Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
33 Cards in this Set
- Front
- Back
|
Age-distribution of Hodgkin's Lymphoma.
|
Bimodal distribution:
-Major peak 15-34 -Lesser peak after 55 |
|
|
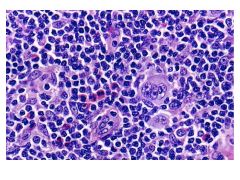
Hodgkin's Lymphoma:
Histologic Features CD Markers Cell Origin (location) |
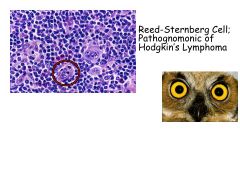
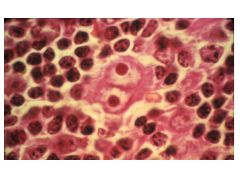
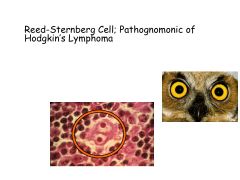
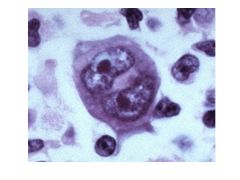
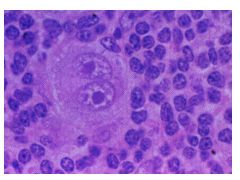
-Multi-nucleate REed-Sternberg Cells (Owl's Eyes)
-Background of normal inflammatory cells (non-malignant) Note: only 1-5% of total tumor mass are R-S cells CD15+ and CD30+ = Hodgkin's B-cells originate at germinal center or post-germinal center (even though fail to express Ig genes!) |
|
|
What is a crippling Ig gene rearrangement? When is it acquired?
|
Acquired during somatic hypermutation and for some reason doesn't result in apoptosis.
Cells are allowed to escape cell death and acquire additional mutations-->malignant R-S cell |
|
|
What causes transformation of R-S cells?
|
This is hypothetical:
EBV (EBV DNA localized in R-S cells) There's more Hodkin's in HIV |
|
|
Hodgkin's Lymphoma:
Presentation |
Cervical LN enlargement
Mediastinal involvement by CT Involvement of spleen |
|
|
Hodgkin's vs Non-Hodgkin's Lymphoma:
Spread |
HL: initially localized at single peripheral LN region; subsequent progression by contiguity within lymphatic system. Contiguous spread!
NHL: Diffuse spread initially |
|
|
Hodgkin's Lymphoma:
Ann Arbor Staging (I-IV) Subscripts (E, S) |
I: Single LN group involved
II: Involvement of 2 or more LN groups on same side of diaphragm III: involvement of LN regions on both sides of diaphragm IV: Outside LN areas (BM, liver) Subscripts: S = splenic involement E = extranodal extension |
|
|
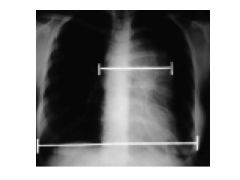
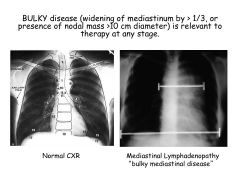
What is bulky disease in HL?
|
Widening of mediastinum by >1/3 of chest diameter
|
|
|
A vs B Symptoms
|
A: absence of constitutional symptoms
B: presence of constitutional symptoms (Fever >38 degrees C, Weight Loss >10% over last 6 mos, Night Sweats) Constitutional syx present with widespread dz. |
|
|
What's the Pel-Epstein fever?
|
Cyclical fever (on and off); pathognomonic of HL
|
|
|
Patient presents with bilateral cervical and axillary LAD.
