Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
122 Cards in this Set
- Front
- Back
|
Lumbar puncture: needle enters subarachnoid space to extract CSF
The needle is usually inserted between __________ because spinal cord may end as low as _____ in adults and _____ in children. |
The needle is usually inserted between L3/4 or L4/L5, because spinal cord may end as low as L2 in adults and L3 in children.
|
|

Young patient comes u with back pain that radiates down his limb, after lifting a heavy load. He prob has hernatied disc.
Herniation of disc usually occurs in lower CERVICAL (C5-C7) OR LUMBAR LEVELS: L4/L5 OR __/____, leading to a DECREASE in the Achilles tendon reflex. A herniation of L4/L5 will compress _______ what level of root? |
Herniation of disc usually occurs in CERVICAL (C5-C7) OR LUMBAR LEVELS: L4/L5 OR L5/S1 leading to a DECREASE in the Achilles tendon reflex.
A herniation of L4/L5 will compress L5 root (always one root below) |
|
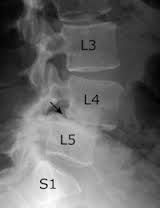
Shown here s spondylolithesis (which a bone (vertebra) in the spine slips out of the proper position onto the bone below it)
Causes what clinical condition? |
Lordosis
can also occur b/c of pregnancy |
|
|
________________ exaageration of thoracic curvature, in erderly people due to, ____________
|
Kyposis- Osteoperosis
|
|
|
Fall or a blow on the DORSAL aspect of flex wrist leads to --distal fragment of the radius is __________ displaced
Fall or Blow leading to the extension of the hand leads to this.....distal fragment of the radius is __________ displaced |
Fall on Dorsal aspect of hand = Smith's fracture, distal fragment of the radius is anteriorly displaced
Fall or Blow leading to the extension of the hand leads to this Colles fracture = distal fragment of the radius is posteriorly displaced |
|

Fall onto hand when palm is abducted = _____________ fracture
Proximal fragment may undergo ___________ Clinical signs: deep tenderness in anatomical snuffbox |
Fall onto hand when palm is abducted = SCAPHOID fracture
Proximal fragment may undergo avascular fragment |
|
|
Fistfight leads to necks of the metarcarpal bones fractured -
|
Boxer's fracture
2nd or 3rd professional 4th or 5th unskilled |
|
|
Avulsing the attachment of the extensor digitorum tendon to the base of the distal phalanx will lead to what clinical symptom?
|
Inabilty to extend the distal interphalangeal joint
|
|
|
Name the rotator cuff muscles--where will disclocation most likely occur at shoulder?
|
Supraspinatus
Infraspinatus Teres minor Subscapularis disclocation most likely occur at inferiorly at shoulder |
|
|
Abduction of upper limb
Name muscle & nerve responsible: 0-15 (initation) 15-horizontal Above horizontal |
0-15 (initation) : Supraspinatus -- suprascapular n.
15-horizontal : deltoid -axillary nerve Above horizontal : serratus anterior- long thoracic TRAPEZIUS -accessory nerve The accessory nerve innervates the trapezius which is the muscle responsible for elevating the acromion of the scapula, also known as the tip of the shoulder. |
|
|
A painful arc of abduction/ pain when raising arm is due to what condition ?
And, if you were to isolate this condition to one tendon, which one would you pick? |
A painful arc of abduction/ pain when raising arm is due = subacromial bursitis
Calcification/inflammation or trauma to SUPRASPINATUS tendon (responsible for initiation of abduction) |
|
|
Inflammation to the bursa near tendon where triceps brachi attach =
|
Subcutaneous Olectranon Bursitis
Olecranon Bursa provides some mobility to the skin |
|
|
A patient comes to you complaining of pain when opening a door or lifting a glass.
His pain is felt over the lateral epicondyle and radiates down the posterior aspect of forearm. Which muscles are likely affected? And what tendon do all these muscle share in common? |

Common EXTENSOR Tensonr
Any of the muscles that start with "extensor" in forearm The point, is when you see lateral epicodylitis = EXTENSOR inflammation See how her hand is extended. Serena Williams is sure to walk in to your clinic one day. |
|
|
Medial epicondylts -- inflammation of the ..... TENDON
Which muscles may be affected? |
Medial epicondylts -- inflammation of the common FLEXOR TENDON
"P-F-P-F" muscles: Pronatore teres, flexor carpi radialis, palmaris longus, flexor carpi ulnars |
|
|
Blockage of Subclavian or Axillary Artery can be bypassed b/w anatostomoses b/w branches of __________________ & ____________
Name the branches of each |
Blockage of Subclavian or Axillary Artery can be bypassed b/w anatostomoses b/w branches of Thyrocervical and Subscapular
Thyrocervical (branch going across neck & above scapula) --Transverse cervical artery -- Suprascapular Subscapular artery -- Subscapular --Circumflex scapular artery |
|
|
Cubital fossa
Contents from Lateral to Medial Area Subcutaneous venous structures from Lateral to Medial Area --Which of these veins is site of venipencture (b/c it's not accompanied by nerve) |
Contents from Lateral to Medial Area
Bicipital Tendon Brachial Artery Median Nerve Subcutaneous venous structures from Lateral to Medial Area Cephalic Vein ****** Median Cubital VeIN* Basilic vein |
|
|
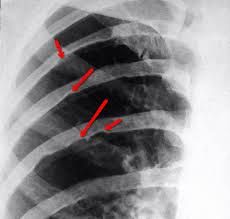
Patient comes in with
Decreased sensaation in lateral 3.5 digits (so everything innervated by the...) Fingers have difficulty opposing each other These are symptoms of carpal tunnel syndrome. Often involves dislocation of _____________ bone & __________ nerve |

carpal tunnel syndrome.
