Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
57 Cards in this Set
- Front
- Back
|
How many cranial bones?
How many bones of face? How many teeth? |
8
14 28 |
|
|
How many fossa in cranium?
What are they and what do they hold? |
3
• Anterior fossa- frontal lobe • Middle fossa- temporal lobe • Posterior fossa- cerebellum |
|
|
Spinal Cord goes through
|
Foramen Magnum
|
|
|
CNS is...
PNS is... |
• CNS— Brain and spinal cord
• PNS— 3 main things: autonomic nervous system, cranial nerves, somatic nervous system |
|
|
Lobes of the brain and major functions...
|
• Frontal – executive functions
• Parietal- sensory • Temporal- Auditory • Occipital- vision • Cerebellum- coordination and balance • Brainstem: Pons, midbrain, medulla. Locked in syndrome when brainstem is damaged , respiratory |
|
|
6 major components of brain...
|
– Cerebral lobes 2
– Cerebellum – Brainstem – Basal ganglia- Striatum, globis palids – Diencephalon – Thalamus and hypothalamus – Limbic system - Emotions |
|
|
ANS is...
|
has 2 systems
– Sympathetic- fight or flight – Parasympathetic- rest and digest Function of ANS- Autonomic Nervous System • Innervation of internal organs, blood vessels, glands • Regulation of smooth muscles (cardiac and organs) • Control of vegetative functions eg: • Influence on muscle tone- Tracts • Respiration, maintaining hemostasis Parasympathetic Nervous System • Activates to maintain homeostasis of body systems • Cell bodies are located in the brain stem and sacral spinal cord – Page 107 • Neurotransmitter is acetylcholine(Ach) |
|
|
SNS is...
|
• SNS---responsible for innervation of skeletal muscles.
– Skeletal nervous system, somatic nervous system is what it is called Sympathetic Nervous System • Activates the fight/flight response – Takes blood flow from GI tract – Constant stress causes cell death • Location of cell bodies is in inter-medio-lateral horn of thoracic and first 2 lumbar section of SC • Neurotransmitters are acetylcholine and norepinephrine |
|
|
Cerebellum has how many lobes? Name them.
|
3
– Anterior – Posterior – Flooculuar |
|
|
Function of Cerebellum
|
• Plays a role in
– Coordination of movement • Gross motor – Walking, crawling, reaching • Fine motor – Writing, shaving, eating, brushing teeth/hair – Maintains of posture – Equilibrium • Balance • Romberg- Close their eyes, stand with feet together, put hands out and test balance – Major function is proprioception • Awareness of ones body in space, unconsciously |
|
|
Top down and Bottom up...What would you do first?
|
Top-Down
• Take a shower and get dressed, then assess their performance. Look at her performance based on an task. • Which one do you use? • Based on diagnoses, their history, or the circumstances (like if they are already in the shower, then go for Top-Down Bottom-up • Perform assessments for range of motion or another sensory testing. Based on that performance, then she will have problems with this and this area. Look at a certain component then generalize. o Zolthan chapter 2 |
|
|
Types of assessments...
|
• Occupation-Based
Specific occupational performance tasks • Static/Quantitative Specific, quantitative measures of performance Getting facts and numbers Static means asking the client to do something with no feedback. Just do it and do the next thing asked • Qualitative Clinical observation See how the client looks. If they have food on their face, if half their hair is combed etc |
|
|
Reliability
|
o Consistency and Accuracy (How close data is to actual results)
Test-Retest Inter-Rater Intra-Rater o Reliability Co-Efficient 1- The best 100% reliable 0.8- acceptable 0.6- Unacceptable o Results are consistent and reliable. Test-retest. Giving the same assessment over time in the same conditions, the results would be the same. Inter-rater 2 different OT’s doing an assessment on a client and getting the same results, regardless of who’s giving it. Intra-rater, The assessors isn’t affect by how many times they give the assessment, even if they gave it 25 people |
