![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
26 Cards in this Set
- Front
- Back
|
Relations of Liver |
- Right dome of diaphragm superiorly - Posteroinferiorly (visceral surface), location of gall bladder |
|
|
Lobes of the Liver |
1) Anatomically: Left, Right, caudate & quadrate 2) Functionally: Couinards classification of 8 different lobes. - Each has its own vascular inflow, outflow & biliary drainage |
|
|
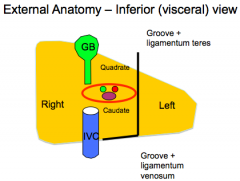
Anatomy of lier - visceral view |
|
|
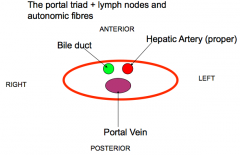
Porta Hepatitis |
|
|
Peritoneum |
- Small posterior bare area - Coronary ligaments (anterior & posterior) - Right & left triangular ligaments - Falciform ligament - Ventral mesentry - Lesser omentum (Arises from port hepatic & ligamentum venosum) |
|
|
Blood supply |
Coeliac trunk (25%)
Hepatic Portal System of Veins (75%) - Splenic & SMV meet posterion to head of pancreas to form portal vein. |
|
|
Cirrhosis |
- A consequence of chronic liver disease characterized by replacement of liver tissue by fibrosis, scar tissue & regenerative nodules (lumps) - This leads to loss of liver function |
|
|
Portal Hypertension |
Portal pressure gradient >10 mmHg
Normal portal pressure = 9 IVC = 2-5
--> Splenmegaly |
|
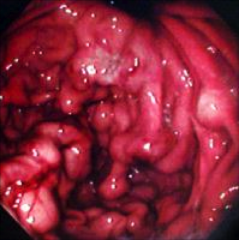
Oesophageal Varicies |
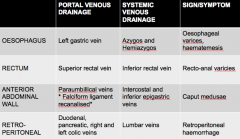
- Occur at the anastomoses of left gastric vein with esophageal veins at gastro-oesophhageal junction. - Present with haematemesis - Can be treated with gastric banding
|
|
|
Causes of Oesophageal Varicies |
- Peptic/GD ulcers - Tumours - Erosion of oesophagus - Gastroenteritis |
|
|
Ascites |
Fluid in Peritoneal Space
|
|
|
Causes of Ascites |
1) Portal hypertension 2) Hypoalbuminaemia 3) Aldosterone related renal sodium retention, with consequent blood volume expension - Further exacerbated by additional pressure on kidneys - ischaemia) |
|

|
Caput Medusae - Recanalised umbilical vein within the falciform ligament. - Paraumbilical veins radiate superiorly to intercostal veins and inferiorly to the inferior epigastric vein. |
|
|
Anorectal varices |
- Rectal varices NOT haemorrhoids - Form due to portal hypertension due to formation of portosystemic shunts. - May bleed massively - 53% of patients with portal hypertension & 78% of individuals with esophageal varicose have anorectal varicose |
|
|
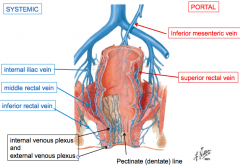
Veins of rectum and anal canal |
|
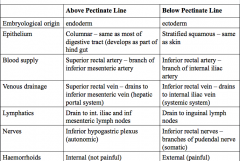
Recto-anal junction |
Recto-anal junction |
|
|
Porto-systemic anastomoses |
|
|
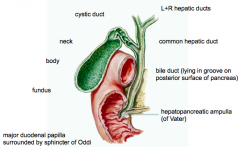
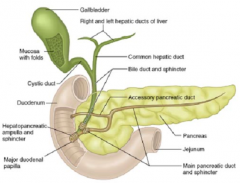
Biliary Tree |
|
|
Bile ducts of the liver |
- Bile secreted by the liver at a constant rate - 40ml/hour - Bile canaliculi drain into interlobular ducts - Form right (right lobe)& left (left, caudate and quadrate lobes) hepatic ducts at port hepatis - Ducts leave porta hepatic --> Common bile duct
|
|
|
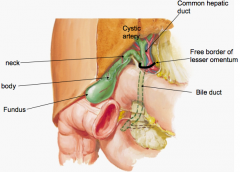
Free margin of lesser omentum |
Common hepatic duct - Lies in the free margin of the lesser momentum (4cm). It's joined on the right side by the cystic duct --> Form bile duct
Bile duct - Bile duct (8cm), in the free margin of lesser momentum, anterior to hepatic portal vein & right of the hepatic artery - Behind the duodenum (1st) - Lies in a groove on posterior head of pancreas, joined by pancreatic duct |
|
|
Gall Bladder |
- 50ml bile/day - Concentrates bile - Supplied by cystic artery (RHA) - Related to hepatic flexure of colon & duodenum - Inflamed gall bladder (cholecystitis) therefore herniates into these structure - Pain in the right upper quadrant, referred to right flank and right scapula |
|
|
Gall bladder and Extrahepatic ducts |
|
|
Pancreas and Gall bladder |
|
|
Gallstones in cystic duct |
Biliary colic (acute inflammation)- Acute cholecystitis -> Pain in right hypochondrium
NO JAUNDICE |
|
|
Gallstones in common bile duct |
Frequently but moderate jaundice |
|
|
Gallstones at the hepatopancreatic ampulla |
Jaundice & Pancreatitis |