Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
53 Cards in this Set
- Front
- Back
|
Main classes of anti-fungal chemotherapies:
|
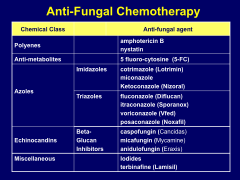
*polyenes
*anti-metabolites *azoles --> imidazoles and triazoles *echinocandins *miscellaneous |
|
|
Main components of the fungal cell:
|
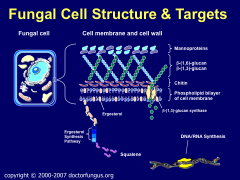
-Chitin, bilayer, ergosterol
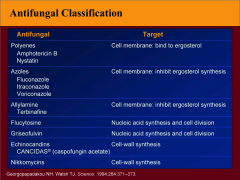
*w/i bi-layer, ergosterol is the tgt for the POLYENES *Ergosterol synthesis pathway is the tgt for the AZOLES. *ß-(1,3)-glucan is tgt of inhibitors *tgts are in cell wall and cytoplasm, not cell membrane |
|
|
Summary of Anti-fungals and their tgts:
|
|
|
|
What are the polyenes?
-general uses, locations, smell |
*Amphotericin B and Nystatin ; these are ANTI-BIOTICS
*Polyene macrolides produced by different strains of the gram-positive bacteria Streptomyces (of the group Actinobacteria or Actinomycetes). *Streptomycetes are found predominantly in soil and in decaying vegetation, and most produce spores *Streptomycetes are noted for their distinct "earthy" odor |
|
|
As far as route of administration, how do the polyenes differ?
|
Amphotericin B = Systemic
Nystatin = Topical |
|
|
4 formulations of Ampho B:
|
*Amphotericin B deoxycholate – Conventional (Amphocin®, Fungizone®)
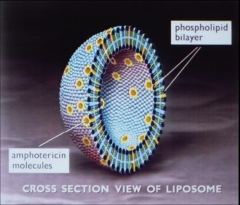
*Amphotericin B Colloidal Dispersion (ABCD; Amphocil™ or Amphotec™) *Amphotericin B Lipid Complex (ABLC; Abelcet™) *Liposomal Amphotericin B (L-AMB; Ambisome™) |
|
|
Unique chemical structure of polyenes that makes them work:
|
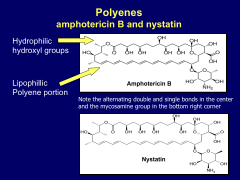
*both hydrophilic and hydrophobic portions in both ampho B and nystatin.
|
|
|
Why don't polyenes kill us humans?
|
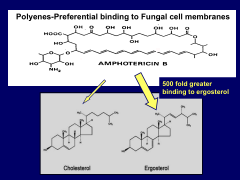
*preferentially bind to ergosterol, vice cholesterol
*500x binding to ergosterol |
|
|
Mechanism of Action of polyenes:
|
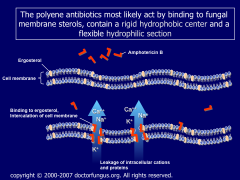
*Binds to membrane sterols, preferentially to the primary fungal cell membrane sterol, ergosterol
*Disrupts osmotic integrity of the fungal membrane by forming pores in the cell membrane thus resulting in leakage of intracellular potassium, magnesium, sugars, and metabolites leading to cellular death *The affinity for ergosterol (in fungal membranes) is 500 times greater than for cholesterol (in mammalian cell membranes) |
|
|
Antifungal spectrum of POLYENE effectiveness. 8
|
Candida albicans
Candida non-albicans Aspergillus spp. Cryptococcus neoformans Coccidioides immitis Histoplasma capsulatum Blastomyces dermatitidis Sporothrix schenckii |
|
|
What fungi will NOT respond to amphotericin B?
|
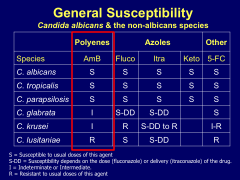
*C. lusitaniae.