Often involves dislocation of LUNATE bone (outlined in red) & median nerve |
|
|
Bending/ the proximal interphalangeal joints (making an 'L' with one finger tests what
Bending/ the distal interphalangeal joints tests what |
Bending/ the proximal interphalngeal joints (making an 'L' with one finger tests what = Flexor digititorum superficialis
Bending/ the distal interphalangeal joints tests what = = Flexor digititorum profundus |
|
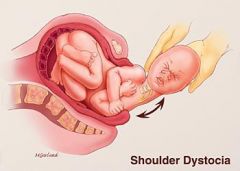
Excessive increase in the angle between neck and shoulder, involves injury to what part of the brachial plexus?
|
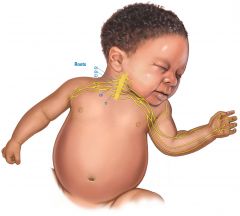
C5, C5 roots or SUPERIOR trunk -= upper brachial plexus
Look how the c5, c6 is stretched :( in this super cute baby :( Why did they make this baby sooo cute . Note that OVER stretching causes the damage. So overstreching the left neck will cause symptoms on left side-- (paralysis of muscles and shoulders supplied by C5 & C6 spinal nerves of upper trunks) |
|
|
Upper brachial palsy
adducted shoulder (b/c you can't abduct anymore b/c of loss of supraspinatus m. function) Medially rotated arm (no infraspinatus function) extended elbow Involves denervation of what nerves Where would you find loss of sensation? |

Involves denervation of what nerves:
nerves supplied by C5, C6 or superior trunk so -muscultaneous n. -suprascapular n. -axillary Think of denervation of musculocutaneous nerve-- loss of sensation on shoulder -- so lateral aspect of upper limp Where would you find loss of sensation? |
|
|
Suddenly pulling or stretching your hand during a fall from a tree or stretching a baby's arm may lead to loss of sensation in MEDIAL arm and fingers (that's pinky & 4th digit) . This involves injury of what nerves?
What other condition can also lead to the same symptoms? |
Injury of lower roots & trunk (C8 & T1 roots of inferior trunk)
This involves combination lesion of ULNAR + MEDIAN nerve. What other condition can also lead to the same symptoms? Thoracic outlet syndrome May include Horner's syndrome (only b/c of thoracic outlet syndrome which causes pressure on C8-T1) |
|
A tumor at this site (apex of lung) may result in what syndrome?
What will be symptoms patient may exhibit? |

A tumor at apex of lung = Pancoast tumor & may cause pressure on LOWER TRUNK of brachial plexus (C8-T1).
Leads to Thoracic outlet syndome -also possibly via pressue on subclavian artery by CERVICAL rib. --Remember, lower brachial plexus injury relates to pain down the MEDIAL side of FOREARM --atrophy of intrinsic hand muscles (due to the lesion of the ulnar nerve, from lower trunk) Also Horner's sydndrome (ptosis, miosis & anhydrosis) b/c it affects sympathetics passing by. |
|
|
injury to musculocutaneous nerve (from lateral cord) greatly weakens what actions?
|
Rmbr, injury to musculocutaneous nerve is included in Upper Brachial Palsy (waiter's tip), so patient will have trouble in flexion & supination
Just like upper brachial palsy lead to lateral anesthesia...Denervation of musculocutaneous nerve affect so lateral aspect of upper limp |
|
|
Which artery is used for cardiac catherization?
Describe the catheter's course to heart (which ventricle will it end up in) |
Which artery is used for cardiac catherization?
Femoral artery Femoral Artery --> External Iliac--> Common iliac---> Aorta--> LEFT ventricle (rmbr, this is arterial blood flow, & aorta connects to left ventricle) |
|
|
Fractures of the femoral neck (common in elderly women w/ osteoperosis) leads to what symptoms in lower limb?
|
Shortness & lateral rotation of lower limb (recall that femur is usually posteriorly dislocated in femur fractures)
|
|
|
Neck fractures of the femur (transcervical fractures) disrupts blood supply to the head of the femur via __________________ (from ________ artery).
How would you describe resulting condition of femoral head? |
Neck fractures of the femur (transcervical fractures) disrupts blood supply to the head of the femur via retinacular (from medial circumflex femoral artery).
How would you describe resulting condition of femoral head? Avascular necrosis = the death of bone tissue due to a lack of blood supply. |
|
|
Injury of WHAT nerve will lead to lack of dorsiflexion in foot (and possibly lack of plantar flexion also?)
|
SCIATIC NERVE injury, will lead to lack of dorsiflexion in foot ("foot drop")
This could be due to any gluteal injection OUTSIDE of the upper lateral quadrant. The upper lateral quadrant is only safe area in butt. |
|

Say you're shadowing in ER. Patient comes in, after a head on collision while a front-seat passenger. He's clutching his hip. You know enough to suspect a hip dislocation involves the femur. (That's something...)
If you had to pinpoint it down, this collision likely led do a fracture of WHAT BONE (find it on the X-ray) & WHAT Ligament torn? Describe how femoral head MOST commonly dislocates in hip dislocations |

POSTERIOR hip dislocations most common.
This is a fracture of the ISCHIUM Femoral head is driven POSTERIORLY out of the acetabulum & tears the ISCHIOFEMORAL lig. This leads to shortening & medial rotating of the limb. |
|
|
You already know that posterior dislocation of hip is most common. This actually also may injure the superior gluteal nerve.
1. This nerve will lead to paralysis of what muscle(s) ? 2. A patient suffering from superior gluteal nerve will have trouble in abducting the pelvis & in abduction of the thigh. Is the ipsi or contra-lateral side to the nerve injury display symptoms? |
1. Denervation of superior gluteal nerve = paralysis of gluteus medius + gluteus minimi
2. Contra-lateral side display symptoms. Just requires you to understand that when you lift one leg, the action of the CONTRALATERAL gluteus medius + gluteus minimi m stabilizes you. |
|
|
Patient presents with trouble climbing stairs & standing from a seated position.
Weakened hip extension is due to injury of what nerve? |
Injury to INFERIOR gluteal nerve (gluteus max m.)
|
|
|
Carcinoma of the breast (malignant) leads to enlargement & shortening of which ligaments/
|
SHORTENING OF suspensory (Cooper's ligaments)
|
|
|
Most lymph, especially from the lateral breast quadrants drains to the _______________ Lymph nodes
Medial breast quadrants drains to the ____________ OR to _____________ |
Most lymph, especially from the lateral breast quadrants drains to the AXILLARY Lymph nodes , initially to the anterior (pectoral nodes)
Medial breast quadrants drains to the PARASTERNAL Lymph nodes OR to THE OPPOSITE BREAST |
|
|
Know
Serratus Anterior, innervated by _____________ Nerve Denervation: ____________ Condition |
Serratus Anterior, innervated by LONG THORACIC Nerve
Denervation: shoulder blade, or shoulder bone, protrudes from a person's back in an abnormal position (winged scapula) |
|
|
Radical mastectomy may injure the intercostobrachial nerve leading to
|
skin deficit of medial arm
|
|
|
The intercostal blood vessels (vein, nerve, arteries) run between the __________- & ___________ muscles
Of these, which are most vulnerable? |
The intercostal blood vessels (vein, nerve, arteries) run between the internal intercostal & innermost intercostal muscles
Of these, which are most vulnerable? V A N The intercostal nerve & posterior intercostal artery b/c neither are covered by ribs. |
|
Shown here is a patient's xray & let's just pretend at the moment he's INSPIRING. There is paralysis of half of the diaphragm.
