![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
400 Cards in this Set
- Front
- Back
|
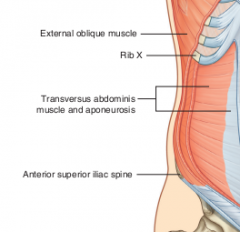
Surface markings Thorax |
Xiphoid process (Rib 6) Costal margin (Rib 6 - Rib 10 laterally) Umbilicus (T6) Linea alba Linea semilunaris |
|
|
Superficial fascia * > locatin > structure |
Location > lower abdomen, anterior below umbilicus Structure > Camper's fascia > Dartos fascia = Men: continuous over penis, having smooth muscle = Women: labia major, fat |
|
|
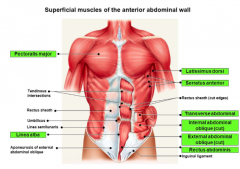
* Intro 1. Most superficial muscle 2. Posterolateral muscles 3. Vertical muscles 4. Form the line alba a. internal oblique b. transversus abdominis c. external oblique d. rectus abdominis e. pyramidalis |
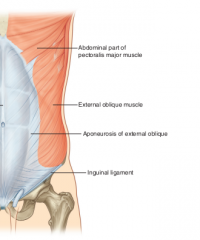
1. External oblique
2. External, internal obliques, transversus abdominis 3. Rectus abdominis, Pyramidalis 4. externat obliques |
|
1. Significance 2. Label *
|
1. What is formed when external oblique is around |
|
|
* 1. Form the inguinal ligament and pectinate ligament 2. Blend with line alba at midline a. internal obliqueb. transversus abdominisc. external obliqued. rectus abdominise. pyramidalis |
1. External oblique 2. Internal oblique, transverses abdominal (the external oblique forms it) |
|
|
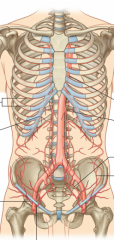
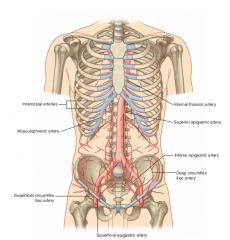
Blood supply abdominal cavity * > Properties |
Superficial > superior: internal thoracic artery = Musuclophrenic A. > inferior: femoral A = Superficial epigastric A. (medial) = Superficial circumflex iliac A. (lateral) Deep > superficial: internal thoracic artery = Superior epigastric A., medial = 10, 11th ICA, subcostal, lateral > external iliac artery = inferior epigastric A. (medial) = deep circumflex iliac artery. The superior epigastric and inferior epigastric both enter rectus sheath, posterior to rectus abdomens muscle throughout their course and anastomose with each other. |
|
|
The superior and inferior epigastric arteries are posterior to what. What else? * |
Posterior rectus abdominis muscle throughout course when they enter rectus sheath. Anastomose with each other |
|
|
Lymphatics abdominal wall* |
Superior lymphatics above umbilicus: axillary nodes Drainage below umbilicus: superficial inguinal nodes Deep lymphatic drainage: parasternal |
|
|
CS 1. 5 Fs for abdominal protrusion: |
fat, feces, fetus, flatus, fluids (+tumors) |
|
|
Surface anatomy of abdominal viscera (CS 2.)* |
G
gallbladder: inserseciton semilunar line, 9th coastal cartilage spleen: under 9th-11th ribs left side, midaxillary kidneys: scapular line, superior lobes at 11th ribs = left more superior than right |
|
|
Gallbladder location * |
intersection semilunar line, 9th costal cartilage referred pain: > referred pain right side, 9th-11th midaxillary |
|
|
spleen location * > referred pain? |
Under 9th-11th ribs left side at midaxillary line referred pain: > 6-7th rib left side midaxillary |
|
|
Kidneys location * > referred pain? |
located along scapular line 11th ribs, left more superior than right, Superior lobes at level 11th ribs referred pain: > back lower left abdominal |
|
|
Relevant dermatomes |
Xiphoid process: T6 Umbilicus: T10 Inguinal ligament; T1 |
|
|
Cremaster reflex * > method > result > significance |
L1-L2 nerve test Method > stroke medial aspect upper thigh, stimulate ilioinguinal nerve Result: contraction cremaster (genital branch genitofemoral nerve), retraction testes |
|
|
A physicina strokes the medial aspect of a person.* 1. Result? 2. Reason? |
1. The cremate should contract (genital branch genitofemoral nerve), resulting in retraction testes. This is the cremaster reflex that is intended to test L1-L2 s/c levels. |
|
|
1. testicular lymphatics 2. scrotal lymphatics 3. deep lymphatic drainage a. para-aortic nodes b.axillary nodes c. parasternal nodes d. superficial inguinal nodes |
1. para-aortic nodes (lumbar) 2. superficial inguinal nodes 3. parasternal nodes |
|
|
Orchitis (CS 16) |
Inflammation testes |
|
|
Peritonitis * (CS 18) > cause > result |
Result: inflammation peritoneum (parietal peritoneum) Cause: > infections, perforated ulcers, appendititis, diverticulitis, cancer, cirrhosis |
|
|
Peritoneal adhesions * (CS 19) > cause > result |
Cause: fusion parietal, visceral alyers, inflammation or trauma (surgery) |
|
|
There is a fusion of parietal and visceral pleura > dx? > cause? * |
Dx: Peritoneal adhesion Cause: trauma (surgery) |
|
|
linea alba * |
band of fibrous C/T, abdominal wall muscles attach to, running from: > xiphoid process - pubis symphysis, between the 2 rectus abdomens muscles |
|
|
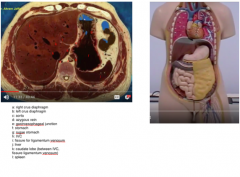
inferior thoracic aperture * > components |
xiphoid process, costal margin, diaphragm |
|
|
diaphragm * |
domed structure w/ organs under: > kidney, spleen |
|
|
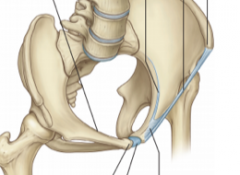
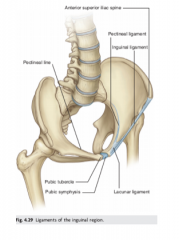
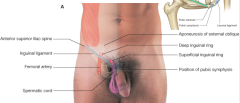
inguinal ligament * > span > structure |
span > between ASIS, pubic tubercle Part of the tendon of the external oblique muscle , bottom edge of ligament rolled on itself |
|
|
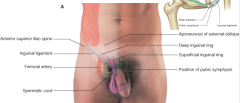
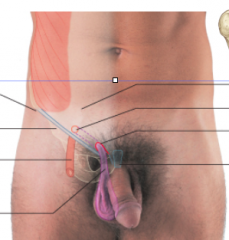
spermatic cord * > components > developmenet |
development > external oblique creates passage way for spermatic cord, part of the reason the abdominal wall forms covering of spermatic cut + scrotum, both testes, ovaries, kidneys, and they move down Structure > inguinalcana, A/V/N |
|
|
Organ locations ** |
Liver: ribs 8, 9, 10 Spleen: lt midaxillary ribs 9-11 Gallbladder: Rt 9th RIB - semilunar line kidney: scapular line, rib 11 (leftkiney more superior right kidney) |
|
|
layers * |
skin, campers fascia, scarpa's fascia, muscles (externa, internal oblqiues, transverses abdominis), transversalis fascia, endoabdominal fascia (extraperitoneal), parietal peritoneum |
|
|
Cremaster muscle * > structure > function |
Structure: > Streaks from internal oblique that extend down into the spermatic cord, cremaster fascia Cremaster reflex: > Irritate thigh, muscle pulls testicle up, cremaster muscle pulled up Sensory part: ilioinguinal Genitlofemoral nerve: inenrvates cremaster muscle Tests: L1 spinal cord level |
|
|
L1 spinal cord injury. 1. What sensory nerve damaged? 2. What muscle nerve damaged? 3. How to test? |
1. ileiinguinal nerve 2. genitofemoral nerve 3. Touch internal thigh |
|
|
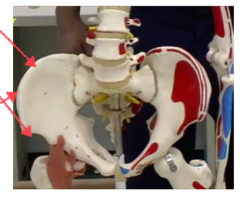
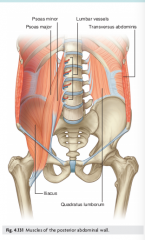
Lateral vertebral abdominal muscles * > label > function |
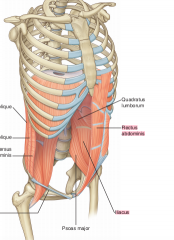
QIP Quadratus lumborus Ileacus muscle Possess major Ileacis + soacis: distal portions pass into thigh and are major flexors of th ship joint |
|
|
Relevant surface markings* |
> Iliac crest (L4) Anterior superior iliac spine (ASIS), L4-L5 Pubic tubercle: one on each sid epubic symphysis Inguinal ligament > between ASIS + pubic tubercle > part of the tendon of the external oblique muscle |
|
|
Spermatic cord * > layers |
External spermatic fascia (external oblique aponeuroses) Cermasteric fascia (internal oblique aponeuroses) Internal spermatic fascia (transversalis fascia) |
|
|
linea alba span * |
xiphoid process - pubic symphysis between 2rectus abdomens muscles |
|
|
Label aspect inguinal ligament * |
|
|
Label * |
|
|
|
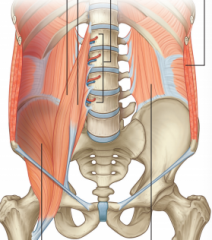
These muscles reinforce posterior aspect of abdominal wall * |
QIP Quadratus lumborus Ileacus Psoas ==> All of these are the lateral vertebral abdominal muscles |
|
|
These muscles pass into thigh and are major flexors of the hip joint ** |
Ileacis Psoasis > Specifically distal ends of posts major and ilacus muscles pass into thigh and are major flexors of th ship joint |
|
|
Rectus abdominis spans * |
inferior thoracic wall - pelvis |
|
|
Define inguinal canal * |
passage via anterior abdominal wall created by processes vaginalis |
|
|
Spermatic cord * |
Tubular extension of layers of abdominal wall into scrotum that contain all structures passing between testis and abdomen > external scrotal fascia(external oblique fascia) > cremaster (internal oblique fascia) > internal scrotal fascia (transversus fascia) |
|
|
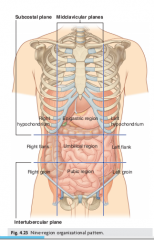
Explan 4 box division abdominal wall * |
2 lines > vertical: umbilicus (T10) - pubic symphysis > horizontal: IVD L3-L4 All have parts SI RUQ: superior ascending colon, poyloris stomach, majority live LUQ: left transverse colon, body stomach, minor part liver RLQ: inferior ascending colon LLQ: |
|
|
9 Divisions abdomen ** |
|
|
|
Divisions fascia abdominal wall * |
Superficial fascia = camper's fascia (superficial fatty layer of superficial fascia) Deep fascia (Scarpa's fascia) = colles' fascia (superficial perineal fascia) = fascia lata (continues into thigh, below inguinal ligament, fusing w/ deep fascia thigh) |
|
|
Explain arterial supply abdomen * |
Superior > internal thoracic = musculophrenic (anterior) = superior epigastric (posterior) Inferior (external iliac artery > femoral artery) > femoral artery > anterior: superficial epigastric artery, superficial circumflex iliac artery > posterior: inferior epigastric artery, lateral deep circumflex iliac arteries Deep lateral: A from 10th, 11TH ICA, Subcostal artery |
|
|
Groin * > span > significance |
span > junction between anterior abdominal wall and thigh significance > weakened from changes that occur during development = can create inguinal hernia, most common in men |
|
|
Inguinal canal * > span > around > contents |
spans > deep inguinal ring - superficial inguinal ring around = deep inguinal ring: midst between Anterior superior iliac spine + Pubic symphysis > parallel to inguinal ligament contents > genital branch genitofemoral nerve > spermatic cord men, round ligament women > ilio-inginal nerve (exiting superficial inguinal ring) |
|
|
deep inguinal ring? * > location > significance |
location > Midpoint Anterior superior iliac spine - pubic symphysis significance > forms one of the covering: interior spermatic fascia |
|
|
SUPERFICIAL INGUINAL RING?* > location > significance |
Location > end inguinal canal, superior pubic tubercle significance > forms external spermatic fascia |
|
|
inenrvation abdominal wall * Dermatomes * |
T7-L2 > T7-T11 T12: subcostal L1: iliohypogastric L2: ilioinguinal ** Dermatomes > T6: Xiphoid process > T10: Umbilicus > L1: Inguinal ligament |
|
|
Functional role of abdominal wall musculature * |
Compress abdominal viscera Assist in respiration Movement |
|
|
Anterolateral abdominal muscles * |
External oblique, internal oblique, transverses abdominal, rectus abdominal, pyramidalis |
|