Complains of malaise, night sweats, loss of weight over last 3 months. What's his Ann Arbor stage? |
Stage IIB (B bc has B syx)
|
|
|
Classical HD vs Non-Classical HD: General
|
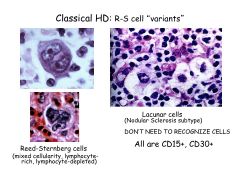
Classical:
RS cells positive for CD15 and CD30 Non-classical: RS cells ARE CD15-, CD30-, CD20+ |
|
|
Lacunar cells are indicative of ________.
|
Nodular Sclerosis subtype of Classical HD
Lacunar cells are RS cells (owl eyes) that undergo shrinkage when cells are fixed. All are CD15+, CD30+. |
|
|
What are popcorn cells?
|
Popcorn cells are lymphocytic histiocyte cells (LH) present in non-classical HD.
Don't need to recognize for exam. |
|
|
What is the only subtype of non-classical HD?
|
lymphocyte predominant
|
|
|
What is the most common subtype of HD?
Age distribution? Presentation? |
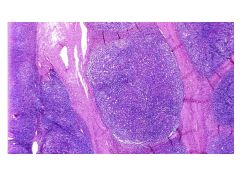
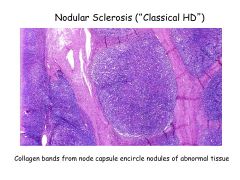
Nodular Sclerosis
Predominates in young adults Presents with cervical and anterior mediastinal involvement in young adult FEMALES> |
|
|
Nodular Sclerosis:
Histologic Features |
Nodular (collagen bands)
Lacunar R-S cells |
|
|
The link with EBV is strongest in this subtype of HD.
|
Mixed Cellularity HD
|
|
|
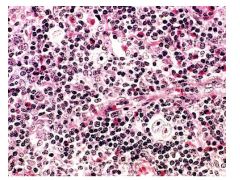
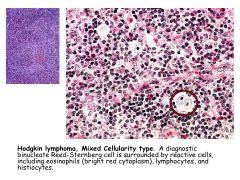
Mixed Cellularity HD:
Histologic Features |
R-S Cells surrounded by a mix of cells (ephils, lymphocytes, histiocytes)
|
|
|
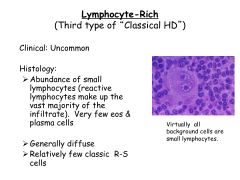
Lymphocyte-Rich HD:
Histologic Features |
R-S cells surrounded by small lymphocytes
|
|
|
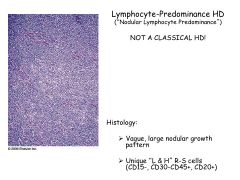
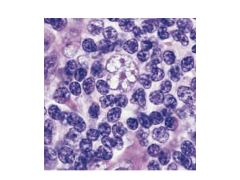
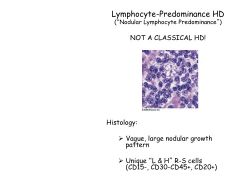
Lymphocyte-Predominance HD:
Histologic Features |
NOT A CLASSICAL HD
Lymphocyte predominance with nodularity (subtle) No R-S cells Popcorn cells (L&H cells) with CD15-, CD30-, CD20+ |
|
|
HD:
Treatment |
ABVD:
Adriamycin - cardiac tox Bleomycin - pulm fibrosis Vinblastine - MT agent Dacarbazine - alkylating Note: Choice depends on stage of dz XRT alone may be adequate for early stage favorable HD, but combined modality tx may be more effective Also, higher doses of XRT are curative, but increase incidence of solid tumors in irradiation field (and inc CAD) |
|
|
What is the most important prognostic variable for HL?
|
Staging!
Early stage cure rates of 90% |
|
|
HD:
Complications of treatment (early vs late mortality) Non-malignant complications |
Early mortality due to HD recurrence
After 15 years, almost all deaths due to secondary malignancy, CV, pulm dz (related to radiation, alkylating agents) Non-malig: Sterility (MOPP) Infectious complications Cardiac/pulmonary complication of mediastinal XRT and chemotx |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|