This may result from injury of what nerve? In this case, is the left or right phrenic nerve injured? |
paralysis of half of the diaphragm = injury of phrenic nerve
In this case, is the RIGHT phrenic nerve is injured. During inspiration, the dome of the diaphgram of the the injured side will RISE instead of descending, b/c it;s being pushed up by abdominal visceral. |
|
|
An anterior hip dislocation (less common) may cause injury of WHAT nerve?
Describe the symptoms. |
An anterior hip dislocation (less common) may cause injury of OBTURATOR nerve.
The obturator nerve supplies upper medial thigh. Symptoms: difficulty in adduction of thigh (rmbr, all the adductor muscles are located in the upper medial thigh) Decreased sensation over upper medial thigh |
|

You'll need this slide if you wanna be a physician qualified to take care of Olympians (pay day!)
You've just been hired by the Russian team to take of the star runner above, Andrea "Tibby" Hamstring (she was 'born' for this) Unfortunately, she has suffered from an avulsion fracture with her hamstring muscles affected. The hamstring muscles allow Tibby to accomplish 1.) extension of the hip joint (stretching out upper thigh) & semimembranous specifically allows flexion of knew joint as she's doing for her back leg. 1.) In an X-ray, the hamstring tendons will be torn at what site? 2.) Name the hamstring muscles 3. What nerve supplies the hamstring muscles? |
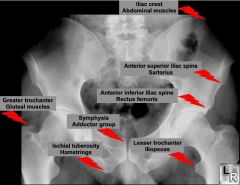
1.) In an X-ray, the hamstring tendons will be torn at what site? At Ischial tuberosity (what you sit on)
2.) Name the hamstring muscles: Biceps femoris, semimembranous, semitendenous 3. What nerve supplies the hamstring muscles? Tibial Nerve (Her name is TIBBY Hamstring!") |
|
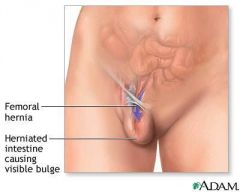
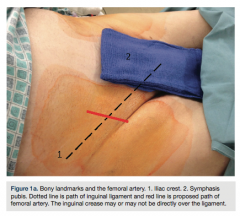
A female patient presents with a swelling in the upper thigh lateral and inferior to the pubic tubercle. She is diagnosed with a femoral hernia. The femoral hernia passes BELOW the inguinal ligament & protrudes through the ____________ opening into the superficial fascia.
If you decide on a surgical treatment, what artery do have to look out for? |
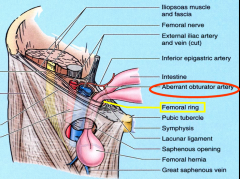
The femoral hernia passes BELOW the inguinal ligament & protrudes through the saphenous opening, an opening into the fascia lata, into the superficial fascia.
If you decide on a surgical treatment, what artery do have to look out for? Aberrant obturator artery |
|
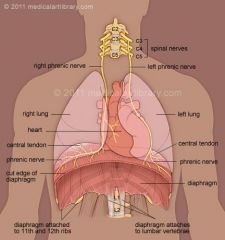
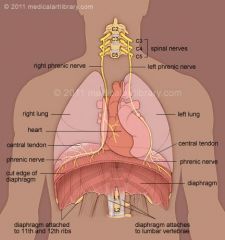
The phrenic nerve, arising from branches of C3-C5 nerves, lies in front of WHAT lateral vertebral muscle?
The phrenic nerve lies _____________ to the root of the lung. The phrenic nerve innervates the pericardium, mediastinal and diaphragmatic pleurae (sensory innervation) & motor innervation to the diaphgram. |
The phrenic nerve, arising from branches of C3-C5 nerves, lies in front of the anterior scalene muscle
The phrenic nerve lies ANTERIOR to the root of the lung. The phrenic nerve innervates the pericardium, mediastinal and diaphragmatic pleurae (sensory innervation) & motor innervation to the diaphgram. |
|
|
Does the vagus lie posterior or anterior to the root of the lung?
|
The vagus lies posterior to the root of the lung?
|
|
|
This mnemonic describes openings of the diapragm
Righteously, I 8 10 EGGS in Vegas AT 12 from a Goose What else travels with the following structures at these thoracic levels? Inferior Vena + (Left or Right Phrenic nerve?) Esophagus + which nerves + which vessels? Aorta + which vessels? |
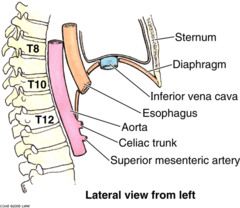
Righteously, I 8 10 EGGS in Vegas AT 12 of a Goose
Right Phrenic Nerve+ Inferior Inferior Vena Cava - T8 Vagus + Esophagus - T10 Azygous (Goose) Vein + Aorta + Thoracic Duct-T12 |
|
|
Choose ONE letter.
Mitral valve failure may cause cardiac hypertrophy: a.) Right ventricle enlargement b.) Left ventricle enlargement c. Left atria enlargement d. Right atria enlargement And may compress what structure? What symptoms may a patient with mitral valve failure present with? |
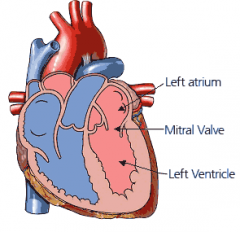
Mitral valve failure may cause:
Left atria enlargement -- makes sense, blood will accumulate in left atrium Left atria enlargement may compress the esophagus/ symptoms: dysphagia |
|
Understand that a heart murmur is heard DOWNSTREAM from the valve.