|
|
• Validity
|
• How well the test measures what it claims to measure
• Including correlating test results with actual functional abilities • It measures what it is supposed to. The assessment measure sensation, then the assessment actually measures sensation. |
|
|
Standardization of Scoring
|
• Standardization Process
Administer to large sample of specified population to determine how the average person in the population scores Norms are determined Standardized manner Must administer the test the exact way it was supposed to ministered • Non-Standardized Tests Benefits Drawbacks Hasn’t gone through the standardized testing process |
|
|
H and P
|
History and Physical
|
|
|
Client Interview
|
• Past History
• Home Environment • Typical Routine • Available Assistance • Current Status Pain level • Goals and Objectives • Personal Preferences What do you do if client is unable to communicate? – Ask them to write it |
|
|
Observe Functional Performance
|
• Standardized Assessment versus Observation
• Performance versus Interview • Impact of Setting • Note type and amount of cuing client needs Relates to client’s ability to process information Demonstrating, verbal cue, pointing • Record Observations |
|
|
Evaluate Component Skills
|
• Components may include
Sensation Cognitive Perceptual Motor Psychosocial If you are depressed, not motivated, can impact the results • Avoid duplication with other disciplines • Understand impact components have on each other • Record Results |
|
|
Synthesize/Summarize Data SOAP
|
• Subjective- What the client tells you
• Objective- Results of the assessments, not interpreting, just saying what happened • Assessment Problem list- clinical reasoning skills. Figuring out what is wrong • Plan Goals Treatment plan Begin discharge planning immediately |
|
|
Documentation
|
• Legible!
• Professional • Accurate • Complete • Goals Realistic & Obtainable Understandable Measurable Behavioral Able to observe it and see it happen. Seeing the action done |
|
|
CN1 –
|
Olfactory = S
o Function: Smell o Pathway: Chemoreceptors in the nose > inferior frontal lobes > hippocampal formation (temporal lobe) > hypothalamus > thalamus > orbitofrontal cortex o Lesions: Type 1 – Unilateral: no symptoms, opposite olfactory nerve compensates; Type 2 – Bilateral: anosmia (loss of sense of smell) o Test: Test one nerve at a time by first occluding vision, then blocking one nostril. Present one odor at a time to the opposing nostril. Give the patient a list of verbal choices if they have difficulty identifying |
|
|
Cranial Nerve II --
|
o Location:
o Photoreceptors of the retina o Function: o Visual Acuity, the accuracy of sight not the interpretation o Pathway: o Retina optic nerve optic chiasm optic tract lateral geniculate midbrain occipital lobe o Lesion: o Unilateral lesion (only one optic nerve) produces ipsilateral blindness o Bilateral lesion (both optic nerves) produces bilateral blindness o Test: Optic N. =S o Test visual acuity with eye chart, one eye at a time o Visual field test=test vertical and temporal and peripheral vision, test one eye at a time |
|
|
CNIII
|
Oculomotor N. = M.
o Location midbrain at the same level as the superior colliculi o Function Eye movement-specially up, down, medially and laterally o Pathway Medial Longitudinal fasciculus, ordinates in midbrain and innervates the 5 following eye muscles: levator Palplebrae, superior rectus, inferior oblique, inferior rectus, medial rectus o Lesion double vision, eyeball deviates outward or laterally o Test one eye at a time have patient scan moving stimulus while keeping head in fixed position, stimulus is moved in shape of letter ‘H’ to test the muscles; observe symmetry of pupil size to test for strabismus in dim light shine pen light on bridge of nose and observe corneal reflection |