Label.* |
QIP Top Left: Quadratus lubrosums Middle left: Iliacis RIght: Psoas |
|
|
Label |
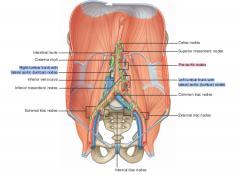
Median umbilical ligament > Supravesical fossa Medial umbilical ligament > Medial inguinal fossa Lateral umbilical ligament > Lateral inguinal fossa |
|
|
Opening in external oblique muscle * |
superficial inguinal ring |
|
|
opening in transversalis fascia * |
deep inguinal ring |
|
|
internal oblique and transversus abdominis * |
Conjoin tendon |
|
|
Superficial inguinal ring * |
opening external oblique muscle |
|
|
Deep inguinal ring * |
opening in transversals fascia |
|
|
Conjoin tendon * |
internal oblique and transversus abdominis |
|
|
cremaster > structure > innervation |
structure > internal oblique innervation > genital branch of genitofemoral nerve |
|
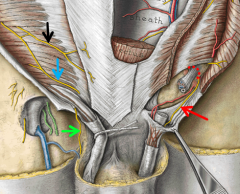
Label * |
Black arrow: Ileohypogastric nerve (L1) Blue arrow: Ileoinguinal nerve (L1) Green arrow: genital branch of genitofemoral nerve > innervates cremaster muscle Red arrow: Deep ring of inguinal canal |
|
|
Label * |
green arrow: deep ring of deep ring inguinal canal blue arrow: genital branch of genitofemoral nerve pink arrow: femoral branch, genitofemoral nerve |
|
|
components hesselbach's triangle * |
lateral border: inferior epigastric artery medial border: rectus abdominis base: inguinal ligament |
|
|
1. What muscle is most proximal to the deep inguinal ring? 2. What muscle is most proximal to the superficial inguinal ring? |
1. transversus abdominis muscle 2. external oblique muscle |
|
|
Properties deep inguinal hernia *** (CS) |
> Transverse anterior abdominal wall > Medial inferior epigastric vessel > pass directly through Hasselbach's triangle = Lateral: inferior epigastric artery = Medial rectus abdominis = Base inguinal ligament > covered parietal peritoneum, transversals fascia > does not transverse entire inguinal canal > outside spermatic cord > emerges from superficial ring > can go into the scrotum |
|
|
Properties indirect inguinal hernia ** |
> Direct inguinal hernias traverse anterior abdominal indirectly, through inguinal canal > most common type inguinal hernia > leave abdominal cavity lateral epigastric vessels via congenitally patent deep ring > traversese entire inguinal canal > same coverings of spermatic cord > common enter scrotum |
|
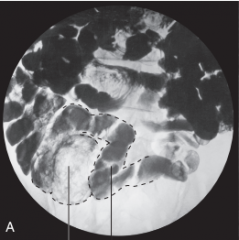
Type hernia? * |
Indirect b/c inside, in inguinal canal |
|
Type hernia?* |
Indirect b/c inside inguinal canal |
|
|
Hernias and comparisons |
Direct inguinal hernia: medial inferior epigastric A indirect inguinal hernia: lateral inferior epigastric A Femoral hernia: inferior inguinal ligament |
|

Describe * |
Femoral hernia > inferior inguinal ligament |
|
|
Explain arterial flow, venous drainage of testes |
Arteries > from abdominal aorta Venous > right testicular veins: IVC > left testicular veins: left renal vein |
|
|
Dx * Possibilities? |
Direct henia * (most common since older male) Hematocele |
|
|
Dx* |
Hematocele > if intestine must be clear fluid (peritoneal fluid) Cause: > deep inguinal ring that doe snot close, from that cavity leaking fluid into scrotum |
|
|
1. What layers must be cut? 2. Structure in danger of iatrogenic injury? 3. Nods lymphadenoapthy? |
1. Skin, Campers fascia, Sarcos fascia, External spermatic fascia, cremaster, internal spermatic fascia 2. Testicular artery, ilioinguinal artery, genital branch: genitofemoral nerve 3. Superficial inguinal node (since scrotum) |
|
Label * |
|
|

1. Organ 2. Label * |
Gallbladder Neck Body Fundus |
|
|
Areas around stomach if ulcer develop * |

|
|
|
Anterior stomach * |
left: hepatic right: phrenic lower: epigastric |
|
|
Posterior stomach * |
Splenic Renal, Adrenal Pancreatic Colomesocolic surface Hepatic surface (bottom right) |
|
|
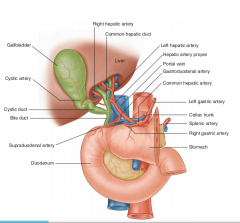
Lesser omentum * > span > components |
Span > lesser curvature stomach - 1st part duodenum - inferior surface liver Components > medial hepatogastric ligament > lateral hepatoduodenal ligament = end laterally as free margin,s erving as anterior border of mental foramen > enclosed in free edge, hepatic artery proper, bile duct portal vein, right and left gastric vessel between layer lesser momentum near lesser curvature stomach = haas portal triad = artery, vein, bilary systme (bile duct) |
|
|
Divisions abdominal * > blood supply |
Divisions: Foregut, Midgut, Hindgut Foregut > Inferior esophagus, stomach, liver, spleen, proximal duodenum = Blood supply: Celiac artery, division abdominal aorta Midgut > Distal 2/3 duodenum, Jejunum, Ileum, Ascending, transverse colons, appendix = Blood supply: Superior mesenteric artery, division abdominal aorta Foregut > Descending colon, Sigmoid colon, rectum = Blood supply: Inferior mesenteric artery, division, abdominal aorta |
|
|
Lowest part external oblique aponeuroses ? * |
Inguinal ligament |
|
|
1. Inguinal ligament composed of what?* 2. Location related to what structure?* a. internal oblique muscle b. internal oblique aponeuroses c. external oblique muscle d. external oblique aponeuroses e. transversus abdominis muscle f. transversus abdominis fascia g. rectus abdominis muscle h. pyramidalis muscle |
1. external oblique aponeuroses 2. The lowest part of the external oblique aponeuroses is the inguinal ligament. |
|
Label * |
Anterior superior iliac spine (distal part of the inguinal ligament) |
|
Label * |
Pubic symphysis * (medial part of inguinal ligament) |
|
Label * |
inguinal ligament |
|

Describe * |
Fascia lata (deep fascia(Scarpos fascia)) of the thigh
|
|
|
Layer surrounding rectus muscles* > layer > rectus muscles? |
Rectus muscles: > rectus abdominis, pyramidalis The rectus sheath encloses rectus muscles Formaiton rectus sheath (via fascia of flat muscles) > aponeuroses of external oblique muscles, internal oblique muscles, transversals muscles |
|
|
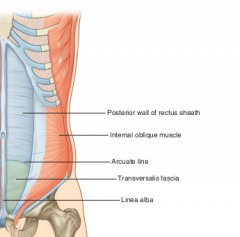
Arcuate line * |
Line demarcates transition between aponeurotic posterior wall rectus sheath and transversals fascia |
|
|
linea alba * > span > structure |
span > XP - Pubic symphysis structure > anterior + posterior layers of the rectus sheath = Rectus sheath: anterior layer: aponeuroses of all 3 muscle layers |
|
|
What cover the inferior epigastric vessels? * a. median umbilical ligament b. medial umbilical ligament c. lateral umbilical ligament |
lateral umbilical ligament |
|
|
Explain GI venous drainage * |
SMV + Splenic vein (POSTERIOR NECK PANCREAS) > Hepatic portal vein > sinusoids liver > IVC |
|
|
Where does SMV + Splenic vein meet?* |
Posterior neck pancreas |
|
|
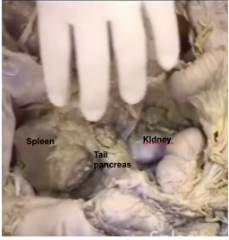
At the hilum of the spleen * |
Tail pancreas |
|
|
Tail pancreas near what * |
Hilum spleen Superior part kidney |
|
|
Nerves to kidney * |
T12, L1 Subcostal nerve Iliohypogastric nerve Ilioinguinal nerve |
|

Describe * |
|
|
|
Ureter passes anterior to what muscle * |
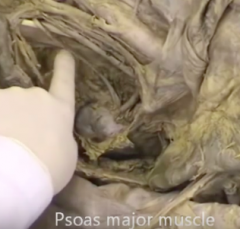
Psoas major |
|
|
Structure around psoas major muscle |
Anterior: > ureter > genitofemoral nerve |
|
|
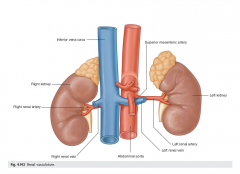
Possible sites ureter constriction * |
1. Bifurcation of common iliac artery into external and internal iliac arteries (see diagram drawn) 2. Pelvo-uretetic junction (see diagram drawn) 3. Entrance to bladder |
|
|
Gallbladder relations * |
Fundus gallbladder at level pylorus stomach |
|
Label * Importance ? * |
Top to bottom: Iliac crest, Tubercle of iliac crest, Anterior superior iliac spine (ASIS) Iliac crest: L4 ASIS: first part of inguinal ligament Tubercle of iliac crest (L5): Forms the inter tubercular plane (lower horizontal plane of the 9 box designation) |
|

Describe * |
ASIS (Below Tubercle iliac crest, L5) |
|

Describe * |
tubercle of iliac crest (location transtubercular plane) L5 vertebra |
|
Label * |
|
|
Label * |

|
|
* |
Horseshoe kidney |
|
|
Common sites ureteral constrictions * |
constrictions, stones > renal pelvis > crossing over by genital vessels (testicular, ovarian) |
|
|
Rectus sheath * |
Formed by aponeuroses of 3 Flat muscles |
|
|
1. What covers the inferior epigastric vessels? ** 2. What covers umbilical vessels?** 3. What contains deep inguinal ring?** a. median ubilical ligament b. medial umbilical ligament c. lateral umbilical ligament d. transverse umbilical ligament e. supravesical fossa f. medial inguinal fossa g. lateral inguinal fossa |
1. medial umbilical ligament 2. lateral umbilical ligament 3. lateral inguinal fossa |
|
|
Quadratus lumborus * @ > span > function |
Span > 12 rib - TP 1st 3 Lumbar vertebrae, inserted iliac crest, TP L5 Function > lateral flexion lumbar spine |
|
|
Psoas major > span > function |
Span > TP, VB, IVD T12-L5 Function > |
|
|
rECTUS ABDOMINIS * > Span |
Span > 5,6,7 costal cartilages - pubic crest |
|
|
External oblique* > Span |
Span: > Rib 5 - Rib 12 |
|
|
Internal oblique * > span |
Span > thoracolumbar + iliac crest + superior inguinal ligament - upwards |
|
|
1. What supplies the jejunum most directly? 2. What supplies the ileum most directly? a. celiac trunk b. superior mesenteric artery c. inferior mesenteric artery d. superficial epigastric artery e. superior epigastric artery f. deep circumflex artery |
1. superior mesenteric artery
2. SMA (ileal arteries, ileac branch ileocolic artery) |
|
|
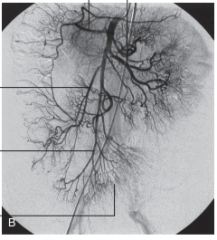
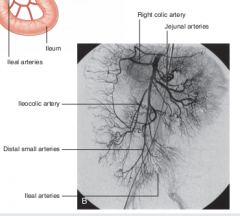
SMA, IMA supply * |
SMA: > Jejuneal arteries > Ileal arteries > Ileocolic artery = Ileal branch = Cecal artery (to colon) > right colic A (to ascending colon) > middle colic A (to transverse colon) IMA: > left colic A (to descending colon) > sigmoidal A > superior rectal A |
|
|
What supplies the rectum *? |
Superior rectal A (from inferior mesenteric A) |
|
|
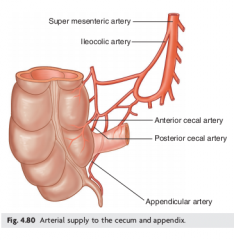
Blood supply to 1. Colon 2. Appendix * |
1. Colic artery of ileocolic artery (of SMA) 2. Appendicular artery of ileocolic A (of SMA) |
|
|
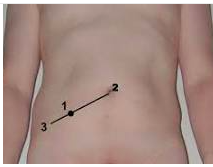
Pain abdomen. Where felt? * |
McBurney's point Lateral and middle 1/3 of line from ASIS to umbilicus |
|
Label * |
|
|
|
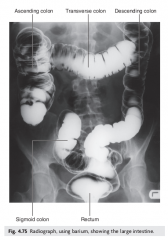
Parts colon peritoneal/retroperitoneal ? * |
Ascending, descending colon > (secondarily) retroperitoneal Transverse, sigmoid colon > intraperitoneal |
|
|
location right colic flexure * |
junction ascending and transverse colon (inferior to the right lobe of the liver) |
|
|
location left colic flexure * |
junction transverse, descending colon (inferior spleen) Higher and more posterior to right colic, attached to diaphragm by phrenjicocolic ligament |
|
|
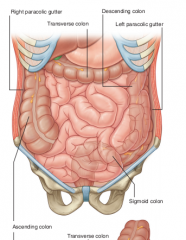
right and left parabolic gutters * > location > significance |
Formation/loocation > depressions are formed between the lateral margins of the ascending and descending colon and the posterolateral abdominal wall Significance > Materials can pass from 1 region of the peritoneal cavity to another |
|
|
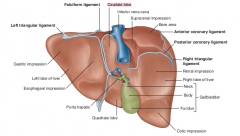
surfaces liver * |
diaphragmatic surface: anterior, psoterior, superior visceral surface: inferior direction |
|
|
recesseces liver * |
diaphragmatic recesses > subphrenic: separates diaphragmmatic surface liver from diaphragm, divided by falciform ligament > hepatorenal recess: part peritoneal cavity on right side between liver and right kidney and right suprarenal gland |
|
|
subphrenic recess * |
separated diaphragmatic surfaece of the liver from he diaphragm divided into right and left areas by the falciform ligament |
|
|
hepatorenal recess * |
part of peritoneal cavity on right side between liver and right kidney and right suprarenal gland |
|
|
areas visceral surface liver not covered with visceral peritoneum?* |
fossa gallbladder porta hepatitis bare area liver (small area liver against diaphragm) |
|
|
connects between liver * |
additional folds peritoneum connect liver to: > stomach (hepatogastric ligament) > duodenum (hepatoduodenal ligament) > diaphragm (right and left triangular ligaments and anterior and posterior coronary ligaments) = triangular ligaments are when coronary ligaments come together laterally |
|
|
lobes of the liver * |
left and right lobe divided via falciform ligament (anteriorly and posteriorly) caudate lobe > between fissure for ligamentum venosum (left) + IVC (right) > functionally separated from both lobes liver (right and liver) quadrate lobe > between fissure for ligamentum teres (left) and gallbladder fossa (right) > functionally related to the left lobe liver |
|
|
arterial supply liver * |
right and left hepatic artery propers (from common hepatic artery, from celiac branch abdominal aorta) |
|
|
Diagram visceral portion liver * |
|
|
|
Blood supply gallbladder * |
Cystic A(from right hepatic artery, from hepatic A proper, from common hepatic artery, from celiac trunk of abdominal aorta) |
|
|
** 1. Rounded end part of an organ that may project from the inferior border of the liver 2. Narrow part of this organ with mucosal folds forming the spiral fold 3. May be against the transverse colon and superior part of the duodenum a. fundus b. body c. pylorus d. neck e. cardia |
1. fundus (of gallbladder) 2. neck (of gallbladder) 3. body (of gallbladder) |
|
|
pancreas * (see drawn diagram too ) > orientation > R/P? |
Orientation: > lies mostly posterior to stomach extends across the posterior abdominal wall from the duodenum on the right and spleen on the left R/P > (secondarily) retroperitoneal |
|
Label ** |

