Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
31 Cards in this Set
- Front
- Back
|
Abbreviations:
AA, ASA, CNS, COX, coxibs, NSAID, PG, PGI2, PNS, PUFA, TxA2 |
AA-arachidonic acid, ASA-acetylsalicylic acid (aspirin), CNS-central nervous system, COX-cyclooxygenase enzyme, NSAID-nonsteroidal antiinflammatory drug, PG-prostaglandin, PGI2-prostacyclin, PNS-peripheral nervous system, PUFA-polyunsaturated fat
|
|
|
Pain control drugs: narcotics, nonnarcotics, anticonvulsants, and antidepressants: which ones?
|
ONLY NARCOTICS ARE GOOD FOR ACUTE INJURY
Nonnarc: NSAIDs, salicylates, ibuprofen, naproxen, celecoxib Narcotic: opioids (morphine, codeine) Anticonvulsants: gabapentin Antidepressants:amitryptilene, duloxetine |
|
|
PUFA and AA and their relation? Formation of PG: how is it done? What does PG do?
|
Cell membranes have dietary PUFA in their bilayer: AA (AA eicosatetraenoic acid is major one (20c FA chain))
Stimuli free up the AA which is substrate for COX COX will transform AA into a PGH2 PG binds to receptors and provides cell signaling PGH2 is converted into other things needed for signaling via tissue specific isomerases |
|
|
What does an excess of PG in inflammed tissue do?
|
Part of inflammation is due to too many PGs
Without treatment, excess PG will cause eventual loss of function |
|
|
Cardinal signs of inflammation seen by PG
|
vasodilation, permeability, fever (temp), pain sensitization
|
|
|
Cyclooxygenase: how many are there and which ones?
|
COX 1 and COX2
|
|
|
COX1 and 2 Similarities: what are they?
|
Both use and make the same substrates (AA and PG respectively)
Both play an important role in inflammation Both have a physiological role in renal function |
|
|
COX1: expression and roles?
|
COX 1 is constitutive expression (expressed in all tissues at all times)
Plays a role in responding to physiological stimuli Also plays a role in responding to any pathological stimuli that release AA Contributes to forming PG |
|
|
Mechanism of COX 1 Action: what is it?
|
AA + COX1 + O2 = PGH2
PGH2 travels to tissues and via tissue specific isomerases becomes tissue specific PGs In uturus, helps during birthing. In gut, helps with mucosal integrity. In blood, helps with platelet aggregation, in blood platelets it stimulates activation of new platelets |
|
|
COX 2 and it's differences
|
Has a pathological function
COX2 must be induced by cytokines (induced in SOME tissues at SOME times)-inflammation induces it and so does cancer COX2 has a distinctive physiological role in kidney (complements role of COX1 in kidney) |
|
|
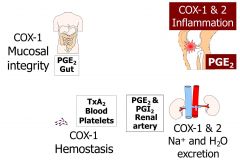
COX2 and COX1: roles in kidney
|
They are expressed together in the kidney.
Their combined actions will make PGH2 and via tissue specific isomerases will make PGE2, PGI2 in the renal artery to help with sodium and water excretion |
|
|
COX1 and 2 in inflammation
|
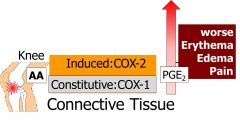
Inflammation stimulates AA release, COX 1 converts AA into PGE2 and PGE2 will cause symptoms.
With inflammation, COX2 expression will be induced and COX2 derived PGE2 will amplify symptoms |
|
|
NSAIDS: which drugs, traditional and nontrad?
|
Traditional NSAIDS: ibuprofex, naproxen, Indomethacin
Coxibs: Celecoxib Salicylates: Salicylate, Diflunisal, Aspirin Acetaminophen is only an ANALGESIC |
|
|
Mechanism of Action of NSAID
|
Anti-inflam, analgesic, and antipyretic actions of NSAID are though their inhibition of COX enzyme activity.
In doing this, they reduce PG formation and provide LOCAL reduction of edema, swelling, and pain sensitization |
|
|
Salicylates Traditional NSAIDs: what's their mechanism of action?
|

Competitive, Reversible, Nonselective
These drugs occupy the active site of COX1 and COX2 Not every NSAID can get into all COX: ibuprofen is able to bind the AA site on BOTH COX1 and COX2 |
|
|
tNSAIDs: length of action
|
Ibuprofen has a half life of 2 hrs
Naproxen has a half life of 14 hours |
|
|
NSAID AntiInflammatory Indictions
|
Osteoarthritis, bursitis, gout, ankylosing spondylitis, gout, dysmenorrhea, headaches
|
|
|
tNSAIDs: what are complications?
|
Ulcers, preipheral edema (due to reduced excretion of NA and H20), bleeding
These risks will increase with prolonged usage and as age increases |
|
|
COXIBS selective inhibition of COX2: how does it do it?
|
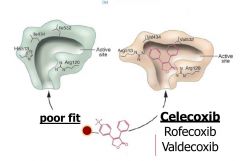
Competitive, Reversible, Selective
11 hr half life COXIBS don't fit well on the active site of COX1...They fit great on COX2: therefore, it will spare COX1 and select COX2 |
|
|
Selectivity and Issues with COXIBS in the kidney
|