A stenosis is orthograde direction from valve An insufficient is retrograde from the valve ( b/c regurgitation of blood back to previous compartment) Match each site with a letter. Knowing this, where best will you hear: a.) mitral stenosis? b.) aortic stenosis? c.) aortic insufficiency ? d. mitral insufficiency? e. triscuspid insuffiency? |
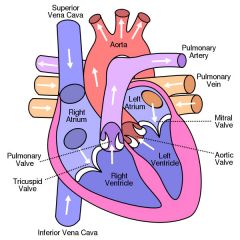
Knowing this, where best will you hear:
a.) mitral stenosis? M b.) aortic stenosis? A c.) aortic insufficiency ? M d. mitral insufficiency? P e. triscuspid insuffiency? T |
|
|
Conducting system of the heart:
Sinoatrial node ---> Atrioventricular Node -> Atrioventricular bundle of His (Right band passes down moderator band, while left is on left side) Of these structures: Which one is located .... near the coronary sulcus on the diaphragmatic or posterior surface of the heart? ....near the opening of the superior vena cava? |
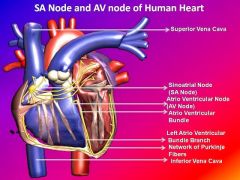
Coronary sulcus on the diaphragmatic or posterior surface of the heart = coronory sinus (only visible on posterior view= site of AV node
Site of SA node = near the opening of the superior vena cava? |
|
|
How the right coronary artery contribute to blood supply of the heart.
Right Coronary Artery Branches: What area does each branch supply? Anterior Cardiac Branches supplies..... [region] Nodal branches ....... Marginal Artery .... Posterior interventricular artery..... |
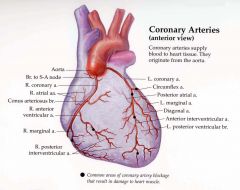
Anterior Cardiac Branches supplies ....right atrium
Nodal branches .... SA & AV node Marginal Artery ...... right VENTRICLE Posterior interventricular artery..... Diaphragmatic surface of BOTH venricles , posterior 1/3 of lower septum |
|
|
Which artery supplies the left atrium and left ventricle?
|
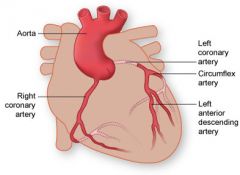
The CIRCUMFLEX artery of the left coronary artery
Notice how the circumflex artery of the LCA is the only artery willing to circumvent the heart to around the atrioventricular groove to anastomose with the RCA. Making circles to make peace with the RCA! |
|
|
This artery-most common place of MI-- supplies branches to the
...anterior 2/3 of the muscular lower (IV) septum ...anterior heart wall ...bundle of His ...apex of heart |
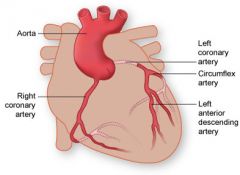
Anterior inter-ventricular artery of the left coronary artery
|
|
|
Fill in with Right coronary artery or left coronary artery
What artery supplies the AV node ? AV bundle ? SA node? |
AV node ? RCA (nodal branches)
AV bundle ? LCA (anterior descending/interventricular artery) SA node? RCA (nodal branches) |
|

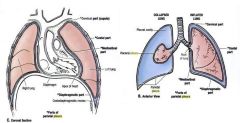
This is Priscilla (she looks prissy, let's be honest). She's got atrial septal defect.
What causes atrial septal defect? Specifically what to septum fail to fuse? Postnatally, what type of shunt results from atrial septal defect? |
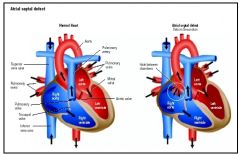
What causes atrial septal defect?
Failure of foramen ovale to close Specifically what to septum fail to fuse? Failure of septum "prisci"cella: PRImum & SECundum Postnatally, what type of shunt results from atrial septal defect? Left--to-->right Again, her picture is meant to help you. Look at Priscilla, she's not blue! It's a non-cyanotic shunt |
|
|
Ventricular septal defect is most common congenital defect, due to failure of membranous portion of the muscular portion of the ventricular part to fuse.
Describe direction: This is a __________-to-_____________ shunt, leading to _(left or right?)____ventricular hypertrophy |
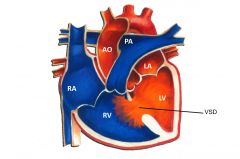
It kinda makes sense that ventricular septal defect is a non-cyanotic & most common type. It fits observation: There's a lot of ppl in this world who might not even know that they have a septal defect b/c their skin complexion is normal.
As a typical non-cyanotic condition: This is a left- to-right shunt, leading to right ventricular hypertrophy |
|

Tao & Lerene
You're a third yr-first day of rotation in Ob/Gyn...in India! (You decided to do your away rotation far away!) You've just delivered this baby, Tao, who was quite premature (look at how small it is!) The mother, Lerene, unfortunately was just recovering from a present rubella infection & the child was diagnosed with patent ductus arteriosus. PAD is a result of a failure of what connection between what 2 vessels? Surgery needs to happen. When you ask Lerene for consent to operate, what possible nerve injury (& clinical manifestations) should you warn her of? |
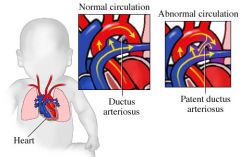
PAD = failure of TAO - pulmonary trunk & aorta
You BETTER Inform Lerene that the "LEft REcurrent Nerve" may be cut, leading to hoarseness (paralysis of the ipsilateral vocal cord) The surgery was successful! Maybe Tao will become a superstar singer! |
|

You're on the night shift with an attending who likes to pimp like he owns you.
He passes you a chart of a patient suffering from an aneurysm of the aortic arch, and grimaces like he always does when he's about to ask u a random question he sure you'll miss, junior. He asks "Paralysis from an aneurysm of an aortic arch likely results in the left or right vocal cord?" The super smart nurse comes and whispers to you, that the patient may have been misdiagnosed earlier. She thinks it's an aneuryms of the thoracic aorta. Where would you palpate to verify before you tell your attending ? |
Left vocal cord.
Aortic arch aneurym ---> Left recurrent layrngeal nerve--> Compression of the left recurrent laryngeal nerve leads to coughing, hoarseness & paralysis of the ipsilateral vocal cord. Aneurysm of thoracic aorta: palpate the trachea at the STERNAL NOTCH (T2) |
|
|
Abdominal aortic aneurysm typically occur just above the bifurcation at the level of ___________ & cross by __________
Pulsation of a large aneurysm can be detected where.... |
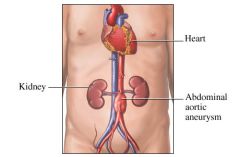
Abdominal aortic aneurysm typically occur just above the bifurcation at the level of L4 & cross by the third part of the duodenum.
Pulsation of a large aneurysm can be detected to the LEFT of the midline at the umbilical region. Don't be that third year that palpates for an abdominal aneurysm on the right side. You WILL be called out. |
|
Above is the X-ray of a young patient suffering from a congenital narrowing of the aorta (coarctation of the aorta), with the characteristic rib notching.