|
|
|
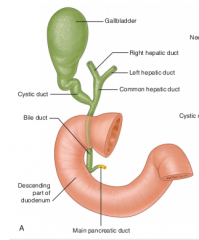
Explain ducts within the pancreas * |
ducts: pancreatic duct in tail pancreas > enters pancreas goes inferior > joining bile duct to form > hepatopancreatic ampulla (ampulla of Vater) > enters descending part duodenum at major duodenal papilla (surrounding ampulla is sphincter of ampulla, smooth muscle)Accessory pancreatic duct> empties into duodenum above major duodenal paipilla at minor duodenal papilla |
|
|
Blood supply to pancreas * |
gastroduodenal A from common hepatic artery (brac of celiac trunk), after branching forms hepatic artery proper |
|
|
Pancreatic cancer * > sx > patho |
sx: > non specific sx: = upper abdominal pain, loss appetite, weight loss = obstructive jaundice (obstruction of bile duct) Patho > most frequent within head and neck |
|
|
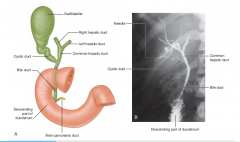
Describe duct system for bile * |
|
|

Label * |
|
|
|
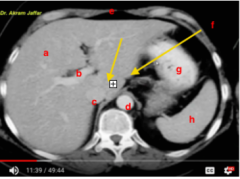
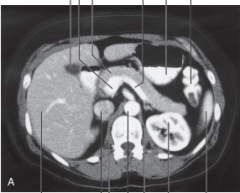
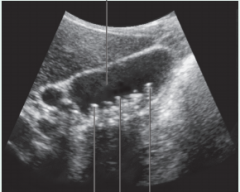
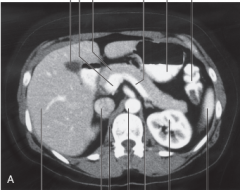
Spleen location * transverse section shown |
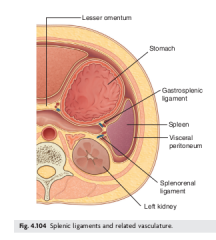
LUQ (Left hypochondrium) midclavicular 9th rib left of pancreas (see diagram drawn) posterior stomach (connected via gastrosplenic ligament) anterior left kidney (connected via splenorenal ligament) |
|
|
Hartmann's pouch * |
bulbous region neck on gall bladder gallstones impact the region of Hartmann’spouch, which is a bulbous region of the neck of the gallbladder causing severe pain |
|
|
cholecystitis * > sx > patho |
sx > pain RUQ (Right hypochondriac), right shoulder patho > if inflammation involves parietal peritoneum, pain may not only be RUQ but also right shoulder b/c referred pain due to innervation o visceral peritoneum of diaphragm by spinal cord levels: C3-C5 that also innervate skin of the right shoulder Thus one somatic sensory region of low sensory output (diaphragm) related to another somatic sensory region of high sensory output (dermatomes) |
|
Label, explain * |
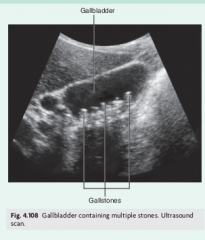
Multiple gall stones in gall bladder |
|
|
Splenic rupture * > cause > result |
Cause > left lower rib fractures > blunt abdominal injury > localized trauma to LUQ Result: > profuse bleeding into peritoneal cavity b/c spleen highly vasucular explanation: Because the spleen has such a extremely thin capsule, susceptible to injury even when there is no damage to surrounding structures and evacuees the spleen is highly vascular when ruptured, spleens profusely into peritoneal cavity |
|
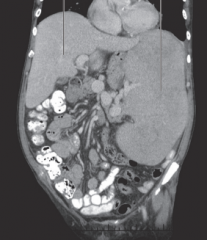
Explain * |
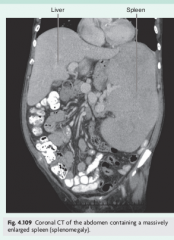
Splenomegaly (enlargement spleen) |
|
Describe * |

|
|
|
The blood supply to the gallbladder. Is derived directly from what proximately? * a. common hepatic artery b. hepatic artery proper c. left hepatic artery d. right hepatic artery e. gastroduodenal artery f. splenic artery g. celiac artery h. SMA i. IMA j. abdominal aorta |
right hepatic artery |
|
|
Porta hepatis significance * |
hepatic artery proper divides into left and right hepatic arteries near the port hepatis |
|
|
hepatic artery proper divides into left and right hepatic arteries near where? * |
porta hepatis |
|
Label, describe * |
|
|
|
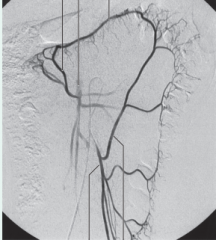
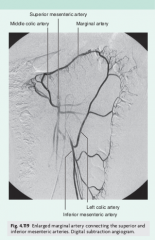
Middle colic artery * > supply > Mech |
Supply > supplies transverse colon Mech > enters transverse mesocolon dividing into right and left branches = right branch anastomoses w/ right colic A, = left branch middle colic artery anastomoses with left colic artery (branch Inferior mesenteric artery) |
|

Label * |

|
|
Label * |
|
|
Label* |
|
|
|
IVC * > tributaries |
> 2 common iliac veins > lumbar veins = become important collateral channels between lower and upper parts of body if IVC become blocked = types lumbar veins - 1st, 2nd lumbar veins: empty into ascending lumbar veins - 3rd, 4th lumbar veins: drain into IVC - 5th lumbar vein: drains into iliolumbar vein, tributary of common iliac vein > right (genital) testicular or ovarian vein > right renal vein > right suprarenal vein > inferior phrenic vein > hepatic veins |
|
|
Lymphatics within posterior abdominal wall ** |
Types: pre aortic nodes: anterior abdominal wall para-aortic nodes = types: right and left lateral aortic or lumbar nodes |
|
Label and explain * |
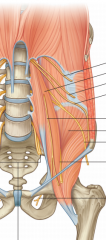
This shows the lumbar plexus, L1-L3, Most L4, Parts T12 Anterior psoas major: > L2 Genitofemoral nerve Lateral psoas major (from superior to inferior): > subcostal nerve, T12 > L1, iliohypogastric nerve > L1, ilioinguinal nerve > lateral cutaneous nerve of thigh, L2-L3 > femoral nerve, L2-L4 Medial to psoas major: Obturator nerve, L4 |
|

Label relevant nerves ** |
|
|

Label and describe orientation and function * |
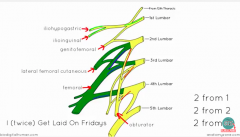
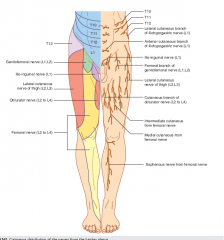
L1 superior: iliohypogastric N > pubic region L1 superior: ilio-inguinal N > penis in males, labia majus in females L1-L2: Genitofemoral N > genito branch: cremaster males > femoral branch: anterior portion thigh L2-L3: Lateral cutaneous nerve of the femur > lateral portion thigh L2-L4 lateral: femoral N > anterior portion thigh to leg L2-L4 medial: obturator N > medial portion thigh |
|
|
5 Fs for ?. CS 1. ** |
5 Fs for abdominal distentions: > fat > flatus > fluid > feces > fetus |
|
|
Locations organs. CS 2. ** |
Gallbladder > Between semilunar line and 9th costal cartilage Spleen > Midaxillary line between 9-11th ribs Kidney > Scapular line, superior poles 11th rib > right kidney lower than left kidney due to presence liver |
|
|
Dermatomes ** CS 3. |
Xiphoid process: T6 Umbilicus: T10 Inguinal ligament: L1 |
|
|
Ilioinguinal nerve * > level > location > innervation > testing |
level > L1 of lumbar plexus location > lateral posts major muscle innervation > penis, labia majora testing (L1-L2 testing) > stroke medial upper thigh to stimulate ilioinguinal nerve (Cremaster reflex, cutaneous abdominal reflex) > should result in contraction of cremaster muscle via genital branch of genitofemoral nerve (L1-L2) and cause testes retraction |
|
|
inguinal hernias ** (CS 8) Comparison direct, indirect |
Direct/indirect inguinal hernia: > most common older males w/ weak abdominal muscles, rare females, children / children (99%), females (70%), males (50%) > herniating bowel exits abdominal cavity medial inferior epigastric vessels via Hesselbach's traingle (bound rectus abd laterally, base inguinal ligament, inferior epigastric vessel medially) / leaves abdominal cavity lateral inferior epigastric vessel via deep inguinal ring > covered by parietal peritoneum + transversals fascia, external spermatic fascia / same covers as spermatic cord (internal spermatic fascia, cremaster, external spermatic fascia) > does not traverse entire inguinal canal, leaving superficial inguinal ring / traverses entire inguinal canal, deep inguinal ring - superficial inguinal ring > nothing said about entering scrotum / commonly enters scrotum > both difficult to diagnose via assessment > direct hernias diagnosed 75%~ intraoperatively |
|
|
Amyand hernia * (CS 8) |
Inguinal hernia involving the appendix Sx > McBurney point pain (1/3 between ASIS, Umbilicus), location where appendix commonly attached to cecum |
|
|
Torsion of the testes ** (CS 11) |
Torsion of the testes Factors Infants < 1 year Cause/Patho Rotation/twisting of spermatic cord Deficient anchoring testicle to tunica vaginalis via gubernaculum > free rotation of testicle in the scrotum Result Sudden testicular enlargement and pain N&V Abnormal cremaster reflex (L1-L2 damaged?) Abnormal positioning of the epididymis , Head of epididymis to testicle instead of nromally, posterior + lateral |
|
|
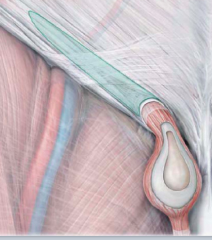
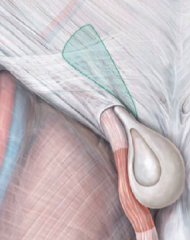
Layers from testes to scrotum * diagram shown |
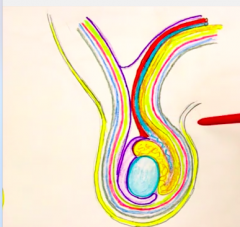
> tunica albuginia (inside testes), blue > tunica vaginalis, purple > processes vaginalis (continuation TV above), purple up > internal spermatic fascia (trasnversalis fascia), yellow > cremaster (internal oblique aponeuroses) ck, next layer > external spermatic fascia (external oblique aponeuroses) , next layer > dartos fascia (deep layer campers/fatty/superficial fascia) > skin |
|
|
* 1. Patient complains of nausea and vomiting and epididymis was assessed to be posterolateral to the testis. What is the most likely diagnosis? * 2. Other physical findings? 3. Cause? |
1. Not torsion of testis, b/cepididyis is normal, anterolateral 2 None |
|
|
* 1. Patient complains of nausea and vomiting and epididymis was assessed to be anterior to the testis. What is the most likely diagnosis? 2. Other physical findings? 3. Cause? |
1. Torsion of the testis, since epid. is anterior abnormally when it should be psoterolateral 2. Absent cremaster reflex (no scrotal retraction)(innervated by genital branch genitofemoral nerve, L1-L2 of lumbar plexus) Sudden testicular enlargement and pain N&V Abnormal epididymis position, anterior instead of normal psoterolateral 3. Deficient anchoring of testicle to tunica vaginalis via gubernaculum resulting in free rotation of testicle ins crotum, also rotation/twisting of spermatic cord |
|
|
Hydrocele * |
patho > accumulation fluid in the tunica vaginalis cause > can be congenital = communication between tunica vaginalis and processes vaginalis Dx > transillumination of the scrotum |
|
|
Hematocele * |
Patho > accumulation of blood in the tunica Vaginalis Cause > Trauma |
|
|
** 1. Absent cremaster reflex 2. Enlarged scrotum after trauma in scrotal area 3. Communication between processes vaginalis and another area after birth 4. Area where fluid accumulates in the scrotum commonly |
1. torsion testes 2. hematocele 3. hydrocele 4. tunica vaginalis (after tunica albuginea) |
|
|
** 1. Sudden testicular enlargement and pain, N&V |
1. Torsion of testes, |
|
|
Explain lymphatic drainage testis and scrotum ** |
Testis: lumbar (para aortic nodes) scrotum: superficial inguinal node |
|