*C. glabrata and C. krusei have intermediate susceptibility. |
|
|
Different dosing for different forms of ampho B?
|
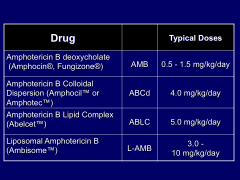
*Big, important differences.
|
|
|
Pharmacokinetics of Ampho B:
|
*Give slowly iv (2-4 hr); 0.5-1.5 mg/kg/day; with D5W
*Large volume of distro; Cmax 2 ug/mL; T1/2- 24 hr *Complex excretion: 5% excreted in urine unchanged; metabolites found in urine for up to 3 months *No change in dose with renal or hepatic dysfunction |
|
|
Toxicity of Ampho B:
|
*Most toxic antimicrobial in clinical use today
*Fever, N/V, anorexia, hypotension, electrolyte disturbances *Anaphylactoid reactions, phlebitis, bone marrow toxicity *Nephrotoxicity is a big concern. |
|
|
What are the major side effects of Ampho B?
How can you mitigate them? |
*Infuse over 2 to 6 hours, avoid rapid administration (hypotension, hypokalemia, arrhythmias, and shock can occur)
*Most commonly observed: -Nausea and vomiting, most common, usually occurring between 15 min to 3hrs following the dose -Infusion-related side effects are fever, chills & myalgia. Partially overcome by premedication with diphenhydramine and/or acetaminophen *Nephrotoxicity is the major adverse effect limiting use -The manifestations of nephrotoxicity are azotemia, decreased glomerular filtration, loss of urinary concentrating ability, renal loss of sodium and potassium, and renal tubular acidosis. |
|
|
Why are the newer formulations of Ampho B good?
|
*Amphotericin B traditional mainstay of antifungal therapy…but has changed..
*Its lipid formulations are promising due to their ability to reduce the toxicity of amphotericin B *Lipid formulations are currently licensed for use when amphotericin B therapy fails or is unacceptably toxic. The use of lipid formulations in specific clinical settings is under continuing investigation *All less nephrotoxic, more expensive, generally as effective as amphotericin B *Systemic toxicity is less with Abelcet & Liposomal amphotericin B *Primary indications - intolerance to amphotericin B and disseminated aspergillosis |
|
|
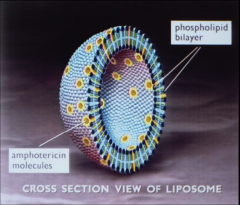
Liposomal Amphotericin B (AmBisome®)
|
|
|
LAMB Characteristics:
*how is it different than regular ampho B? |
*Incorporating AMB into a liposome alters the drug’s pharmacokinetic profile, but maintains its antifungal activity
*Lower volume of distribution and a reduced clearance than the conventional formulation -Dramatic increase in Cmax and AUC (Cmax of 83 vs. 1.1) *The liposomal formulation has a much larger therapeutic index, which allows for a higher dosage of AMB to be given *The effect of the dramatic increase in Cmax and AUC in the clinical setting is still debated |
|
|
Describe resistance issues in Ampho B:
|
*Resistance is rare either before or after treatment
*Usually due to decreased ergosterol levels in cell wall of fungi *May occur in strains of Candida spp. and Aspergillus spp. *Poor correlation between in vitro and in vivo results...means we don't always know what's going on. |
|
|
Discuss flucytosine (5-FC).
When/how is it used? dosing? |
*oral antifungal agent
*resistance develops rapidly *used mainly in combination with amphotericin B in the treatment of cryptococcal meningitis (25 mg/kg/day divided over four times daily) |
|
|
Discuss the MOA of flucytosine (5-FC):
|
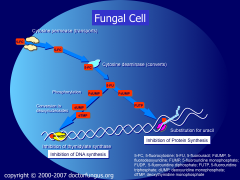
*Conversion to 5-FU (5-fluorouracil)
*In this form it inhibits DNA synthesis and PRO synthesis *Side effects are NVD b/c it kills good bacteria in the gut. |
|
|
5-fluoro-cytosine--PK:
|
*Available orally, 100% absorbed, inexpensive
*renally excreted, excellent CSF penetration (75% of blood levels *short T ½ - 3-4 hr, Cmax-25-50ug/ml (monitor blood levels) *Reduce dose with renal dysfunction |
|
|
5-fluoro-cytosine--toxicity:
|
*GI side effects, hepatotoxicity
*Major toxicity-Bone marrow suppression-especially when given with amphotericin B and other nephrotoxic drugs *Major limitation-rapid development of resistance in Candida, Cryptococcal infections [NEVER USE IN MONOTHERAPY] |
|
|
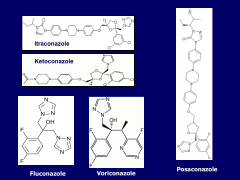
List the azoles:
|
Ketoconazole
Clotrimazole (Lotrimin®) Itraconazole (Sporanox®) Fluconazole (Diflucan®) Voriconazole (Vfend®) Posaconazole (Noxafil®) |
|
|
List the imidazoles.