Coarctation of the aorta is a narrowing of the aorta distal to the ____________ artery What's the cardinal clinical sign? Which arteries provide collateral circulation? |
Coarctation of the aorta is a narrowing of the aorta distal to the left subclavian artery
What's the cardinal clinical sign? Higher blood pressure in the upper limb, compared to the lower limb. - Hypertension in upper extremities, weak pulses in lower extremities Which arteries provide collateral circulation? The intercostal arteries. See how they connect the internal thoracic artery & descending artery. The dilation of the intercostal artery --> ribbed notching |
|
|
Aspiration of foreign bodies more likely to enter _______________ & pass into __________ lobe.
|
Aspiration of foreign bodies more likely to enter RIGHT primary bro nchus & pass into middle or lower lobe.
In the vertical position, usually falls into posterior or RIGHT inferior lobe. |
|
|
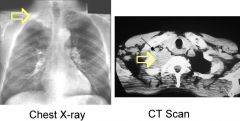
Pneumonia = inflammation of lung.
Name symptoms How would chest x-ray appear? Enlargement of which lymph nodes are expected |
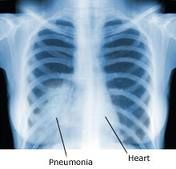
Cough, chest pain, fever & difficulty in breathing.
Enlagerment of bronchomediastinal lymph nodes |
|
|
Bronchogenic carcinocoma spreads first to.... _____________
And may lead to what other syndrome, which which symptoms |
Bronchogenic carcinocoma spreads first to (bronchomediastinal) thoracic lymph node.
Thoracic outlet syndrome : Pressure of lower roots & trunk (C8 & T1 roots of inferior trunk) & atrophy of intrinsic hand muscles like Horner's syndrome (miosis, ptosis, hemianhydrosis) dilation of the head and neck veins |
|
|
Describe the exact location to listen to BREATH sounds of these lobes
Superior Lobes, left + right Middle lob of right lung (only the RIGHT lung has 3 lobes) Inferior lobes of both lungs.... |
Superior Lobes, left + right :
above the 4th rib for the right lung above the 6th for the left lung (as always right-hand dominates!) Middle lob of right lung (only the RIGHT lung has 3 lobes) - b/w 4th and 6th rib Inferior lobes of both lungs -- posterior chest wall |
|
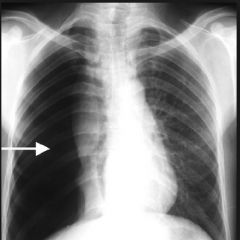
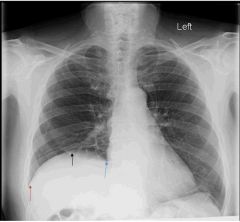
A patient comes in with a stab wound of the thoracic wall that has pierced the parietal pleura, & the parietal pleura has opened to outside air.
Patient is diagnosed with an open pneumothorax. The X ray of the anterior thoracic wall is shown during inspiration. On which side, was the person stabbed? |
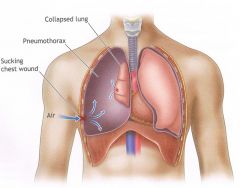
Stab was on right side.
Air moves freely. During inspiration, air will enter the chest wall and the mediastinum will shift toward the other side. |
|
|
Cosdiaphgramatic recess = deepest place in pleural cavity
Where costodiaphragmatic recess at the midclavicular line, the mid axillary line, and the paravertebral line? |
Going down the body. It's within these spaces you can insert a needle.
Midclavicular line: b/w ribs 6- 8 Mid axillary line: b/w ribs 8-10 and the paravertebral line: 10-12 |
|
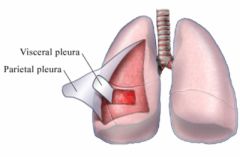
Which of these pleura is sensitive to pain, temp, touch & pressure due to somatic sensory innervation?
Which of these is only sensitive to stretch, & has an autonomic nerve supply from pulmonary plexus? |
Parietal pleura: pleura is sensitive to pain, temp, touch & pressure due to somatic sensory innervation
Visceral: sensitive to stretch, & has an autonomic nerve supply from pulmonary plexus Makes sense to me because b/c pleura is visceral, location-wise it's "insulated" & thus not sensitive to general sensibilities & it's closer to the pulmonary plexus |
|
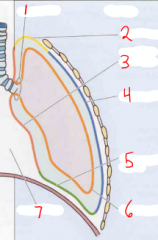
Associated the numbered areas 3, 4,5 with a particular nerve supply.
|
Surface area of visceral pleura has shrunk due to collapsed lung here..but not main point
3-Mediastinal Pleura = Phrenic Nerve 4-Coastal Pleura = Intercostal nerves (block here, way to decrease pain) 5-Diaphgramtic pleura= Phrenic n. Note you want to target the parietal pleura for pain relief. |
|
|
Structures near the sternal notch, posteriorly situated...
In upper part Further down low |
Structures near the sternal notch, posteriorly situated...
In upper part: Left brachiacephalic vein Further down : Aortic arch |
|
|
The thoracic duct drains into the ____________________ vein
The right lymphatic duct drains into which 2 veins ____________ & ______________ The thoracic duct drains the entire, EXCEPT what area? |
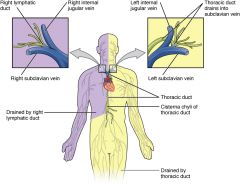
The thoracic duct drains into the Left Subclavian vein
The thoracic duct drains the entire, EXCEPT what area? The right upper limb hemisphere, which drains to the right lymphatic duct |
|
|
Name 3 prime sites where ingested foreign bodies may lodge in the esophagus
|
"Think 4-5-6" (The 'think' is part of this b/c you need to remember it's THORACIC 4/5)
C6 - junction of pharynx with esophagus T4-T5 -- where aortic arch and LEFT main bronchus (think about this in cadaver, aortic arch was on left side) & naturally T10: we already know this! (rmbr...Righteously, I 8 10 EGGS in Vegas AT 12 of a Goose: Vagus + Esophagus - T10) Opening of Esophageal Hiatus |
|
|
Ok, quadrants:
Liver & gallbladder Stomach & Spleen Cecum & Appendix End of descending colon & sigmoid Colon |
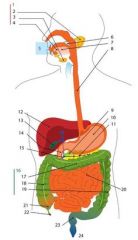
This took me forever to learn for some reason...