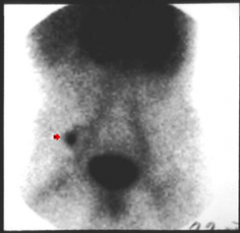
This was noted on a patient. ** 1. Dx 2. Cause 3. Patho 4. Sx |
1. Varicocele 2. Varicose vein of the pampiniform plexus due to vertical entry of left testicular vein into left renal vein (congestion) and or entrapment of left renal vein by SMA. (more commonly on the left side) 4. Hematuria, flank pain, varicocele |
|
|
This was observed ** 1. Dx 2. What vessel can affecting the left testicular vein? 3. What vessel can be affecting the left renal vein? 4. Sx expected? |
1. Varicoceles 2. Left renal vein 3. SMA 4. Flank pain, hematuria, varicocele |
|
|
Vesectomy * > anesthesize? > layers traversed > NV structures at risk |
Anesthesize: > Iliohypogastric, ilioinguinal (L1) neves > genitobranch genitofemoral nerve (L1-L2) Layers traversed: > Skin, Colles fascia, dartos fascia, External spermatic fascia, cramaster muscle/fascia, internal spermatic fascia, extraperitoneal fat NV structures at risk > inferior epigastric artery, external iliac artery, external iliac vein |
|
|
Phrenicolic ligament** (CS 17) |
Phrenicolic ligament: > tethers the splenic flexure of the colon to the body wall, restricting the flow of ascites in the abdominal cavity |
|
|
Guarding ** (CS 20) |
Pain from appendicitis, ulcers, tumor or ectopic pregnancy resulting in guarding Flexive contraction of abdominal wall musculature to protect inflamed organs |
|
|
** Pain from appendicitis, ulcers, tumor or ectopic pregnancy resulting in guardingFlexive contraction of abdominal wall musculature to protect inflamed organs |
Guarding (CS 20) |
|
|
Mesentery * (CS 21) > area > properties > patho |
Area > Peritoneal folds that attach viscera to posterior abdominal wall Proeprties > allow movement (CS) and provide a conduit for vessels, nerve, and lymphatics Patho > although allow movement, prone to volvulus, twisting of the organ that block flow of intestinal contents (obstruction) ,resulting in reduced blood flow and ischemia |
|
|
Volvulus * (CS 21) > Description > Organs |
Description > twisting of the organ that block flow of intestinal contents (obstruction) ,resulting in reduced blood flow and ischemia Organ > commonly those in mesenteries (SI) |
|
|
Ascites * > description > tx |
Description > accumulation sserous fluid within peritoneum Tx > Paracentesis |
|
|
Peritoneum ** > clinical uses > pathos |
Clinical uses > paracentesis > intraperitoneal delivery of drugs (peritoneum large S/A), permitting rapid absorption fluids within peritoneal cavity > peritoneal dialysis: used in renal failure, large surface area of peritoneum allows ut to be used as a dialysis membrane > ventriculoperitoneal shunt: through proper placement of catheter, excessive CSF can be absorbed via peritoneum > pneumoperioteum: gas can be introduced into peritoneal cavity for laparoscopic procedures |
|
|
pneumoperitoneum (CS 27)** |
pneumoperiotneum: gas can be introduced into peritoneal cavity for laparoscopic procedures |
|
|
Ventriculoperitoneal shunt ** (CS 26) |
ventriculoperitoneal shunt: through proper placement of catheter, excessive CSF can be absorbed via peritoneum |
|
|
Tx renal failure ?* |
Peritoneal dialysis. used in renal failure, large surface area of peritoneum allows ut to be used as a dialysis membrane |
|
|
Peritoneal dialysis ** (CS 25) |
peritoneal dialysis: used in renal failure, large surface area of peritoneum allows ut to be used as a dialysis membrane |
|
|
Intraperitoneal delivery of drugs ** (CS 24) |
intraperitoneal delivery of drugs (peritoneum large S/A), permitting rapid absorption fluids within peritoneal cavity |
|
|
GERD (CS 28)** > cause > sx > protection against |
Sensation of esophagus > via vagus nerve Sx > heartburn (pyrosis), dysphagia and or sore throat Protection against > LES > folds of gastric mucosa folding seal > angle of the cardiac orifice > diaphragm - right crus |
|
|
Barrett's esophagus * |
Patho: Barrett’s esophagus Cause:Chronic reflex Patho: > Replacement of the esophageal epithelium w/ gastric epithelium from chronic reflex Consid: > Patietnts w/ BE have significantly increased risk of developing esophageal carcinoma. |
|
|
** 1. Pyrosis, dysphagia or sore throat 2. Significantly increased risk of developing esophageal carcinoma |
1. GERD 2. Barretts esophagus |
|
|
Long standing Pyrosis, dysphagia or sore throat result? ** |
Barretts esophagus > significantly increased risk esophageal cancer |
|
|
Gastric ulcer * |
Patho > Erosion of stomach lining, eroding via walls + damage adjacent structures > Erosion of major artery can result in significant blood loss + death Result Tx > Surgical sectioning of branch from vagal trunks |
|
|
Tx gastric ulcer * |
surgical sectioning of branch from vagal trunks |
|
|
* 1. Stomach venous channels can spread cancers to where? 2. Stomach cancer via supraclavicular nodes can spread to where? |
1. liver 2. duodenum, pancreas |
|
|
Gastric cancer * > metastasis routes |
Spread locally to impact the duodenum, pancreas, posterior body walls Mech: > via lymph channels: celiac nods = supraclavicular nodes (Virchow's node) = periumbilical nodes (sister mary joseph nodule, ovarian cancer also) > via venous chanenls: To liver f = anterior axillary node (irish node) |
|
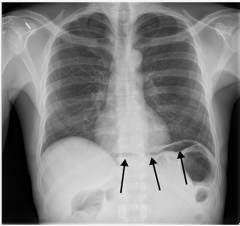
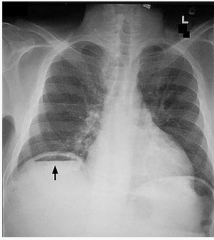
Explain ** (CS 33) |
Sx: intraperitoneal air Dx: Some sort of perforation Expl: Any perforation (i.e: ulcer) involvign stomach, sI, LI can result in intraperitoneal air which can be identified o the radiography as 'free sub diaphragmatic air' |
|
** |
Sx: intraperitoneal air Dx: Some sort of perforation Expl: Any perforation (i.e: ulcer) involvign stomach, sI, LI can result in intraperitoneal air which can be identified o the radiography as 'free sub diaphragmatic air' |
|

Explain *** |
(Wilkie's) Superior mesenteric artery syndrome > Common in young anorexic women w/ little intraabdominal fat Patho > Compression of the 3rd part of the duodenum between SMA and Abdominal aorta Sx: N&V, abdominal pain, malnutrition |
|
|
Wilkie's syndrome ** (CS 34) |
(Wilkie's) Superior mesenteric artery syndrome > Common in young anorexic women w/ little intraabdominal fat Patho > Compression of the 3rd or 4th parts duodenum between SMA and Abdominal aorta Sx: N&V, abdominal pain, malnutrition |
|
|
A 15-year-old female patient was urgently admitted with symptoms of dehydration, loss of appetite and persistent vomiting for 10 weeks. For four months she was vomiting two to three times weekly and this increased to three to four times daily during the last week before admission. Dx most likely? * a. gastric carcinoma b. stomach ulcer c. Wilkie's syndrome d. Transecting abdominal aneurysm e. myocardial infarction f. Barrett's esophagus |
Wilkie's syndrome |
|
|
** CS A 35-year-old female presents to your clinic withcomplaints of onset of severe mid-epigastric pain andvomiting following meals. Between meals she is asymptomatic.This has been going on for the past 2 yearsever since she purposefully lost 25 pounds to attain ahealthy weight for her height. Unfortunately, she hascontinued to lose weight because of the postprandialpain and vomiting. On her exam you notice a midepigastricbruit.The most likely diagnosis is: A) Aortic aneurysm. B) Atherosclerotic disease of the celiac trunk. C) Superior mesenteric artery syndrome. D) Chronic pancreatitis. |
C) Superior mesenteric artery syndrome. |
|
|
Ileal diverticulum (Meckel's diverticulum) ** |
Patho > About 2 feet from the ileocecal valve there exists in 2 % of the population an ideal diverticulum (Meckel’s diverticulum), representing a persistent vitelline duct. Rules of 2 > 2% population, 2 feet proximal ileocecal valve, 2 inches length, 2 types of common ectopic tissue (gastric and pancreatic), 2 years most common age at clinical presentation, 2:1 male : female ratio Sx > Majority people asymptomatic (silent Mecke’s diverticulum) > Painless rectal bleeding: melena like black offensive stools > followed by intestinal obstructionfeatures acute appendicitis > Pain epigastric, umbilical regions |
|
|
A 2-year-old boy with no significant past medical history presents with bright red blood per rectum in his diaper. His parents were immediately concerned and called the pediatrician. The patient is not in much pain but cries when the RLQ is palpated. Dx? ** CS |
Meckel's diverticulum (ileal diverticulum) About 2 feet from the ileocecal valve there exists in 2 % of the population an ideal diverticulum (Meckel’s diverticulum), representing a persistent vitelline duct. |
|
Dx *? CS ** |
Meckel's diverticulum (ileal diverticulum) About 2 feet from the ileocecal valve there exists in 2 % of the population an ideal diverticulum (Meckel’s diverticulum), representing a persistent vitelline duct. |
|
|
Crohn's disease ** |
Description > Chronic inflammatory condiiton of the intestine (most one the ileum) that typically leads to fibrosis and obstructive symptoms Sx > Abdominal pain, diarrhea, Often complicated by fistulas and obstructions |
|
|
Ischemia of the intestine *** |
Ischemia of the intestine > Despite good collateral circulation, a blood clot may deprive a small segment of intestine, resulting in encores Sx > Visceral painIleus (blockage because of paralysis) |
|
|
*** 1. Visceral pain, ileus 2. n&v 15 year old anorexic female 3. About 2 feet from the ileocecal valve there exists in 2 % of the population 4. abdominal pain, diarrhea, often complicated by fistulas and obstructions 5. Intraperitoneal air on CT 6. significantly increased risk esophageal cancer a. IBD b. crohn's disease c. ischemia of the intestine d. Transition normal stratified squamous epithelium to columnar epithelium e. perforated duodenal ulcer f. Meckel's diverticulum g. Wilkie's syndrome |
1. ischemia of the intestine 2. wilkie's syndrome (or SMA syndrome) 3. Meckel's diverticulum 4. crohn's disease 5. perforated duodenal ulcer 6. significantly increased risk esophageal cancer (Barrett's esophagus) |
|
|
Appendix *** > Clinical supplement facts |
Predisposition to appendix to infection > reason: since the appendix is a long thin tube, it can easily collect fecal material As a result, the thin long tube can get blocked with fecal material and be infected Structure > significant lymphoid tissue Appendicular artery > does not form significant anastomoses, thus inflammation of appendix can compress surrounding appendicular artery leading to neroiss/gangrene/perforation Appendicitis (most common cause acute abdomen) > pain begins as vague 'visceral' (GVA) around the umbilicus (referred pain*) > then irritation of the parietal peritoneum results in a well-localized, somatic pain (GSA), right lower quadrant or right flank region = pain GSA commonly located at McBurney's point: 1/3 between ASIS and the umbilicus, used to approximate the appendix region) |
|
|
Appendicitis ** |
Appendicitis (most common cause acute abdomen) > pain begins as vague 'visceral' (GVA) around the umbilicus (referred pain*) > then irritation of the parietal peritoneum results in a well-localized, somatic pain (GSA), right lower quadrant or right flank region = pain GSA commonly located at McBurney's point: 1/3 between ASIS and the umbilicus, used to approximate the appendix region) |
|
|
*** 1. Hyperactive bowel sounds 2. Increased risk colorectal cancer 3. Bloody stool, weight loss, change in stools 4. Ischemia and necrosis in ileocolic region 5. Rectal bleeding, LLQ pain. 6. Pain LLQ only |
1. bowel osbtruction 2. ulcerative colitis 3. colorectal cancer 4. intussusception 5. diverticular disease 6. appendicitis |
|
|
Colorectal carcinoma ** (CS 47) > Sx > Mech |
Sx: > may be asymptomatic but as tumor growths: bloody stool, weight loss, changes in stool (decreased caliber, diarrhea) and malaise Spread: > local growth: peritoneum, pelvic organs > lymph > veins: Caval system, Batson's plexus (brain), vertebrae, lungs (caval system), liver (portal system) |
|
|
Intussusception ** (CS 46) > patho > sx |
Patho
> Telescoping of a proximal gut segment into the lumen of an adjacent segment) Sx > Ischemia, necrosis (most commonly ileocolic region) |
|
|
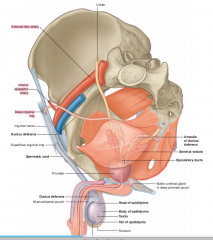
Digital rectal exam * > palpable structures |
Male > bladder, segminal vesicles, ductus deferens, prostate, perineal body, bulb penis Female > vagina, cervix, perineal body |
|
|
Which of the following is not palpable via the digital rectal exam in males according to CS? ** (CS 42) a. bladder b. seminal vesicles c. epididymis d. ductus deferens e. prostate f. perineal body g. bulb penis |
Epididymis rest are shown on CS |
|
|
Colostomy ** (CS 48) > indications > procedure |
Need > Diseases affecting the LI = Colon cancer = Diverticulitis Procedure > When it is necessary to let a distal portion of th ecolon heal, the proximal portion o the colon is sutured to an opening, stoma along the anterior abdominal wall, via the rectus abdomens muscle where waste products are expelled |
|