|
|
CN IV
|
Trochlear= Motor Nerve
o Function: Eye movement down/laterally o Location: Just below inferior colliculi o Pathway: Originates at Midbrain, level of colliculi. Ends-superior oblique muscles of the eye o Leision: If damage difficulty looking down/laterally o Test: Test with oculomotor and abducens nere. o Occulomotor nerve test-therapist moving visual stimulus in shape of an H. Allows therapist to determine if eye muscles are working |
|
|
CNV
|
Trigeminal N = S/M
Sensory and Motor information • Sensory o Sensory half of the Trigeminal nerve mediates sensation of the face, head, cornea of the eye, and inner oral cavity. o Includes pain, temperature, and discriminative touch. • Motor o Innervates the jaw muscles that control chewing. 2. Location • Mid pons • Motor o Begins in the pons and goes to the jaw muscles • Sensory o Begins in the inner, oral cavity, sensory receptors in the face, head, and cornea and goes to the pons 3. Lesion o Sensory o Damage to the sensory half causes ipsilateral loss of sensation to the head, face, and inner oral cavity. o Trigeminal neuroglia occurs when half of the face loses sensation o Motor o Weakness in chewing The jaw deviates to the affected side. 4. Test o Sensory Half of the Trigeminal nerve • Evaluate the abilities on the face, head, and inner oral cavity 1. Cotton swab stroke inner oral cavity. Assess intact side then affected. 2. Cotton swab stroke forehead, cheek, jaw, chin. unaffected then involved. 3. Touch patient's cornea with cotton swab to check corneal reflex. |
|
|
CN VI
|
Abducens= M
• Function: lateral eye movement • Pathway: Located in the lower pons, travels to the lateral rectus muscle of the eye • Lesions: Medial Strabismus - Turning inward of the eyeball - Loss of the lateral rectus muscle - Can cause double vision or diplopia Nystagmus • Test: tested simultaneously with Oculomotor and trochlear nerves - test one eye at a time (cover one eye) -keep head still while scanning a moving stimulus (i.e. color pen cap) -therapist moves the stimulus in the shape of an "H" • Observe symmetry and pupil size • Shine pen light into eye and check for constriction of pupil |
|
|
CN VII
|
Facial N.= M and S
A. Sensory • taste receptors • anterior tongue B. Motor • Facial Expressions • Closing eyelids • Muscle for the stapes. 2. The location is mid pons • Starts in the pons and goes to the muscles and sensory portions of the face. 3. Lesion • Decreased taste • Decreased corneal reflex. 4. Test • Test the send of taste on the anterior tongue-Sensory test 1) Present one taste at a time. • sweet • salty • sour 2) Indicate whether they can taste it 3) Identify what it is • Location- Mid to Low Pons • Function- Sensory and Motor • Sensory- taste on anterior tongue • Motor- muscles of facial expression, eye lid closing, stapes of middle ear • Pathway- comes off of a separate branch of the facial nerve called the nervous intermedius • Lesion- decreased taste on anterior tongue and corneal reflex • Test- present sweet, salty and sour solutions to the anterior tongue - ask the patient to elevate eye brows and forehead - ask patient to smile, frown or pucker lips |
|
|
CN VIII
|
Vestibulocochlear S
• Location: Pons-Medulla Junction • Function: Two branches- Auditory, for hearing, and Vestibular for balance and equilibrium. • Pathways: o Auditory- From the hair cells of the organ of Corti to the vestibular nucleus in the brainstem o Vestibular- From the semicircular canals, utricles, and saccules to the vestibular nuclei in the brainstem • Lesion Symptoms: o Auditory- deafness or tinnitus (ringing in ears) o Vestibular- Nystagmus (eyes moving rapidly), vertigo, decreased balance, decreased protective responses, and changes in extensor tone • Tests: o Auditory- Whisper into ears, or rub fingers together next to ears to see if the client can hear the noises. o Vestibular- Romberg Test (Have client stand with open and closed eyes, watch for swaying.) The test for nystagmus would involve the client sitting down and have them follow an object in the shape of the letter ‘H’ or ‘X.’ |