Liver & gallbladder -- Right upper Quadrant Stomach & Spleen --Left Upper Quadrant Cecum & Appendix -- Right Lower Quadrant End of descending colon & sigmoid Colon -- Left Lower Quadrant |
|
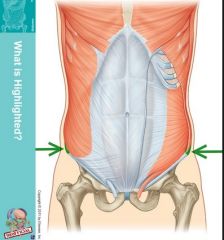
Alright, let's discuss nerve supply of the anterior abdominal wall.
All nerves and deep blood vessels lie in the neurvoscaular plane .... located b/w which muscles? The L1 iliohypogastric & ilioinguinal nerves can be anesthetized by injecting 1 inch superior to what site marked on this patient (highlighted) |
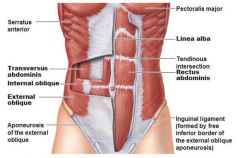
The L1 iliohypogastric & ilioinguinal nerves can be anesthetized by injecting 1 inch superior to the ANTERIOR superior iliac spine
All nerves and deep blood vessels lie b/w the INTERNAL Oblique & Transversus Abdominis musclces. Arteries termed "superficial xzy" supply skin. Other arteries, "deep arteries" like in this neurovascular plane. |
|
|
The __________________ fascia is the FIRST structure which is crossed by any abdominal hernia
|
The TRANSVERSALIS fascia is the FIRST structure which is crossed by any abdominal hernia
|
|
|
Difference b/w indirect & direct inguinal hernia
http://youtu.be/wAzXSqGybvE An indirect inguinal hernia passes through __________ ring. Which of these - direct or indirect-- descends into the scrotum? Describe both passages in relation to the inferior epigastric vessels. (Remember the inferior epigastric vessels are deep arteries, that lie in between the internal oblique and transversus muscles) |
An indirect inguinal hernia passes through deep inguinal ring. An indirect inguinal hernia passes lateral to the inferior epigastric vessels.
Which of these - direct or indirect-- descends into the scrotum? The Indirect descends into the scrotum (look at video) The direct, just DIRECTLY protrudes into the ABDOMINAL hernia. The direct passes MEDIALLY to the inferior epigastric vessels |
|
|
Hernial sac: Is it a pouch of peritoneum or transversalis fascia?
|
Hernial sac: Is a pouch of peritoneum.
|
|
The lesser omentum. Ummm.
Consists of 2 ligaments: It includes gastric vessels & the portal triad, which consists of: Inferior to this, will the be 1st part of the duodenum Superiorly, the caudate lobe of the liver. |
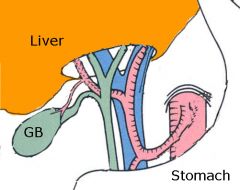
Consists of 2 ligaments: hepatoduodenal & hepatogastric ligament
It includes gastric vessels & the hepatoduodenal enclosing the portal triad, which consists of, anteriorly to posteriorly situated Bile Duct (also most lateral) Proper hepatic artery Portal Vein Inferior to this, will the be 1st part of the duodenum |
|
|
Female comes in suffering from abdominal pain, diarrhea, fever. She's later diagnosed a pelvic abcess.
This is the space of the pelvic abscess location: it is he vertical position of the female body b/w the RECTUM & CERVIx. |
Rectouterine pouch (RECTUM & CERVIx OF UTERUS)
This is the lowest portion of the female peritoneal cavity. Ectopic (abdominal) pregnancy can also occur in the rectouterine pouch Know that, in order to access it, you have enter via the POSTERIOR vaginal fornix (so posteriorly) --just like your milk boy will try to sneak in via the back door to hang out with your daughter's vagina--IT AIN'T happenin'....) |
|
|
The _________ collateral ligament is a broad flat band extending from the medial epicondyle of femur to the medial shaft of tibia
-Does this collateral ligament attach to the ipsilateral meniscus? -Disruption of this ligament will lead to what clinical manifestations? The _________ collateral ligament is a broad flat band extending from the lateral epicondyle -Does this collateral ligament attach to the ipsilateral meniscus? -Functions of this ligament: |
Tibial Collateral Ligament - Medial
Firmly attaches to the medial meniscus Disruption: It limits extension and abduction of leg. Fibular Collateral Ligament - Lateral Does NOT attach to the lateral meniscus Disruption: It limits extension and adduction of leg. (The lateral ligament doesn't wan't the leg to go to far medially--Lateral ligament says "stay on MY side") |
|
|
Describe the symptoms of associated with tearing of the anterior or posterior cruciate ligaments?
|
I think of the crucial ligaments as "book ends" for the femur--they keep the femur from moving to far beyond range.
Tearing of the anterior cruciate ligament: excessive displacement of the femur anteriorly Tearing of the posterior cruciate ligament: excessive displacement of the femur posteriorly |
|
|
The patellar reflex
Afferent & efferent limb: ________ nerve (spinal cord levels too) |
The patellar reflex
Afferent & efferent limb: femoral nerve nerve (spinal cord levels L2-L4) |
|
|
The Achilles tendon reflex (tapping the calcaneal tendon)
Afferent & efferent limb: __________nerve (spinal cord levels) |
The Achilles tendon reflex (tapping the calcaneal tendon)
Afferent & efferent limb: TIBIAL nerve (spinal cord levels S1-S2) |
|
|
Sprained ankle is nearly always an Inversion injury involves _________________ ligament
Pott's fracture (a fracture-dislocation of ankle joint) -Eversion injury involves _________________ |
I think of it as the overstretching cause the damage. Inversion will "overstretch" lateral side--dunno if that's true, but it makes it really easy for me.
Inversion injury involves anterior talofibular (lateral) ligament on foot Eversion injury involves deltoid ligament |
|

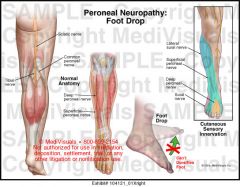
Rmbr, how the sciatic nerve injury leads to foot drop?
Injury of a fracture at this above on the fibula(what is this site?) will cause injury to WHAT nerve--the result also being foot drop |

Fracture at fibular neck
Injury to common fibular nerve, branch of the sciatic nerve Associated with loosing sensation of dorsum of foot |
|
|
A patient comes in with a ruptured Achilles tendon.
Which action will patient be unable to do? Which muscle(s) will be affected? |
Ruptured Achilles tendon.