Describe *** (CS 49) |
Rectal prolapse: > protrusion of the rectal wall into the anal canal or via the anal opening Characterization > protrusion of a reddish, mucosal mass into the anal canal (most commonly related to longstanding hemorrhoids), associated with constipation, malnutrition and prior rectal trauma |
|
|
Rectal prolapse *** (CS 49) |
> protrusion of the rectal wall into the anal canal or via the anal openingCharacterization> protrusion of a reddish, mucosal mass into the anal canal (most commonly related to longstanding hemorrhoids), associated with constipation, malnutrition and prior rectal trauma |
|
|
*** 1. Long standing hemorrhoids 2. Change bowel habits 3. Hyperactive bowel sounds 4. Peritonitis 5. Anorexic young woman |
1. rectal prolapse 2. colorectal carcinoma 3. bowel obstruction 4. Diverticular disease 5. wilkie's syndrome (Superior mesenteric artery syndrome) |
|
|
*** 1. Loss blood flow in Sudeck's and Griith's points 2. 3. Constipation, prior rectal trauma |
1. Ischemic colitis (pain, bloody stools) 2. 3. rectal prolapse |
|
|
Upper GI bleeding ** (CS 51) > Sx > Cause |
Sx > hematemesis (vomiting blood) > black tarry stool (melon) Cause > upper GI bleeding (stomach, duodenum) Due to: > stomach cancer > ulcers > gastritis > esophageal varices |
|
|
Lower GI bleeding ** (CS 51) > Sx > Cuase |
Sx > hematochezia (red or maroon colored stool) Causes > Low GI bleed = diverticular disease = polyps = hemorrhoids = anal fissures = cancer = IBD |
|
|
Rectocele ** (CS 50) > Sx > Patho |
Patho > weakness in puborectalis, pubovaginalis muscles resulting in bulging of the rectal wall into the posterior vaginal wall Sx > painful intercourse or bowel movements > constipation > sense of fullness > can lead to rectal prolapse |
|
|
Ischemic colitis *** > patho > sx |
Poor blood flow (atherosclerosis, hypovolemia, hypo perfusion, Sickle CA) > poor blood flow, especially in important watershed/susceptible areas: = Griffith's point (Splenic flexure) : middle colic > let colic = sudeck's point (rectos-sigmoidal junction) : last sigmoidal > superior rectal Sx: > pain, blood stool |
|
|
Spleen ** (CS 53) > location > pathologies |
Location > Midaxillary between 9th-11th ribs Pathologies Splenic rupture: Patho: prone rupturing, since: = thin outer capsule, contact w/ ribs 9-11 on left side) = soft Sx > Left shoulder pain (ruptured spleen), due to irritation diaphragm/peritoneum (Kehr's sign) Splenomegaly Patho: enlarged in numerous inflammatory or degenerative conditions Sx > enlarged spleen palpable below the left costal margin and displace the splenic flexure from the colon |
|
|
Liver ** (CS 54) > trauma > hepatomegaly > variations in liver? > significance of portal lobes |
Trauma > in living, liver soft and covered by a thin capsule, thus lacerations or puncture wounds to the liver will often result in hemorrhage Hematomegaly > caused by: CHF, Cancer, alcoholic cirrhosis Variations > there are significant variations in the origin of the hepatic arteries, they may arise from the left gastric artery or aberrant hepatic arteries penetrating the left lobe directly Significance portal lobes > knowledge of the functional segmentation of the liver permits removal of diseased vascular segments |
|
|
Possible sources blood supply to the liver ** |
> Hepatic artery property > Left gastric artery (*CS 54, there are many variations in the blood supply to the liver) |
|
|
Which of the following is a possible blood supply to the liver?* a. splenic artery b. gastroduodenal artery c. renal artery d. left gastric artery e. right colic artery f. cystic artery |
left gastric artery (*CS 54, there are many variations in the blood supply to the liver, the left gastric artery is one possible method blood supply to the liver ) |
|
|
Lymph drainage from the liver ** > amount lymph to where total? > specific drainages from certain areas > most common metastatic origin of the liver? reason? |
amount lymph > liver is a major lymph producing organ, about 50% of the lymph in the thoracic duct arises from the liver Lymph drainag of the liver > lymph from most liver > hepatic node > celiac node > lymph from bare area liver > phrenic node > posterior mediastinal node > lymph from falciform ligament > parasternal nodes > lymph from round ligament > umbilical nodes Most common metastatic origin of the liver > right breast, since the liver has so much lymphatics |
|
|
What is the most likely origin of hepatic cancer? ** a. left kidney b. right kidney c. stomach d. gallbladder e. left breast f. right breast g. duodenum h. jejunum i. ileum j. ascending colon |
right breast > right breast, since the liver has so much lymphatics |
|
|
*** Include the next route of the node as well. 1. Lymph around falciform ligament 2. Lymph around round ligament 3. Lymph around bare area liver 4. Lymph of most of the liver a. hepatic nodes b. phrenic nodes c. parasternal nodes d. nodes around umbilicus and anterior abdominal wall |
1. parasternal nodes 2. nodes around umbilicus (and anterior abdominal wall ) 3. phrenic nodes > posterior mediastinal nodes 4. hepatic nodes > celiac nodes |
|
|
*** Include all pathways 1. Celiac nodes receive what drainage? From where? 2. Posterior mediastinal nodes receive what drainage? From where? 3. Round ligament drains to what. a. hepatic nodes b. phrenic nodes c. parasternal nodes d. nodes around umbilicus and anterior abdominal wall |
1. hepatic nodes, mode liver 2. phrenic nodes, bare area liver 3. nodes around umbilicus and anterior abdominal wall |
|
|
*** 1. Falciform ligament to 2. Bare area liver to 3. Round ligament to a. hepatic nodes b. phrenic nodes c. parasternal nodes d. nodes around umbilicus and anterior abdominal wall |
1. parasternal nodes 2. phrenic nodes > posterior mediastinal nodes 3. nodes around umbilicus |
|
|
Explain variation within the biliary tree ** (CS 56) |
There is significant variation in the branching of: > hepatic ducts > cystic ducts > bile duct > as well as location major duodenal papilla |
|
|
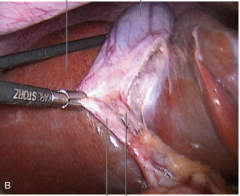
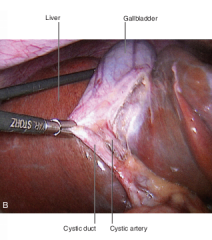
Carlot's triangle *** (CS 57) > boundaries > components |
Boundaries > bound by = cystic duct = common hepatic duct = base liver Contents > cystic artery, vein > lymph nodes > autonomic nerve fibers > any anomalous ducts |
|
|
Portal triad ** (CS 58) > contents > procedures |
Contents > hepatic artery proper > hepatic portal vein > common bile duct > lymphatics > CN X (Vagus nerve) Pringle's maneuver > during bleeding during hepatic procedures, clamping vessels of the portal triad = locaiton at tfree edge of the lesser momentum, the hepatoduodenal ligament |
|
|
Jaundice *** (CS 59) > types > causes |
Types > prehepatic: excessive breakdown RBC > hepatic: disruption liver functino (i.e: cirrhosis) > obstructive jaundice: if bile can not escape the gallbladder or biliary tree (b/c of gall stones), it enters blood and causes jaundice Causes: > liver cirrhosis |
|
|
Liver cirrhosis *** (CS 60) > patho > sx |
Patho > atty and or fibrous C/T impedes blood flow through the liver sx > hepatomegaly, ascites, edema, jaundice, splenomegaly, and portal hypertension |
|
|
Sites of portal - naval anastomoses *** (CS 61) |
Portal vein / caval vessel / presentation: left gastric veins / esophageal veins / esophageal varices superior rectal veins / middle and inferior rectal veins / hemorrhoids paraumbilical veins / superior epigastric veins // caput medusae veins along bare area of the liver / inferior phrenic veins / bleeding risk |
|
|
Blood flow in portal veins *** (CS 62) Stomach cancer will cause what?? *** |
Right lobe > receives venous drainage from mid gut (intestines) Left lobe > receives venous drainage from stomach, spleen stomach cancer > will impact the left lobe of the liver since stomach venous flow tends to drain into the left lobe of the liver |
|
|
Gall stones *** > risk factors > patho |
Risk factors > Fs: fat, fertile, female over 40 (obese, multiparous, female > 40) Patho > areas common gall stones = fundus: may result in air within the biliary tract, may form a cholecysto-colonic fistula = bile duct (common bile duct): block hepatic secretions = hepatopancreatic ampulla (ampulla) of vater: block hepatic and pancreatic secretions |
|
|
*** 1. Obstruction where block hepatic and pancreatic secretions 2. Obstruction where blocks hepatic secretions 3. Obstruction where may form a cholecysto-colonic fistula a. fundus b. body c. neck d. bile duct e. cystic duct f. ampulla of vater g. hepatic vein |
1. ampulla of vater (hepatopancreatic ampulla) 2. bile duct 3. fundus |
|
|
Cholecystitis *** > patho > sx |
Patho > inflammation of the gallbladder via gallstones blocking the cystic duct, resulting in inflammation of the gallbladder sx > pain in epigastric, shifting to right hypochondriac region at junction 9th costal cartilage and line semilunaris > right shoulder (b/c gallbladder irritates diaphragm, which receives C3-C5 phrenic innervation), |
|
|
Pancreatitis *** > patho > result |
Patho: inflammation of the pancreas (often sequela of gallstones, retrograde flow bile into pancreatic duct) Result: block pancreatic ducts |
|
|
Lymphatic drainage of the pancreas *** > cancer spread in pancreas? |
B/c gland at crossroads of foregut and midgut, pancreas drains into both: celiac and superior mesenteric nodes Pancreatic cancer > often spreads into para aortic (lumbar nodes) |
|
|
Pancreatic cancer *** > patho > sx |
Patho > pancreatic cancer causes obstruction of the bile and pancreatic ducts Sx > weight loss, abdominal /back pain, obstructive jaundice (retention bile pigments), painless, palpable gallbladder, jaundice |
|
|
*** CS 1. Abdominal/back pain, painless, palpable gallbladder, jaundice 2. Right hypochondriac pain and right shoulder pain 3. Back up venous flow from left gastric veins 4. breast cancer metastasis 5. Kehr's sign |
1. pancreatic cancer 2. cholecystitis 3. esophageal varices 4. liver cancer (especially right breast) 5. Spleen pain, left shoulder pain associated w/ irritation diaphragm, peritoneum |
|
|
** CS 1. sudden testicular pain 2. Griffith point severed 3. hematuria, flank pain |
1. torsion of the testis 2. ischemic colitis > (griffith point or splenic flexure) from middle colic A > left colic A affected Sx:pain, bloody stool 3. varicocele |
|
|
Abdominal esophagus location *** > innervation > arterial supply |
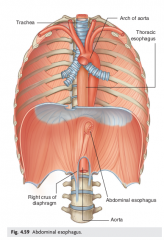
Emerging right crus of diaphragm usually at level V 12 Passes from esophageal hiatus to cardial office of stomach just left midline (See diagram drawn, organ notes) Innervation > anterior and posterior ends esophagus innervated by left and right portion vagal nerve Arterial supply > esophageal branches from left gastric A (from celiac trunk of AA) > esophageal branches from left inferior phrenic artery from AA (see drawn diagram, organ notes) |
|
|
Where would the jejunum be located**? |
LUQ |
|
|
Superior duodenum *** > span > anterior/posterior/medial |
Span > pyloric stomach - neck Gallbladder Anterior > Bile duct, gastroduodenal artery, Portal vein, IVC |
|
|
Inferior duodenum *** > A/P/M |
Posterior > SMA, SMV Anterior > IVC, Aorta, vertebral column |
|
|
Ascending duodenum *** > A/P/M |
Lateralaorta |
|
|
Area between duodenojejunal fissure * |
ligament of Treitz |
|
|
Ligament of Treitz * |
Duodenojeunal flexure |
|
|
Jejunal, ileum locations *** |
Jejunal: LUQ (left hypochondrium) Ileum: RLQ |
|