|
|
CN IX
|
Glossopharyngeal S and M
Location: Ambigous in the Medulla near the Vagus N. 2. Function: (S) Taste of posterior aspect of tongue (M) Swallowing 3. Pathway: (Abbreviated version) Medulla to Jugular Foramen to Internal Jugular Vein to inferior to Styloid Process where it passes under the Hyoglossus M. and is distributed to the Palatine Tonsil, Mucous Membrane, base of the tongue, and mucous glands of the mouth 4. Lesion Symptoms: (S) Loss of taste in posterior aspect of tongue (bitter taste) (M) Loss of gag and swallowing reflexes, dysphagia 5. Test: Test with Vagus N. (S) Chew on lemon rind to see if they can taste the bitterness (M) Test gag reflex with tongue depressor |
|
|
CN X
|
Vagus S and M
• Carries - sensory and motor information • Function - Sensory portion carries taste information. Motor portion carries parasympathetic information. • Location - Medulla • Test - Observe the patient's ability to speak clearly without slurring words. Sensory Test |
|
|
CN XI
|
Accessory N= M
) Location • Cranial nerve root o Located in the medulla o Emerges from nucleus ambiguous • Spinal nerve root o Located in C1-C5 o Emerges from ventral horn 2) Function • Cranial nerve root o Elevation of larynx during swallowing • Spinal nerve root o Head rotation, flexion, extension 3) Pathway • Cranial nerve root o Jugular foramen Cranial root Inferior vagal ganglion Striated muscles of soft palate and larynx • Spinal nerve root o Jugular foramen Spinal root Post. To Int. jugular vein Crosses at transverse process of atlas Sternocliedomastoid or Trapezius muscle 4) Lesions • Cranial nerve root o Dysphasia • Spinal nerve root o Weakness in head rotation, flexion, elevating shoulders 5) Test • Cranial nerve root o Place index finger on patient’s Adam’s apple, ask patient to swallow, check rise/fall of larynx • Spinal nerve root o Ask patient to flex head laterally, forward, and rotate head. Ask patient to resist your attempts to prevent desired movement. Compare and check for atrophy |
|
|
CN XII
|
Hypoglossal N = M
• Carries: o Motor information • Pathway: o Originates in the medulla and ends in the muscles of the tongue • Function: o Innervates the muscles of the tongue o Responsible for tongue movement • Lesion Symptom: o Dysphagia (because the tongue muscles are needed to manipulate food into a bolus in the mouth and propel bolus to the pharynx) • Test: o Ask patient to protrude tongue |
|
|
Flexor Withdrawl
|
• Onset: 28 weeks
• Integration: 1-2 months • Testing Position: supine, both legs extended • Stimuli: Sole of foot • Response: Hips, knees and ankle extend and toes extend • Purpose: Safety, survival, walking |
|
|
Flexor Withdrawal-
|
• Onset: 28 weeks
• Integration: 1-2 months • Testing Position: supine, both legs extended • Stimuli: Sole of foot • Response: Hips, knees and ankle extend and toes extend • Purpose: Safety, survival, walking |
|
|
Crossed Extension-
|
• Onset: 28 weeks
• Integration: 1-2 months • Testing Position: supine, one leg flexed, the other extended • Stimuli: flexing the extended leg • Response: opposite leg will extend (the one that is flexed) • Purpose: balance/ Stability |
|
|
Extensor Thrust
|
• Onset: 28 weeks
• Integration: 1-2 months • Testing Position: Supine, one leg extended and one flexed • Stimuli: sole of flexed foot • Response: same leg extends in response • Purpose: withdraw from stimuli |
|
|
Rooting Reaction
|