Patient will be unable to do plantar flexion Muscles affected: gastro, soleus & plantaris |
|
|
Sciatic nerve divides into two branches common fibular nerve (loss--> foot drop) & tibial nerve.
What is the symptoms for injury of tibial nerve & which muscles are affected in popliteal fossa? |
Tibial Nerve:
Loss of Plantar Flexion (inability to stand on toes) Muscles affected: gastro, soleus Note that in common peroneal nerve damage --- loss of sensation is on dorsum of foot But in tibial nerve damage - loss of sensation & paralysis of intrinsic muscle on the sole of the foot. (Tibial, t for "terra" - your sole touches the terra) |
|
|
Polythelia is an accessory nipple resulting from persistence of fragments of the mammary line (milk line).
|
May develop anywhere along the original mammary line but usually appear in the axillary region
|
|
|
Dermatome is the dermis AND associated spinal nerve.
Dermis of the face and head is derived from neural crest! |
Dermatome (Segmental) patterns result from patterning of mesodermal elements. These patterns form independently of the patterns of ectoderm formation!
|
|
|
Name the major source of hematopoieses during 3 trimesters of pregnancy
|
Spleen/ Liver & Bonemarrow
|
|
|
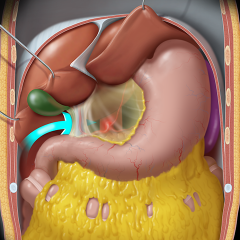
Posterior gastric ulcer may erode throguh the posterior wall of the stomach in to the ____[structure]____________________
Most important, posterior gastric ulcer will affect what organ & may lead to erosion of what artery? |
Posterior gastric ulcer may erode throguh the posterior wall of the stomach in to the lesser perinoteal sac.
Most important, posterior gastric ulcer will affect what organ & may lead to erosion of what artery? Pancreas Splenic Artery |
|
|
Congenital diaphragmatic hernia: Describe this condition.
What do infants with this disease usually die of? |
Protrusion of intestine through hole in diaphragm through a POSTEROLATERAL DEFECT in diaphgram.
It is in seen in INFANT who usually die of lung hypoplasia. |
|
|
Sliding hiatal hernia (usually no symptoms, but if so: heartbone) is caused by the hernia of cardia of the stomach into the thorax through the esophageal hiatus of the diaphgram ( rmbr, at T10)
What structure may this damage? |
Vagal trunks.
Change the mnemonic & it's easy! Righteously, I 8 10 Eggs in VEGAS at 12 from a Goose @ T10: Esophagus, runs with Vagus nerve! |
|
|
Merkel's diverticulum is a congential anomaly = persistent portion of _____________________ located in the .....
What's this 2 business with Mekel's diverticulum?? |
Persistent portion of vitellointestinal duct, also known as the omphalomesenteric duct, is a long narrow tube that joins the yolk sac to the midgut lumen of the developing fetus.
Mekel's is generally 2 feet long in the ILEUM, within 2 feet of ileocecal valve until the SMA supplies it. |
|
|
Name all (3) of the features of the large intestine:
|
Haustra (Sacculations)
Appendices epiploid Tenaia coli, which meet together at base of appendix |
|
|
Name all the structures that lack a mesentery in the gut
|
KRUS - 1 retro
Kidney Rectum Ureter Suprarenal glands PADD -- 2nd Retro (Pancreas, Ascending colon, Descending colon, Duodenum) Everything else will be intraperitoneal position. |
|
|
They guy who played Frodo in LOTR had appendicitis--I clearly remember him discussing it (strangely) on Letterman's
The first pain he likely felt was dull, due to afferent pain fibers entering the spinal cord at the level of _______. Where was his first pain? |
The first pain he likely felt was dull, due to afferent pain fibers entering the spinal cord at the level of T10. Where was his first pain?
Dull around the umbilicus. Then later IF Parietal Peritoneum gets involved the pains shifts laterally to the Burney's Point. 2nd Pain is precise & localized at the base of the appendix, between the anterior superior iliac spine & umbilicus. |
|
|
Which intraperitoneal strutures have a great degree of mobility and may thus sometimes rotate around the mesentery, leading to a possible cut-off of blood supply.
|
Jejunum, Ileum & Sigmoid
|
|
|
It's your end of the first week of Indian rotation. Ppl are loving 'cause you're making yourself useful!
One of the midwives presents you a newborn who has not been able to pass a meconium stool within 24-48 hour after birth. At the end of the 48 hours, the baby has even started vomiting bile-stained vomit. What may this child have? & DESCRIBE ETIOLOGY. What may be a possible treatment for the child? |
NBME: newborn who has not been able to pass a meconium stool within 24-48 hour after birth.
You: Hirschsprung's, boooyyaaa! ABSENCE OF POSTGANGLIONIC PARASYMPATHETIC neurons (this is intuitive, b/c that's what's required to poop) Treatment: Removal of colon missing postganglionic parasympathetic neurons |
|
|
Describe the levels at which the following branches of abdominal aorta
Celiac Trunk SMA Renal Arteries IMA |
Get Low aorta: this reminds me the first two structures originates at the LOWER border of T12 (celicac trunk) and the LOWER border of L1
Celiac Trunk: T12 SMA: L1 Renal Arteries: L2 IMA: L3 Common Iliac L4 |
|
|
Name the 3 branches of the celiac trunk.
Which of these branches, further gives off branches that ascend within a ligament of the lesser omentum? |
Common Hepatic Artery
Left Gastric Artery Splenic Artery (tortorous) Think of position organ structures.... (well, I just remembered a stomach and spleen are in the LUQ) Common Hepatic Artery --> Proper hepatic artery --> in Hepatoduodenal ligament of lesser omentum |
|
|
Do you remember what may cause erosion of the splenic artery?
|
The splenic artery is located deep to stomach, that's all.
So penetrating ulcer of the posterior wall of the stomach into the lesser sac may lead to erosion |
|
|
Name branches of IMA..everything else in gut will likely be off SMA.
|
IMA branches. IMA supplies descending colon & superior rectum. ("In My opinion, things are descending down your rectum")
Left colic artery (where your descending colon is) sigmoid arteries superior rectal artery Every other branch in intestine will be branch of SMA |
|
|
Mesenteric ischemia is ischemia that usually involves the SMA and small intestine. It primary affects organs located far away from anastomoses with celiac artery & IMA, so it would likely compromise blood supply to...
|
Pic uploading - no longer working but
Jejunum & Ileum Note that are portions of the right-sided jejunum & ileum are far away from the IMA branches, which supply the leftish descending colon & superior rectum ("In My opinion, things are descending down your rectum") |
|
|
Recount journey of bile as it travels from liver to gallbladder to duodenum.
|
Best to draw pic-uploading not working :(
Bile --> Cystic Duct (w/ common hepatic duct) --> Bile Duct--> Hepatuoduodenal ligament At Head of pancreas, Pancreatic Duct + Common duct = hepatopancreatic ampulla This then drains into posteromedial wall of second part of duodenum |
|
|
The mot common site for impaction of gallstones is the narrowest part of the biliary passages.