Label *** |

|
|
|
What organ contains place circularis according to Greys*? a. duodenum b. jejunum c. ileum d. colon |
jejunum |
|
Label *** |
|
|
|
Sub diaphragmatic gas noticeable * explanation** |
perforation stomach or dudodenal uclers |
|

Label ** |
|
|
|
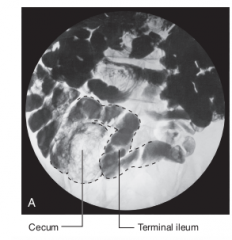
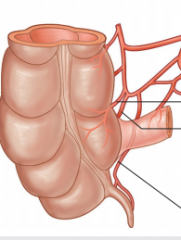
CECUM Intra/retroperitoneal? Reason * |
Intraperitoneal b/c of its mobility not b/c of its suspension by a mesentery (Greys 32) |
|
|
Blood supply to the appendix *** |
aNTERIOR CECAL, POSTERIOR CECA AND APPENDICULAR ARTERIES FROM THE ILEOCOLIC a. (FROM sma) |
|
Label everything, include other relevant parts not shown as well *** |
|
|
|
Colon intra/retroperitoneal ? ** |
Ascending, descending colon: retroperitoneal Transverse, sigmoid colon: intraperitoneal |
|
|
Neck pancreas location *** |
Anterior: > Superior mesenteric vessels (SMA, SMV) > Splenic vein = SMV, Splenic vein join to form portal vein |
|
Label *** |

|
|
|
Spleen * > location > covering > A |
Location connecteed to: > stomach via gastrospleno ligament > left kidney via splenorenal ligament ==> both above ligaments part of the greater momentum > lateral at splenic hilum: neck pancreas Covering > covering with visceral peritoneum except at splenic hilum A > splenic artery (from celiac trunk of SMA) |
|
|
Splenic artery > location *** > function |
Posterior stomach > Takes a tortuous path to the Left along superior border pancreas Function > tRAVELS IN SPLENORENAL LIGAMENT DIVIDING INTO NUMEROUS BRANCHES WHICH ENTER HILUM SPLEEN. |
|
|
Explain biliary area *** > location, orientation > diagram shown |
Portal vein anterior hepatic artery proper Hepatic artery proper divides into right and left hepatic arteries > right hepatic artery divides into the cystic artery along the way HAP, portal vein to the left of the cystic duct, common hepatic duct and bile duct (combination of cystic duct and common hepatic duct) Posterior to all > IVC Diagram |
|
|
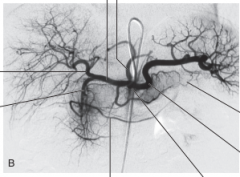
SMA *** > orientation > supplies > diagram shown |
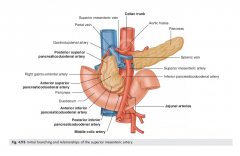
Mimed below celiac trunk Posterior: > neck pancreas > superior portion duodenum > splenic A Anterior > inferior portion duodenum > LRV > Uncinate process pancreas Supplies > jejunal A > Ileal A > Ileocolic A > Right colic A > medial colic A |
|
|
Portal vein *** > orientation > formation > diagram |
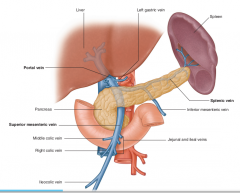
Orientation > As it ascends towards liver> posterior superior part duodenum + enters right margin lesser omentum= Anterior omental foramen= Posterior bile duct (to the right) + hepatic artery proper (slightly left) Formation > Splenic and SMA join posterior neck pancreas (right side) (see diagram drawn) |
|
|
Renal vessel locations ** > diagram shown |
Left renal vein: posterior > SMA anterior > abdominal aorta ==> left renal vein can be compressed by an aneurysm in either of these (See drawn diagram ) Renal arteries: Right renal A > longer than LRA, posterior: > IVC |
|
|
Ureters *** > common areas constriction > arterial support > diagram shown |
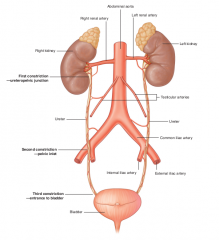
Areas constriction > ureteropelvic area > L4, Common iliac artery bifurcation into external and internal iliac arteries > entrance bladder Arterial support > right arteries > testicular/ovarian arteries > common iliac arteries > internal iliac arteries |
|
|
Pancreatic cancer *** (CS 68) explain result |
Result > obstruct bile + pancreatic ducts = weight loss, abdominal/back pain, obstructive jaundice, painless, palpable gallbladder ('Courvoisier sign') and jaundice > obstruction of portal vein + IVC (See diagram, notes for visualization) > metastasis via: = regional spread to adjacent organs = any peritoneal surface, local nodes = liver |
|
|
A patient has an enlarged gallbladder and jaundice with no pain. It is expected that metastasis will occur where ? ** a. gallbladder b. kidney c. pancreas d. liver e. duodenum f. stomach g. spleen h. brain i. vertebrae |
liver expl: These are sx of pancreatic cancer, enlarged GB with no pain (Conservier sign) Pancreatic cancer is most likely to metastasize to the liver (regional spread to adjacent organs, any peritoneal surface, local nodes as well ) CS 68 |
|
|
** Splenectomy complications . (CS 70) |
> Removal of spleen endangers the pancreatic tail > If the pancreatic tail is damaged, digestive enzymes can be released into the abdominal cavity |
|
|
** (CS 71) Patient has an abdominal aorta aneurysm. > Cause > Clinical manifestations |
Cause > Congenital or acquired dilation of the wall of the abdominal aorta Sx > palpable abdominal aorta left of the midline > pulsatile non tender mass below the umbilicus) > fatal if ruptured > Sx = Compression of adjacent structures (anterior: vertebrae) (posterior: left renal vein, pylori stomach, superior and inferior duodenum) |
|
|
Patient has a pulsatile contender mass below the umbilicus. Dx? * |
Abdominal aortic aneurysm |
|
|
Aortic dissection * (CS 71) > cause > sx |
Cause > tear in the intimal inner layer of the aorta and hemorrhage between layers o the vessel Sx > acute onset back/chest pain, lower extremity ischemia, neuropathy, pulse deficits in lower extremities |
|
|
Patient has acute onset of back/chest pain and lower extremity ischemia * |
Aortic dissection |
|
|
Patient has neuropathy , pulse deficit sin lower extremities Dx? * |
Aortic dissection |
|
|
Obliteration of the abdominal aorta *** (CS 72) > patho > result |
Patho > gradual buildup of plaque in the abdominal aorta, at the bifurcation of the abdominal aorta (L4), Lerich syndrome Sx > leg pain (claudication), impotence Result > aorta to aorta anastomoses since the gradual nature of this condition permits significant collateral circulation to develop = SMA > middle/inferior rectals > internal iliac = intercostals, subcostal, lumbar > iliolumbar, sup. gluteal > intenral ileac = intercostal, subcostal lumbar > circumflex iliac > external iliac = subclavian > internal thoraci c> superior epigastric > inferior epigastric > external iliac |
|
|
Result IVC obstruction * (CS 74) |
3 sets of tributaries permit venous return from lower extremity (caval-caval anastomoses > IVC to SVC) > inferior to superior epigastric > superficial epigastric to lateral thoracic (th oracoepigastric) > vertebria/lumbar veins + Batson's plexus to azygous system |
|
|
Inferior vena cava filters sgifnicaince * |
recurring blood clots arising form the veins in the lower extremity can be treated by placing a filter / screen in the IVC (below level o renal veins), clot buildup can present as naval obstruction |
|
|
Psoas fascia ** > explain > attachments > innervations > blends with ? > funciton > tests for pathos |
> Psoas major muscle is covered by a stocking like covering of investing fascia > Attachment to psoas major = Lateral surface bodies T12 + L1 - L5- Lesser trochanter of femur Innervation > AR L1-L2 Blends with: > medial arcuate ligament, fascia of quadrates lumborum and iliacus Function > flexion of thigh at hip Tests > > thomas test |
|
|
Psoas major tests *** (CS 78, 79) |
Posts major test/sign > Patho: Inflamed retrocecal appendix can impact function o the right posts major > Test = Passively extend patient's hip, asking him to actively flex the thigh at hip ( Abdominal pain indicates + test) Thomas test > Patho: Dysfunction/contracture of psoas major muscle > Test: Patient lays on back, examiner flexes patients hip. = Dysfunction of the psoas major muscle is indicated when the test reveals flexion of the contralateral hip without knee extension |
|
|
* A physician is performing the Thomas test 1. What muscle is being tested? a. quadratus lumborum muscle b. ileacus muscle c. psoas muscle d. external oblique muscle e. internat oblique muscle f. transversus abdominis muscle g. rectus abdominis muscle h. pyramidalis muscle 2. The test is positive when what occurs? |
1. psoas muscle 2. contralateral flexion of the psoas muscle without knee extension after the examiner flexes the patient's hip |
|
|
*** 1. The examiner passively extends the patient's hip and asks him to actively flex at thigh. Pain was produced. What muscle is effected? a. quadratus lumborum muscle b. ileacus muscle c. psoas muscle d. external oblique muscle e. internat oblique muscle f. transversus abdominis muscle g. rectus abdominis muscle h. pyramidalis muscle 2. Purpose of this? * |
1. (right) psoas muscle 2. Performed to detect inflamed retrocecal appendix Active flexion of thigh at hip after passively extending patient's hip and + abdominal pain is + for inflamed retrocecal appendix |
|
|
Arterial supply abdominal ureter ** (CS 88) > significance? |
Abdominal ureter > medial side Pelvic ureter > lateral side ==> This should be considered in retraction of the ureter during surgery |
|
|
Urinary obstruction *** (CS 87) > cause > result > sx |
Cause > stones, tumors, prostatic hypertrophy > kidney stones (nephrolithisias) or uremic calculus Result: > hydronephrosis, enlargement o the ureter, renal pelvis and or/calyces, renal failure Sx renal stones > pain (renal colic, anywhere form flank to groin), depending on location (renal pelvis, ureter, bladder) > N&V, hematuria |
|
|
Surface markings abdomen (slides 3-4) *** |
XP (T6), T6 dermatome Umbilicus, T8, T8 dermatomes Costal margin, T10 Linea alba (XP -Pubic symphysis between 2 rectus abdomens muscles) Linea semilunaris (pubic tubercle - 9th rib) > separating rectus abdominis muscles Iliac crest (L4) ASIS (L4-L5) Pubic tubercle (ASIS - pubic tubercle) > 1 on each side pubic syphysis Inguinal ligament spermatic cord |
|
|
Linea semilunaris location *** > diagram shown |
Pubic tubercle - 9th rib > separating rectus abdominis muscles |
|
|
Inguinal ligament *** > location > structure > label on shown diagram |
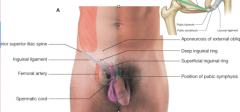
location > ASIS, pubic tubercle > near inguinal canal structure: > external oblique aponeuroses |
|
|
spermatic cord layers*** (from out to in) |
skin, campers fascia, dartos fascia, external spermatic fascia (derived from external oblique aponeuroses), cremaster fascia (derived from internal oblique aponeuroses), internal spermatic fascia (derived from transversals fascia) > pampiniform plexus (venous system cooling venous blood before reaching testis) |
|
|
Surface markings viscera *** (Slide 9) |
Diaphragm > Right: 5th rib, Left: 5th Intercostal space Gallbladder > Crosses body surface, in contact diaphragm > Rt. 9th rib - semiliunar line Spleen > Lt (midaxillary in contact ribs 9, 10, 11) liver * > ribs 8, 9, 10 Kidney > scapular line, superior lobes at rib 11 |
|
|
Describe fascial layers of the lower abdomen *** (slide 10) |
fascia of the Lower anterior abdomen divided into 2 areas in abdomen + thigh layers fascia: > adipose - Camper’s fascia > scarpa’s fascia, fibrous tissue (allow skin move easily over muscle) (deeper part superficial campers fascia), blends into perineum Conversions (same layers, different name) = Dartos: over scrotum = fascia lata: thighColles (Superficial perineal fascia): between legs = Fundiform ligament (both genders)proeprtiesmore prominent males location - malesextensions of deeper membranous layer of superficial fascia attached to pubic symphysis pass inferiorly onto the dorm and lateral parts of penis forming fungiform ligament of the penis - femalescontinues into labia majora and anterior part perineum functionsuspends penis to body wall |
|
|
Explain innervation abdominal wall *** |
innervation: T7-L2, Intercostal nerves all the way to T12, then pick up L1, L2T7-T12 properties > Approaching midline, anterior cutaneous branch passes via rectus abdominis muscle + anteiror wall of rectus sheath to supply the skin (add flashcard) T7T8T9 T10: Umbilicus T11T12 SubcostalFunction T7-T12, L1 branches to anterolateral abdomianl wall and parietal peritoneum T7-T9: skin from xiphoid process to above umbilicus T10: skin around umbilicus T11-L1: below umbilicus - and including pubic region L1 (ilioinguinal nerve)anterior surface scrotum/labia major, small cutaneous branch to the thigh |
|
Label relevant * > location? |
Anterolatearl abdominal wall |
|
|
*** 1. Medial to the psoas major 2. Lateral to the psoas major 3. Anterior psoas major 4. Supplies skin on anterior and lateral thigh to knee level a. ilioinguinal nerve b. genitofemoral nerve c. obturator nerve d. femoral nerve e. subcostal nerve f. iliohypogastric nerve g. intercostal nerves |
1. Superior sacral (ck name) 2. L1 both, Femoral (AR L2-L4), Obturator nerve (AR L2-L4) 3. Genitofemoral nerve (AR L2) 4. lateral cutaneous (AR L2-L3) |
|
|
*** 1. Supplies anterior thigh and medial surface leg. 2. Upper anterior thigh 3. Sensory medial upper thigh 4. Medial compartment thigh 5. Supplies pubic region 6. Supplies scrotum 7. Cremasteric muscle innervation a. ilioinguinal nerve b. genitofemoral nerve c. obturator nerve d. femoral nerve e. subcostal nerve f. iliohypogastric nerve g. intercostal nerves |
1. femoral nerve (AR L2-L4) 2. femoral branch genitofemoral nerve 3. ilioinguinal nerve 4. obturator nerve (AR L2-L4) 5. iliohypogastric nerve 6. ilioinguinal nerve 7. genital branch genitofemoral nerve |
|
|
Insertion of a needle through the abdominal wall at the region indicated. All layers *** (Slide 26) |
Skin, Campers fascia, dartos fascia, external oblique muscle, internal oblique muscle, transversals fascia/muscle, endoabdominal fascia, parietal peritoneum |
|
|
Arcuate line *** (slide |
Arcuate line: > horizontal line that demarcates lower limit of posteriorregion of rectus sheath= at a pt midway between umbilicus and pubic symphysis,corresponding beginning lower 1/4 of rectus abdomens,all aponeuroses move anterior to rectus muscle, from this point inferior, rectus abdomens muscle in directcontact w/ transversalis fascia, making arcuate line. > where inferior epigastric vessels perorate rectus abdominis |
|
|
*** 1. Compresses abdominal contents, flexing trunk, bending trunk and turning anterior abdomen to same side. 2. Flex vertebral column 3. Compresses abdominal contents, flexing trunk, bending trunk and turning anterior abdomen to opposite side |
1. internal oblique 2. rectus abdominis 3. external oblique |
|
|
Externat oblique muscle * > attachment > innervation > function > diagram shown |
Attachment > Ribs 5-12 - Lateral lip iliac crest (ending linea alba) Innervation > T7-T12 Function > compress abdominal contents > flex trunk > bend trunk same side, turning anterior part of abdomen to opposite side |
|
|
Internal oblique muscle * > attachment > innervation > function > diagram shown |
Attachment > thoracolumbar fascia, iliac crest, lateral 2/3 inguinal ligament - inferior broder lower 3 or 4 ribs Innervation > AR T7-T12 and L1 Function > compress abdominal contents > flex trunk > bend trunk and turning anterior part of abdomen to same side |
|
|
Transversalis muscle * > attachment > innervation > function > diagram shown |
attachment > thoracolumbar fascia, medial lip iliac crest, lateral 1/3 inguinal ligament, costal cartilages lower 6 ribs - Aponeuroses ending linea alba Innervation > T7-T12 and L1 Function > compress abdominal contents Only |
|
|
What contains umbilical artery remnants *? a. median umbilical ligament b. medial umbilical ligament c. inguinal ligament d. lateral umbilical ligament |
medial umbilical ligament |
|
|
Hesselbach's triangle *** > borders > significance (slide 28) |
Borders > base: inguinal ligament > medial: rectus abdominis > lateral: inferior epigastric artery |
|
|
inguinal canal ***(slide 32) > structure > components |
structure > fibromuscular canal formed by the layers comprising anterior abdominal wall components > superficial inguinal ring: opening in external oblique muscle > deep inguinal ring: opening in transversals fascia > conjoin tendon: internal oblique and tranversalis abdominis |
|
|
Superficial inguinal ring formed via what * |
opening in external oblique muscle |
|
|
deep inguinal ring formation *** |
opening in transversalis fascia |
|
|
conjoin tendon formation * |
internat oblique and trasnversalis |
|
|
Cremaster muscle *** (slide 36) > structure > innervation |
Structure > the cremaster is an extension of the fibers of the internal oblique muscle Innervation > genitoemoral nerve |
|
|
*** 1. Cremaster is an extension of the fibers of the: 2. Superficial inguinal ring formed via opening in: 3. Deep inguinal ring formed via: a. external oblique muscleb. external oblique fascia c. internat oblique muscle d. internal oblique fascia e. transversalis muscle f. transversalis fascia g. linea alba h. rectus abdominis i. rectus sheath j. arcuate ligament |
1. internal oblique muscle 2. external oblique muscle 3. transversalis fascia |
|
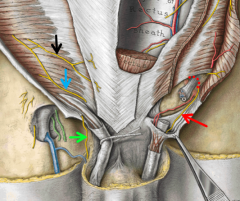
Label *** (slide 39) |
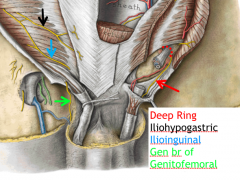
|
|
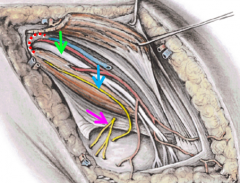
Label *** (slide 40) |
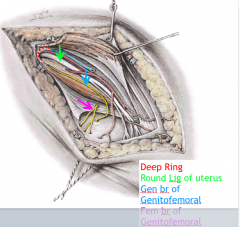
|
|
|
Considerations cutting ductus deferent *** (slide 42-43) > explain |
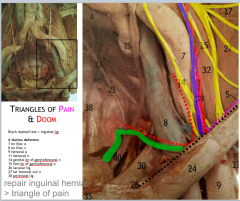
Cutting the external iliac artery |
|
|
Direct inguinal hernia *** (slide 44) |
> properties = traverse anterior abdominal wall medial to inferior epigastric vessels, passing directly via Hesselbach's triangle = covered parital peritoneum, transversals fascia= does not traverse entire inguinal canal, b/c usually does not enter deepinguinal ring, but emerges from superficial ring = outside spermatic cord = can go into scrotum |
|
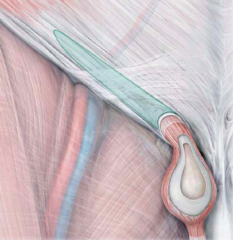
Explain *** |
Indirect (via entire inguinal canal) |
|
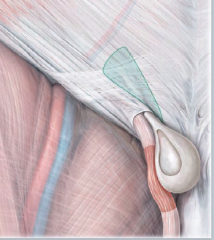
Explain *** |
Direct (not via entire inguinal canal) |
|
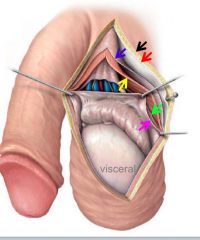
Label *** (slide 50) |
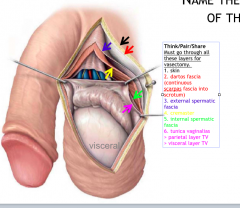
|
|
|
Layers from external to inferior testis ** (slide 50) |
> Skin, darts fascia (continuous scarpas fascia into testes), external spermatic fascia, cremaster, internal spermatic fascia, parietal layer tunica vaginalis, visceral layer tunica vaginalis |
|
|
Explain testicular venous drainage Possible pathologies (slide 52) Diagram shown *** |
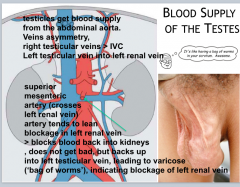
Right testicular vein > directly IVC Left testicular vein > left renal vein ==> Asymmetry Blockage left renal vein > cause: Superior mesenteric artery compression of left renal vein (b/c anterior left renal vein, see diagram drawn) >result: Backup of blood from left renal vein into the left testicular vein ==> Varicocele |
|
|
Testicular and scrotal cancer/infection spread where *** (slide 55) |
Testicular cancer: lumbar (para aortic) nodes Scrotal infection: superficial inguinal node |
|