List the triazoles. What's the structural ∆ b/t the two? |
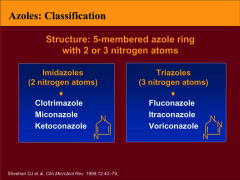
*2 N atoms vs. 3
*Fluconazole frequently Rxd b/c it works against Candida |
|
|
What kinds of things do azoles work vs?
What is resistant to them? |
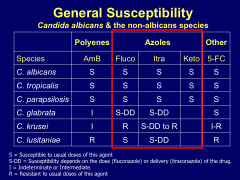
*Resistance to fluconazole in krusei
*glabrate is dose-dependent |
|
|
What is structurally significant about Itraconazole and Ketoconazole that affects their function?
|
-They are bases and must be in the presence of an acid iot be ionized to be active.
-A ppi will cause big problems with its effectiveness. -Take with apple sauce or Coke. |
|
|
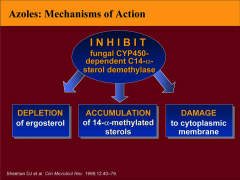
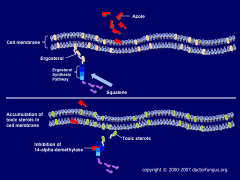
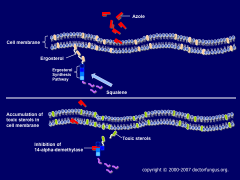
MOA of the Azoles:
|
|
|
|
What's the relative occurrence of different Candida species in pts?
|
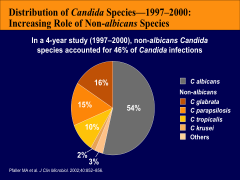
*About half albicans, half non-albicans
*Important to know, b/c some drugs don't work on krusei, etc. *Mostly see non-albicans in immunocompromised pts. |
|
|
Describe the effects of the azoles on the fungal cell membrane:
|
|
|
|
PK of the azoles:
|
*Available orally, limited V/D
*hepatically metabolized; low CSF levels; (except fluconazole) *long T ½ - 12-24 hr, requires gastric acidity for absorption *Reduce dose with hepatic dys. - or renal dysfunction (for fluconazole) |
|
|
Toxicity of the azoles:
-major drug interactions? |
*GI side effects (10%), hepatotoxicity (<1%), skin eruption (5%)
*Major drug interactions – hepatic Cytochrome p450 metabolized drugs (keto>itra>vori>fluconazole) *Inhibition of androgens, sterols *Voriconazole-reversible visual changes (30%); acute delirium (1%) |
|
|
Drug of choice for aspergillosis?
|
Voriconazole
|
|
|
Azole interactions in the GI tract:
|
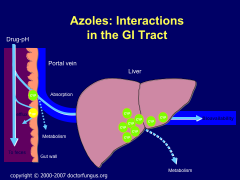
*esp. CYP3A4
|
|
|
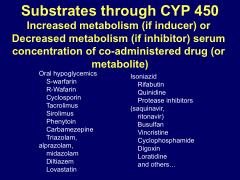
Azole inhibitors of CYP P450:
What general effect do they have? |
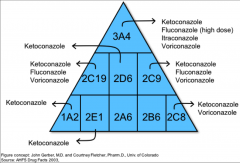
*Turns off metabolism; causes drug to build up.
