol by activating K+ channels and prolonging K+ flow, also inhibit L-type Ca2+ channels |
|
|
Phentolamine:
Drug Class |
COMPETITIVE alpha adrenergic antagonist
REVERSIBLE! |
|
|
Phenozybenazmine:
Drug Class |
IRREVERSIBLE alpha-adrenergic antagonist (will lower Vmax!)
|
|
|
Clostridium botulinum vs Clostridium tetani:
Specific effects of exotoxins Presentaiton |
C. botulinum: botulinum toxin inhibits acetylcholine release-->FLACCID paralysis
C. tetani: Tetanospasmin causes inhibition of inhibitory interneurons in SC that regulate firing of primary motor neurons. These inhibitory interneurons use GABA and GLYCINE as their NTs, but tetanospasmin prevents release of these NTs. Presents with SPASTIC paralysis, muscle spasms, HYPERreflexia |
|
|
Methadone:
Specific MOA Use AE |
Long-acting mu receptor agonist.
Because it's long acting, its sustained effects allow for continuous suppression of withdrawal syx in heroin dependent patients. Causes AEs similar to other opioids: miosis, respiratory depression seen up to 24 hours after one dose |
|
|
Thiamine:
B vitamin number Reactions that require it Effects of deficiency |
B1
Required for: Pyruvate DH (pyruvate-->Acetyl CoA) a-ketoglutarate DH (enzyme of TCA) Transketolase (enzyme of HMP shunt) Thiamine deficiency results in dec'd glucose utilization, which is pronounced in CNS. AN increase in erthryocyte transketolase levels after thiamine infusion is diagnostic for thiamine deficiency. |
|
|
Enzymes required for conversion of Fructose 6-phosphate to Ribose.
|
F6P-->Glyceraldehyde 3-phosphate via TRANSALDOLASE
Glyceraldehyde-3-phosphate-->Ribose-5-phosphate via TRANSKETOLASE This occurs in the nonoxidative reactions of HMP shunt. All cells can synthesize ribose from Fructose-6-phosphate using nonoxidative reactions. |
|
|
Serpentine, medusa head appearance
|
Bacillus anthracis
|
|
|
Bacillus anthracis:
Mode of infection Appearance on CXR Requirement for pathogenicity |
Pulmonary anthrax (woolsorters disease) is caused by inhalation of spores most commonly while working with goat hair or hides. Hemorrhagid mediastinitis evident as widened mediastinum on CXR.
Requires a capsule that contains D-glutamate instead of polysaccharide--this prevents phagocytosis by host |
|
|
45 year-old male
Periodic epigastric abdominal pain, fatigue Mild hepatomegaly CT shows pancreatic calcifications with no e/o gallstones Hgb 9.0 MCV 115 Diagnosis Pathophys |
Chronic pancreatitis due to ethanol abuse
Alcohol-assocd hepatic steatosis probable cause of hepatomegaly Megaloblastic anemia stems from folic acid deficiency. Folic acid is required for synthesis of purine and pyrimidine bases. Note: If answer reads "diminished thymidine synthesis", this means FAULTY DNA SYNTHESIS!! |
|
|
A-a equation
|
PAO2 = 150 - PaCO2/0.8
A-a = PAO2 - PaO2 |
|
|
3 year-old male
Mental retardation Fair-skinned Blond hair, blue eyes Musty odor Diagnosis Pathophys |
PKU likely due to deficiency of phenylalanine hydroxylase
Pallor of substantia nigra, locus ceruleus, and vagal nucleus dorsalis would also point to this diagnosis. |
|
|
In the US, what is the most prominent form of esophageal cancer?
|
Adenocarcinoma > Squamous Cell Carcinoma
|
|
|
67 year-old male
h/o HTN, TIA treated one month ago Presents with mouth ulcers, fever Diagnosis Pathophys |
Mouth ulcers and fever are characteristic of NEUTROPENIA which was likely caused by TICLOPIDINE
This is why ticlopidine is rarely used and CBC must be performed biweekly for first three months. |
|
|
Acetaminophen toxicity:
Treatment Treatment MOA (specific) |
N-acetyl cysteine; works by two ways:
1) Acts as glutathione substitute and binds to toxic metabolites of acetaminophen 2) Provides SULFHYDRYL groups to enhance non-toxic sulfation elimination of acetaminophen (enhance elimination of non-toxic acetaminophen metabolites) |
|
|
Pulmonary embolism:
Long-term treatment (prevention of recurrence) Specific Treatment MOA |
Warfarin: inhibits vitamin K-dependent CARBOXYLAITON OF GLUTAMIC ACID residues on Factors II, VII, IX, and X (also known as vitamin K dependent clotting factors)
Note that therapy of warfarin doses is monitored via PT time (standardized via international normalized ratio--INR) |
|
|
Cilostazol:
MOA 1 other drug with this MOA |
Agents that increase PLT cAMP will decrease platelet aggregation by preventing PLT shape change and granule release
Cilostazol and Dipyridamole decrease the activity of PLT PDE (enzyme responsible for breakdown of cAMP) Cilostazol additionally acts as a direct ARTERIAL VASODILATOR. |
|
|
Hormone responsible for gallbladder contraction
|
CCK (made in duodenum and jejunum in response to FAs and AAs)
|
|
|
Arginase:
Reaction catalyzed |
Arginine-->Urea + Ornithine (important for getting rid of ammonia!!!)