What structure is this? To what area does this structure drain to? |
Hepatoduodenal ligament at pancreatic ampulla, draining to the posterior wall of the SECOND part of the duodenum
|
|
|
Gallstones can be lodged in the body or fundus of the gallbladder.
Which gallstones will have easier passage to rectum? |
Gallstones in the fundus are having FUN, and naturally dancing their way to the TRANSVERSE colon --> descending --> sigmoid --> rectum.
Gallstones in the body of the gallbladder are closer to duodenum & may be held at the ileocecal junction, producing an intestinal obstruction https://www.jhmicall.org/Upload/200711131436_07608_000.jpg |
|
|
Sensory innervation of liver, provided by
Paraympathetic inervation of liver, by |
Sensory innervation of liver, provided by RIGHT phrenic nerve (C3-C5)
Paraympathetic inervation of liver, by Vagus nerve |
|
|
Nerve spply of liver + gallbladder
Sympathetic fibers of preganglionic neurons of segments ______ form greater splanchnic nerves |
Sympathetic fibers of preganglionic neurons of segments T5-T9 form greater splanchnic nerves
Celiac plexus is where postganglionic of T5-T9 are located |
|
|
For treatment of portal hypotension, intrahepatic shunts involves anastomeses b/w portal & hepatic vein
For treatment of portal hypotension, extrahepatic shunt involves anastomeses b/w |
Splenic Vein & Left renal vein (all that really needs to be remembered is that stomach + spleen are on left side!)
So splenic vein will connect with left renal vein naturally. And splenic vein drains to portal vein. |
|
|
Which venous anastomoses are important during portal hypertension?
|
Es-pa-re-nza veins reach the portal veins.
Rmbr, how Esperanza showed Quasimodo thru the tunnels?! Esophageal veins --left gastric & azygous (10 eggs in vegas of a goose) Paraumbilical veins ---> anstomoses w/ superior & inferior epigastric veins gets enlarged REctal veins |
|
|
The superior mesenteric artery (lateral) & vein pass anterior to the ________ of the pancreas.
The splenic veins joins with the superior mesenteric vein to form the ___________ vein, which passes posterior to the enck of the pancreas. |
The superior mesenteric artery (lateral) & vein pass anterior to the head of the pancreas.
The splenic veins joins with the superior mesenteric vein to form the portal vein, which passes posterior to the enck of the pancreas. |
|
|
Remember that the tail of the pancreas tickles the spleen! Which part of the pancreas is intraperitoneal?
|
Remember that the tail of the pancreas tickles the spleen! Which part of the pancreas is intraperitoneal?
The tail of the pancreas! |
|
|
Describe blood supply of pancreas:
Head (+ Duodenum) : (1) _________-- arteries, branch of (2) _________-- arteries, branch of Neck, Body Tail of pancreas -- splenic artery |
Head (+ Duodenum) :
(1) superior pancreaticduodenal arteries, branch of gastroduodenal (2) inferior pancreaticduodenal arteries, branch of SMA |
|
|
High-yied
The spleen follows the contour of rib ____ rib ________ = border b/s spleen & kidney |
The spleen follows the contour of rib 10
rib 11 = border b/s spleen & kidney Just think, rib: 9-11 spleen 11-12 kidney |
|
|
At which spinal levels is levels are kidneys located?
|
T12 - L3
123, A kid is 1 cup of t! |
|
|
Ureter is located on the anterior surface of WHAT muscle?
|
Ureter is located on the anterior surface of PSOAS MAJOR muscle?
|
|
|
Adrenal medulla--Catecholamines, Epinehprine & NorEpi--Sympathetic
Tumor of adrenal medulla, tachycardia, sweating. |
Adrenal medulla--Catecholamines, Epinehprine & NorEpi--Sympathetic
Tumor of adrenal medulla, tachycardia, sweating. |
|
|
Rmb, veins are anterior to arteries supplying kidney
|
Rmb, veins are anterior to arteries supplying kidney
|
|
|
What part of urethra is injured to lead to urinary leak?
Where will urine leak to? |
Spongy urethra
Think about a sponge that normally trying hard to soak up the urine (but failing now, due to injury) Urine will leak to the superficial perineal pouch. |
|
|
Syntrophoblast
|
Syntrophoblast is important: it is the part that has contact with the mother. at the uterine lining. It also makes hCG and progesterone. It contains lacunae (little gaps) that hold blood.
|
|
|
what is being imaged in an ultrasound for baby -- it's the...
|
amniotic cavity.
|
|
|
Prenatal: blood pressure is GREATER ON THE RIGHT SIDE OF THE HEART.
|
POSTnatal: blood pressure is GREATER ON THE Left SIDE OF THE HEART.
As usual right hand dominates, first. |
|
|
Ductus arteriosis: know that it comes from distal __#____ aortic arch. Shunts blood from ______ to aorta.
|
Ductus arteriosis: know that it comes from distal 6th aortic arch. Shunts
blood from pulmonary trunk to aorta. |
|
|
Allantois
|
Allantois--> Urachus--> Median Umbilical Cord Ligament
|
|
|
Polyhydramnios: vs.
o Oligohydramnios: |
Polyhydramnios: more than normal amount of amniotic fluid, like annular pancreas
o Oligohydramnios: less than normal amount of amniotic fluid. Can be due to bilateral renal agenesis (both kidneys fail to develop) and urethra blockage (uretal folds prevent urine from exiting). Oligohydramnios is Potter syndrome (deformed limbs, abnormal facial appearance). |
|
|
Posterior neuropore closes week 4. Failure to close:
|
get spina bifida with myeloschisis.
vs... Anterior neuropore closes week 4 (two days before the posterior one closes). Failure to close: get anencephaly. |
|
|
The left pampiniform plexus goes intto the
The right enters.... |
The left pampiniform plexus enters the left renal vein
The right pampiniform plexu enters one enters directly the IVC inferior to the renal vein, perhaps b/c the right kidney is too far down (The right kidney lies lower than the left) |