Explain *** (slide 56) |
Direct inguinal hernia |
|

Explain *** (slide 57) |
Hydrocele Cause: Most likely patent ductus vaginosis, causing fluid to accumulating in tunica vaginalis Dx: Transillumination |
|
|
*** (slide 58) 1. What layers must be cut? 2. Structures at most in danger of iatrogenic injury? 3. Nodes at risk with infeciton |
1. skin, darts fascia (scraps fascia in scrotum) > external spermatic fascia > cremaster > internal spermatic fascia > parietal layer tunica vaginalis > visceral layer tunica vaginalis 2. Testicular artery, vein Genital branch genitofemoral nerve (innervates cremaster muscle to retract scrotum) 3. superficial inguinal nodes |
|

*** (slide 60) Dx? Patho Ix (all the components, considerations of procedure) |
Dx: ascites Patho: accumulation fluid Paracentesis > skin, campers fascia, scraps fascia, external oblique muscle, internal oblique muscle, transversals muscle, endoabdominal peritoneum, parietal peritoneum (before) peritoneal cavity Clinical applications > Place bolus of local anesthetic into the pudendal canal, anesthetizing the pudendal nerve and its branches |
|
Explain *** |
ascites (top left dark grey fluid) > light grey is the liver |
|
|
changes with breathing *** |
changes abdominal cavity with breathing: > inspiration = contraction diaphragm = relaxation abdominal muscles > expiration = relaxation diaphragm = contraction abdominal muscles |
|
|
Abdominal wall ** > span |
Thoracic diaphragm > pelvic inlet occupying abdominal proper and greater pelvis |
|
|
Abdominal land marks **(slide 63-64) |
transpyloric plane: L1-L2 Transumbilical plane: L3-L4 |
|
|
peritoneum divisions *** |
divisions > greater sac = most space in peritoneal cavity, spanning superiorly at diaphragm - pelvic cavity > lesser sac (omentum bursa) omenta (2 layers periotneum combined) > greater omenta (greater curvature stomach - Ileum, SI) = derivation dorsal mesentary > lesser omenta (lesser curvature stomach + 1st part duodenum - inferior surface liver, either liver and stomach or liver and duodenum ) = derivaiton ventral mesentary (lateral hepatoduodenal ligament: contains portal vein: hepatic after proper, portal vein, bile duct ) (medial hepatogastric ligament) folds peritoneum Function: allow movement, provide conduit for N, V, L to reach viscera, attach viscera to posterior abdominal wall > the mesentery > sigmoid mesocolon > transverse mesocolon = ligaments: splenorenal ligament (connect kidney to spleen), gastrophrenic ligament (connect stomach to diaphragm) |
|
|
*** 1. Which of the following contains the portal triad ? a. medial hepatogastric ligament b. lateral hepatoduodenal ligament c. splenorenal ligament d. gastrophrenic ligament |
lateral hepatoduodenal ligament ( of the lesser omentum) |
|
|
*** 1. Which of the following contains the portal triad ? 2. What is found in the lesser omenta? 3. What is found in the mesentaries? a. medial hepatogastric ligament b. lateral hepatoduodenal ligament c. splenorenal ligament d. gastrophrenic ligament |
1. lateral hepatoduodenal ligament 2. medial hepatogastric ligament, lateral hepatoduodenal ligament 3. splenorenal ligament, gastrophrenic ligament |
|
|
*** 1. What derived from ventral mesentery? 2. What derived from dorsal mesentery? 3. What is over the jejunum and ileum? |
1. lesser omentum 2. greater omentum, all mesenteries (mesentery, transverse mesocolon, sigmoid mesocolon) 3. the mesentery |
|
|
*** Explain the mesentery |
Large fan shaped double layered fold of peritoneum that connects jejunum and ileum to posterior abdominal wall |
|
|
What does the mesentery connect?*** a. duodenum and jejunum b. jejunum c. jejunum and ileum d. duodenum and ileum e. duodenum, jejunum, and ileum f. transverse colon g. sigmoid colon 2. The mesentery derived from what? *** 3. Greater omentum derived from what? 4. Lesser omentum derived from what? a. ventral mesentary b. dorsal mesentary c. lateral mesentary d. medial mesentary |
1. jejunum and ileum 2. dorsal mesentary 3. dorsal mesentary 4. ventral mesentary |
|
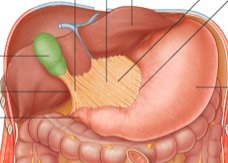
*** Label |
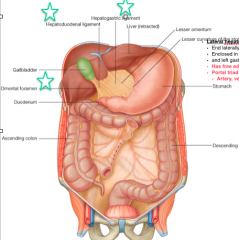
|
|
|
Areas peritoneal cavity *** |
Greater sac Lesser sac (omental bursa) > potential recess posterior stomach > entry: epiploic foramen (of Winslow), only normal pt of entry to the mental bursa = posterio wall: periotneum over posterior wall, pancreas, transverse mesocolon = anterior wall of lesser sac, back stomach, greater and lesser momentum |
|
|
Epiploic foramen (of winslow) * (slide 73) |
Only normal point of entry into the mental bursa (lesser sac) |
|
|
Only normal point of entry into the mental bursa (lesser sac)* (slide 73) |
Epiploic foramen (of winslow) * |
|
|
phrenocolic ligament *** > composed of > location |
composed of > transverse colon, descending colon location > left parabolic gutter H |
|
|
How does a bursted or infected appendix cause problems * > route |
Via right paracolic gutter Not left parabolic gutter b/c there is the phrenocolic ligament there |
|
|
Explain digestive organ innervation *** |
Autonomic innervation (SNS, PSNS, sensory axons) organs innervated in a 'viscerotomal ' pattern >> except oral cavity and anus |
|
|
Properties LI *** (Slide 91) > label on diagram |
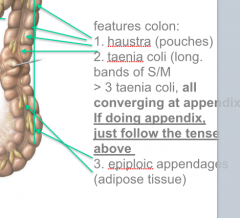
> Haustrations (POUCHES) >Taenia coli (Long bands S/M) = All 3 taenia coli converging at appendix > Epiploic appendages (adipose tissue) |
|