|
|
|
Black vs Brown Pigment Stones (in GB):
Etiology |
Black Pigment Stone: intravascular hemolysis
Brown Pigment Stones: Biliary Tract Infection |
|
|
Biliary Sludge:
Cause |
Incomplete gallbladder emptying in response to CCK stimulation
Can result in acute cholecystitis Risk factors include: Pregnancy Rapid weight loss Prolonged use of parenteral nutrition or octreotide |
|
|
Dystrophin:
Role |
Note that this is the gene DELETED in Duchenne's
Dystrophin is muscle structural protein that allows for interaction of extracellular connective tissue with the intracellular contraction apparatus. |
|
|
Eggshell calcifications of hilar nodes
|
Silicosis
Also presents w/birefringent particles surrounded by fibrous tissues on histologic exam |
|
|
Calcified pleural plaques with ferruginous bodies
|
Asbestosis
|
|
|
Describe the pathophysiology behind developing a brown pigment stone (GB).
|
Brown pigment stones typically arise secondary to infection of biliary tract, which results in release of beta-GLUCURONIDASE by injured hepatocytes and bacteria (usually E.coli)
beta-glucoronidase contributes to hydrolysis of bilirubin glucuronides and increases the amount of unconjugated bilirubin in bile. This significantly elevates the risk of developing more brown pigment stones. |
|
|
NT changes of HD.
|
Low GABA
Low ACh |
|
|
7 year-old male
Low-grade fever, headache Malaise Slapped cheek appearance Diagnosis Site of viral replication |
Erythema infectiosum (fifth disease) due to Parvovirus B19
The virus is highly tropic for erythrocyte precursors and is found predominantly in the BONE MARROW. |
|
|
35 year-old male
Endocardial thickening due to dense fibrous deposits around tricuspid and pulmonary valves Pulmonary valve stenosis Diagnosis Pathophys Diagnostic lab value |
Fibrous intimal thickening with endocardial plaques limited to right heart = Carcinoid heart disease a/w carcinoid syndrome
Carcinoid syndrome procudes skin flushing, abdominal pain, n/v, diarrhea, due to produciton of SEROTONIN, kallikrein/bradykinin/histamine/PGs by carcinoid tumors Degree of endocardial fibrosis correlates w/PLASMA levels of 5HT and URINARY excretion of serotonin metabolite 5-HYDROXYINDOLEACETIC acid Note that carcinoid syndrome causing R-sided endocardial fibrosis may progress to pulmonic stenosis and/or restrictive cardiomyopathy. |
|
|
26 year-old female
Glutamine for arginine substitution near protein C cleavage site in Factor V gene product Diagnosis Complications |
Factor V Leiden mutation (normally Activated Protein C inactivates factors Va and VIIIa)
In FVL, Factor Va has reduced susceptibility to cleavage by APC and results in hypercoagulable state (predisopses to DVT and PE). |
|
|
21 year-old male
Impaired balance, difficulty speaking Developed slowly over last few months Elevated serum transaminases Negative viral serologies Diagnosis |
Wilson's Disease
Should perform slit lamp examination to check for Kayser-Fleischer rings Note: Wilson's is an autosomal recessive disease due to mutation of gene ATP7B--hinder copper metabolism by reducing formation and secretin of ceruloplasmin and by decreasing secretion of copper into biliary system. |
|
|
Right-sided endocarditis:
Bacterial cause |
Staph AUREUS (not EPIDERMIDIS!!!)
likely an IVDU |
|
|
What drug class can decrease adenomatous polyp formation?
|
COX-2 inhibitors
For unknown reasons, increased COX-2 activity has been associated with increased incidence of adenomas. |
|
|
44 year-old female
Dry skin Night blindness |
Vitamin A deficiency
Could be due to biliary obstruction leading to cholestasis and fat soluble vitamin malabsorption |
|
|
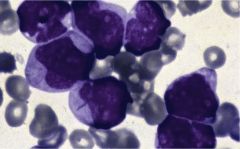
Very large nucleated cells (use red cell size for comparison) with scant cytoplasm-->blast cells-->leukemia likely
Auer rods (even if they're purple!!)--->AML |