Because COXIBS don't affect COX1 they are great at reducing inflammation while keeping all of the other side effects down.
However, due to their physiological function in the kidneys, there may still be an increase in peripheral edema and increase in BP due to reduced Na and H2O excretion Selectivity might not be as black and white in kidneys |
|
|
Hypersensitivity to Sulfonamindes (CELECOXIB): what's going on here?
|

Celecoxib (sulfonamide) can cause exfoliative dermatitis (SJS steven johnson syndrome) and toxic epidermal necrolysis (TEN) which could be fatal.
Celecoxibs have more tendency than other drugs to have this allergy Allergies to sulfa drugs can be indicative to an allergy to celecoxib This can occur without warning or prior sulfa allergies |
|
|
When not to use NSAIDS?
|
Never use with asthma
Never use with gut inflammation: gastritis, colitis, pancreatitis, hepatitis This is because gut healing relies on prostaglandins Also never use with infectious inflammation:meningitis, endocarditis, sepsis, bronchitis, sinusitis, rhinorrhea This is because fever is a mechanism of immunity and the fever is important to maintaining defense. |
|
|
Acetaminophen: how does it work?
|
It inhibits COX in the CNS allowing analgesia
Doesn't work to reduce inflammation |
|
|
COX1 and 2 functions in endothelial and platelet cells
|
Platelets have COX1 active, not COX2 because there is no nucleus (nno induction of COX2 and no regeneration of COX1). Decreased COX in platelets reduces TxA2 which is required for platelet aggregation
In endothelial cells, COX helps make PGI2 which is antithrobotic Aspirin is an irreversible inhibitor of COX!: in endothelial cells it will stop antithrombotic factors and in the platelets it will stop TxA2 from forming |
|
|
Irreversible COX inhibition via aspirin: what happens
|
Inhibition of COX via Aspirin will cause ceased production of thrombotic factors in endothelial cells and cause platelet cells not to release TxA2, req for platelet aggregation and activation.
This will persist DAYS after ASA metabolism and excretion Platelets can't regenerate COX |
|
|
Advantage of Low Dose Aspirin?
|
Low dose aspirin encounters every platelet through the presystemic circulation (liver).
This minimizes risk for toxicity, yet provides a great anti-thrombotic effect. This dosage of aspirin will not produce antiinflammatory effects |
|
|
Aspirin Metabolism: what happens to it?
|
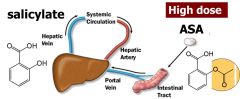
Extensively metabolized in the liver into SALICYLATE via deacetylation.
Salicylate systemically circulates Highdose ASA is a prodrug for anti-inflammatory doses of salicylate |
|
|
COX Independent Toxicities
|
Salicylates and Aspirin can cause: acid base disturbances, tinnitus, hypersensitivity, and reye's syndrome (rash, vomitting, liver failure): The disease causes fatty liver with minimal inflammation and severe encephalopathy (with swelling of the brain). The liver may become slightly enlarged and firm, and there is a change in the appearance of the kidneys. Jaundice is not usually present.
|
|
|
Aspirin Dosage and salicylate effect
|
Aspirin DOSE:
80-160 mg------------antiplatelet (aspirin effect) 325-1000 mg--------analgesic, antipyretic 325mg -6 grams----anti-inflamm/tinnitus 6-20 grams-----------early: Respiratory aklalosis; later-metabolic acidosis fever, dehydration More than 20g-----above plus, shock, coma |
|
|
Aspirin/Salicylate toxicity: what happens? (in cns particularly which causes a cascade)
|
Salicylates uncouple mitochondrial OX phosphorylation in CNS:
1. respiratory centers thinks reduced ATP production is from hypoxemia and responds by hyperventilation 2. hyperventilation blows off CO2 3. drop in CO2 causes respiratory alkalosis (which will prompt kidney to deplete bicarbonate) 4. Organic Acids accumulate b/c ATP isn't generating via Krebs Cycle 5. Metabolic Acidosis becomes life threatening |
|
|
Aspirin in children: when not to use?
|
Shouldn't use aspiring by anyone under 19 with a fever: like treating symptoms of flu like illnesses, chicken pox, cold because of risk of Reyes syndrome (marked by rash, vomitting, liver failure)
Use acetaminophen or ibuprofen for this. |