Label *** (slide 91) |
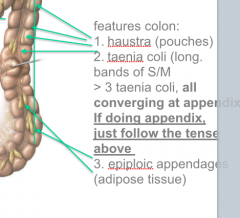
|
|
|
Explain the transition from jejunum to ileum in the mucosa *** |
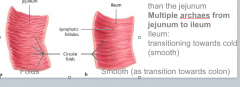
Plica circularis (circular folds( in jejunum Less in ileum |
|
|
McBurney's point *** > location > show on diagram |
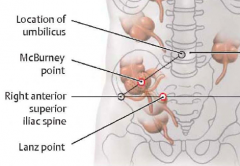
Middle 1/3 from ASIS to umbilicus (T10) or umbilical plane (L3-L4) |
|
|
Stomach in contact with what anteriorly and posteriorly *** (slide 87) |

|
|

Describe *** slide 94 |
On right side, haustration b/c has white contrast |
|

Describe *** > slide 95 |
stomach |
|
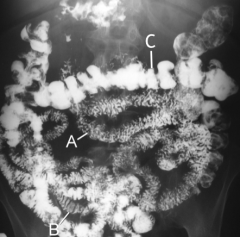
*** Label a-c |
A: Jejunum B: Ileum C: Transverse colon |
|
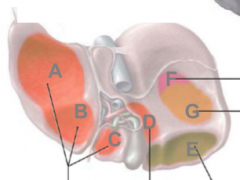
Label A-G *** |
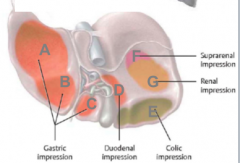
|
|
|
How is liver connected to the body wall *** (slide 99) |
falciform ligament |
|
|
falciform ligament *** |
divides liver into left and right lobes connects liver to body wall |
|
|
**** 1. Division IVC and falciform ligament 2. Division body GB + falciform ligament > on diagram |
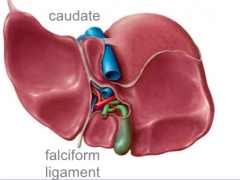
1. Caudate lobe 2. Quadrate lobe |
|
|
*** 1. Caudate lobe location 2. Quadrate lobe location > On diagram |
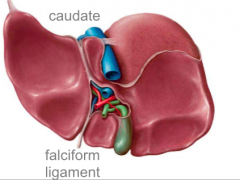
1. Division IVC and falciform ligament 2. Division body GB + falciform ligament |
|

Label *** (slide 101) |

|
|
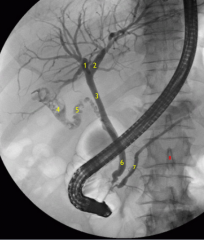
*** Label (slide 103) |
1: right hepatic duct 2: left hepatic duct 3: common bile duct 4: gallbladder 5: cystic duct 6: bile duct 7: main pancreatic duct 8: L1 |
|

Label *** Location of them |
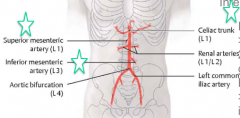
|
|
|
Describe the celiac trunk *** (slide 106) > diagram shown |
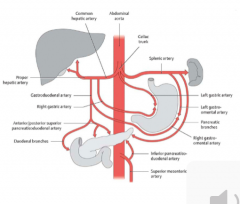
Supplied forgetu > left gastric artery = esophageal artery > splenic artery > common hepatic artery (liver, GB, part stomach, duodenum, pancreas) |
|
|
Position portal vein *** (slide 109) |
free end of lateral gastroduodenal ligament > part of lesser omentum |
|
|
Pringle's maneuver *** |
during surgery GB, if bleeding from liver/GB, just go into ligament, clamp off all blood (arterial, venous) supply to liver |
|
|
explain pancreatic/duodenal artery ** (slide 110) > on diagram |
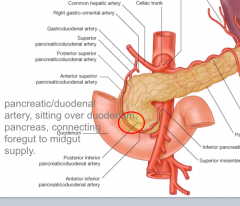
Branch of the common hepatic artery Supplies pancreas and duodenum Sitting over duodenum, pancreas Connecting foregut to midgut supply |
|
|
Explain SMA blood supply *** (slide 111) |
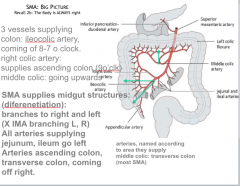
|
|
|
Ileocolic artery *? (slide 112) |
Supplies junction between ileum and colon |
|
|
IMA *** (slide 113, CS) > supply > common ischemic pts |
> descending colon (left colic artery) > sigmoid colon (sigmoid artery) > rectum (superior rectal artery) Common areas ischemia > Griffith's site = anastomoses between middle and left coeliac arteries > Sudek's site = anastomoses between sigmoidal and superior rectal arteries > region of bowel, left colic flexure prone ischemia |
|
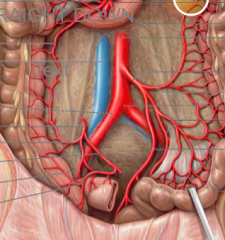
Label relevant parts IMA components ** (slide 114) |
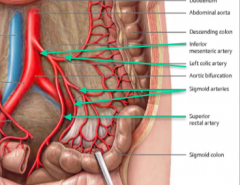
|
|
|
During surgery to remove a tumor in the uncinate process of the pancreas, the inferior pancreaticoduodenal artery is ligated. Which vessel will provide collateral circulation?*** (slide 115) a. right gastric artery b. right colic artery c. anterior superior pancreaticoduodenal artery d. gastroduodenal artery e. right gastroomental artery f. posterior superior pancreaticoduodenal artery f. |
gastroduodenal arter |
|
|
During surgery to repair a diverticulum in the sigmoid colon the IMA is ligated. Which vessel will provide collateral circulation to the descending colon? *** (slide 115) |
Middle colic artery |
|
|
Explain venous drainage GI tract *** (slide 116) |
GI > portal vein > liver > hepatic vein |
|
|
Explain the 5 sites of porto-cabal anastomoses *** |
Left gastric > esophageal veins paraumbilical > superior and inferior epigastric veins intestinal veins > retroperitoneal veins superior rectal > middle and inferior bare area liver > inferior phrenic |
|
|
*** 1. Backup of left gastric will go where? 2. Hemorrhoids 3. Paraumbilical vein backup to 4. intestinal veins backup to: 5. Bare area liver backup to: a. superior and inferior epigastric veins b.retroperitoneal veins c. inferior phrenic veins d. middle and inferior rectal veins e. esophageal veins |
1. esophagel veins 2. middle and inferior rectal veins (superior rectal vein > ) 3. superior and inferior epigastric veins 4. retroperitoneal veins 5. inferior phrenic vien |
|
|
Label *** (slide 118) |
red arrow: portal vein black arrow: IVC yellow arrow: 3 hepatic veins |
|
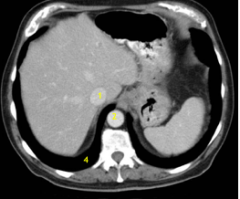
Label *** (slide 124) |
1: IVC 2: Aorta 4: Costodiaphragmatic recess |
|
|
Label *** (slide 124) |
a: blood stomach (expect black tarry stool) 3: spleen |
|
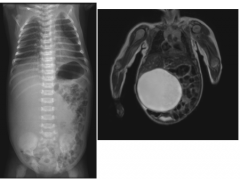
Explain *** (slide 126) |
congenital cyst |
|
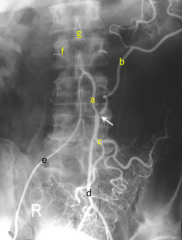
Label *** (slide 128) |
a: IMA b: left colic A c: sigmoidal A d: superior rectal A e: catheter f: pedicle g: spinous process |
|
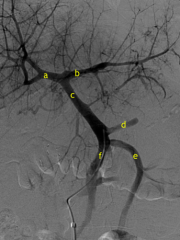
Label *** (slide 129) |
e: IMV f: SMV d: splenic vein c: portal vein a: right branch of portal vein b: left branch of portal vein |
|

label *** (slide 130) |
1: celiac trunk 2: splenic A 3: spleen 4: let gastric artery 5: common hepatic A 6: hepatic A proper 7: gastroduodnal A 8: duodenal/pancreatic A 9: right gastroomental A 11: catheter |
|
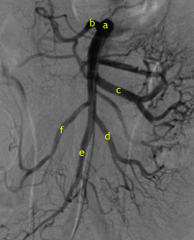
Label *** (slide 131) |
a: superior mesenteric A b: middle colic A c: jejunal A d: ileal A f: right colic A e: ileocolic A |
|
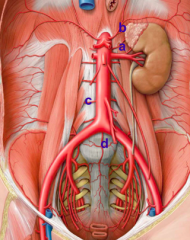
Label *** (slide 135) a-d label |
a: middle suprarenal A b: inferior phrenic A c: lumbar A d: middle sacral A |
|
|
Abdominal aorta, IVC span *** |
AA: T12-l4 IVC: T8-L5 |
|
|
IVC *** (slide 136) > spans > tributaries |
spans: T8-L5 Tributaries > right testicular vein > inferior phrenic veins > lumbar veins > right suprarenal veins (superior, middle, inferior) > renal veins > hepatic veins |
|
|
Explain suprarenal gland arterial venous supply > diagram shown (slide 153) *** |
Superior, middle, inferior suprarenal arteries to both > superior suprarenal A: inferior phrenic A > middle suprarenal A: abdominal A > inferior suprarenal A: renal arteries Venous drainage > right suprarenal directly IVC > left suprarenal to inferior phrenic |
|
|
*** 1. Where does the left suprarenal gland drain directly into? 2. Where does the right testicular venous drainage travel to? a. left renal vein b. SMV c. IMV d. inferior phrenic vein e. IVC |
1. inferior phrenic vein 2. IVC |
|
|
*** 1. Where does the left testicle venous drainage go to? 2. Where does right suprarenal gland venous drainage go to? a. left renal veinb. SMVc. IMVd. inferior phrenic veine. IVC |
1. left renal vein 2. IVC |
|
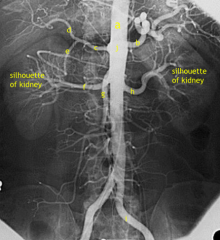
Label *** slide 158 |
a: abdominal aorta j: celiac trunk b: splenic A (tortuous) c: common hepatic A d: hepatic artery proper e: gastroduodenal artery f: right renal A h: left renal A g: SMA i: left common iliac A |
|
|
Suprarenal glands ** (slide 153) > dervation > innervation > venous drainage |
derivation > neural crest cell innervation > preganglionic sympathetic axons venous drainage > right suprarenal veins = directly into IVC > left suprarenal veins = into inferior phrenic vein (> IVC) Arterial supply > superior suprarenal A: inferior phrenic A > middle suprarenal A: aorta > middle suprarenal A: renal artery |
|
|
Innervaiton suprarenal glands* a. postganglionic sympathetic axons b. preganlgionic sympathetic axons c. lumbar sphlanics d. thoracic sphlanics e. pelvic sphlanics |
preganlgionic sympathetic axons |
|
|
*** 1. What is the arterial supply to the superior suprarenal gland? 2. What is the arterial supply to the inferior suprarenal gland? 3. What is the venous drainage of the left and right kidneys? 4. What is the arterial supply to the middle suprarenal gland? > Diagram shown |
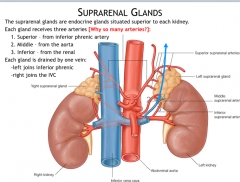
1. inferior phrenic A 2. renal A 3. LK = inferior phrenic vein, RK = IVC 4. Abdominal aorta |
|
|
*** 1. Venous drainage of left suprarenal gland directly 2. Right suprarenal gland venous drainage? a. left renal vein b. azygous vein c. right renal vein d. IVC e. inferior phrenic vein |
1. inferior phrenic vein 2. IVC |