• Onset: In utero
• Integration: 3 months • Testing Position: Supine • Stimuli: around the lip area from the mouth to the cheek • Response: baby’s face/mouth will turn towards the touch • Purpose: Feeding |
|
|
Moro Reflex (or Startle)-
|

• Onset: Prenatal
• Integration: 5-6 months • Testing Position: supine • Stimuli: hold baby up 20 degrees then drop them (while supporting their head) • Response: hands extend, shoulder adduct • Purpose: Safety, balance |
|
|
Suck-Swallow Reflex-
|
• Onset: prenatal
• Integration: 2-5 months • Testing Position: supine • Stimuli: put pinky in mouth or nipple • Response: sucking movement • Purpose: Feeding |
|
|
Palmar Grasp Reflex-
|

• Onset: birth- 2 months
• Integration: 4-11 months • Testing Position: supine • Stimuli: apply pressure on the palm • Response: grasp/ flex around object • Purpose: work on grasp and grip |
|
|
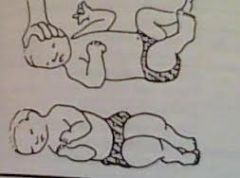
Symmetric Tonic Neck Reflex
|

• Onset: 4-6 months
• Integration: 8-12 months • Testing Position: prone in quadruped position • Stimuli: Flex head/ Extend head • Response: arms flex downwards, legs extend/ arms extend, legs flex • Purpose: crawling, sitting up |
|
|
Symmetrical Tonic Labyrinthine Reflex
|
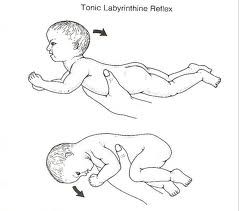
• Onset: Birth
• Integration: 6 months • Testing Position: Supine/Prone • Stimuli: Being in Supine position • Response: legs and arms stay extended and have trouble flexing/ Legs are extended and arms are flexed, hard to extend • Purpose: Helping with rolling |
|
|
Plantar Grasp Reflex
|
• Onset: Prenatal
• Integration: 9 months • Testing Position: Supine • Stimuli: Below the side of the foot • Response: toes curl/flex • Purpose: protection of the foot |
|
|
Babinski Sign
|
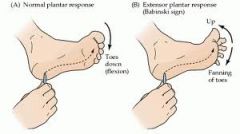
Stroke sole of foot from bottom up, toes should flex, but with Babinski, the big toe extends and toes spread out (extension)
|
|
|
Hoffman’s Sign
|

Flick middle finger nail. Causes flexion of index finger, middle finger will extend
|
|
|
Asymmetrical Tonic Neck Reflex (ATNR)
|
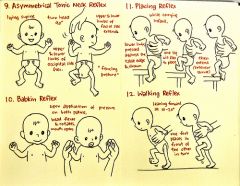
• Onset: Birth
• Integration: 4-6 months • Testing Position: Supine- arms legs extended • Stimuli: turn babies head left • Response: the left hand extends and right arm flexes • Purpose: eye hand coordination |
|
|
Positive Support Reaction
|

• Onset: Birth
• Integration: 6 months • Testing Position: Standing • Stimuli: pressure on ball of foot • Response: extension of foot • Purpose |
|
|
Associated Reaction
|
• Onset: birth- 3 months
• Integration: 8-9 years • Testing Position: sitting • Stimuli: hold a ball in affected hand • Response: other hand will also flex as the effected hand does. Other hand mimics the hand moving • Purpose: using both hands (ex) putting a shirt on) |
|
|
Neck righting on Body-
|
• Onset: 4-6 months
• Integration: 5 yrs • Testing Position: Supine/ arms and legs extended • Stimuli: rotate the head • Response: whole body rotates to align with head • Purpose: rolling, getting into prone position |
|
|
Body Righting on Body
|

• Onset: 4-6 months
• Integration: 5 yrs • Testing Position: supine/arms and legs extended • Stimuli: rotating head or upper or lower trunk • Response: head rotates, then shoulder rotates, then trunk rotates- in segments • Purpose: over all mobility |
|
|
Labyrinthine Head righting response
|

• Onset: birth- 2 years
• Integration: throughout life • Testing Position: vision is covered/ supine/prone • Stimuli: body is tipped over/ tilted body to the left • Response: head tips over with body. Head tilts with the body • Purpose: stability |
|
|
Landau Reflex
|

• Onset: 6 months
• Integration: 2-2 ½ yrs • Testing Position: prone/ carried • Stimuli: head flexion (raise head) • Response: Body flexes- body extends. Head extends (spine legs extend) • Purpose: increases tone |
|
|
Protective Extension (parachute)
|

• Onset: 6-9 months
• Integration: throughout life • Testing Position: standing held up • Stimuli: dropping them • Response: hands extend to protect from falling/ legs abduct • Purpose: protection |
|
|
Equilibrium Reactions (titling)
|

• Onset: 6-21 months
• Integration: throughout life • Testing Position: standing • Stimuli: tilting/ moving the floor • Response: head goes up right, curve body to compensate from falling. Extend extremities, abduction • Purpose: balance, postural control |
|
|
Equilibrium Reactions (Postural Fixation)
|
• Onset: 6-21 months
• Integration: throughout life • Testing Position: standing up • Stimuli: push body • Response: extend and abduct body, curve body to compensate • Purpose: balance, postural control |
|
|
Optic Righting
|
• Onset: birth -2 months
• Integration: throughout life • Testing Position: prone/ supine eyes open • Stimuli: tilt body • Response: bring head to midline • Purpose: stability |