*More toxicity; more drug-drug interactions. *Hard to predict the exact result in individual pts. |
|
|
Azole inducers of CYP P450:
What general effect do they have? |
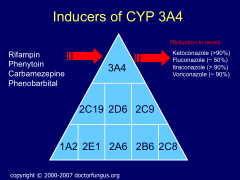
*Most important one is Rifampin (in TB pts, staph infections).
*Turns on metabolism; causes drug to be broken down more quickly; means you must dose higher. *VERY significant reductions in levels of azoles. |
|
|
List a shite-ton of drugs that may be affected by CYP 450 metabolism:
|
|
|
|
How do fungi become resistant to azoles?
|
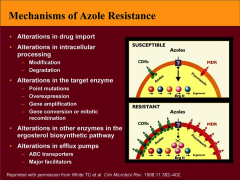
*efflux pumps -- MIC (minimum inhibitory concentration) increases slightly (slight resistance)
|
|
|
What sites on the fungal cell membrane are sites for resistance to azoles?
|
|
|
|
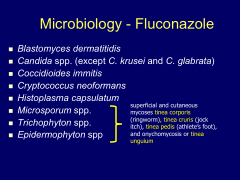
What all is Fluconazole effective against? What is it NOT effective vs?
|
|
|
|
What is Vorizonazole good vs?
What is its MOA? |
*works vs C. lusitaniae when AMB doesn't*
|
|
|
What are the Echinocandins? What do they inhibit?
|
Caspofungin (Cancidas®)
Mycofungin (Mycamine®) Anidulafungin (Eraxis®) *Beta-glucan inhibitors |
|
|
Where in the fungal cell membrane do echinocandins work?
|

|
|
|
What is Caspofungin effective vs?
Dosing? Effect on P450? |
*Activity against most species of Aspergillus and Candida
*Use: Aspergillosis in amphotericin intolerant patients (and itraconazole failures) well tolerated in early clinical trials – Dose 70mg loading: 50mg IV/day, disseminated candidiasis (as effective as Amphotericin B – less toxic). *Minimal renal excretion; modest hepatic metabolism and excretion (decrease dose with moderate-severe liver disease). *No effect on cytochrome P 450 system. |
|
|
PK summary of Echinocandins:
|
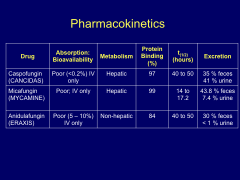
*IV only
*Anidulafungin in pts with bad livers. *Urinary excretion can be a concern in UTI pts. |
|
|
What all do Caspofungins work vs?
|
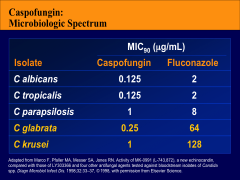
*Shows fluconazole doesn't work vs glabrata and krusei; but Caspofungins do.
|
|
|
Indications for caspofungin Rx:
|
*Micafungin and Anidulafungin now available-for candidiasis
*Caspofungin: Candidiasis and invasive aspergillosis *PK/PD: iv only, hepatic excretion, no effect on cytochrome P450 enzymes, dose at 70 mg loading and 50 mg iv daily |
|
|
Adverse reactions and drug reactions for caspofungins:
|
*Decrease dose for severe liver disease (35mg/day)
*Side effects allergy (rare), drug interactions with cyclosporin A *Rifampin increases hepatic excretion- increase dose to 70 mg/day; consider increasing dose for other enzyme inducers-efavirenz, nevirapine, phenytoin, dexamethasone |
|
|
How does the SE profile of the caspofungins compare to that of AMB?
|
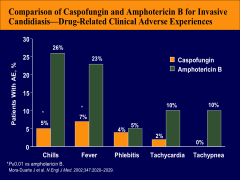
*caspofungin is similar to all the other Echinocandins in its SEs.
|
|
|
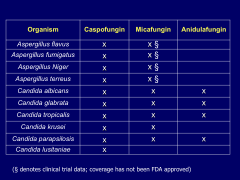
Summary of all the echinocandins' effectiveness against species of both aspergillus and candida:
|
|
|
|
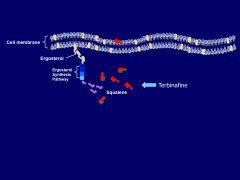
Discuss Terbinafine:
-how does it work -metabolism -indication? |
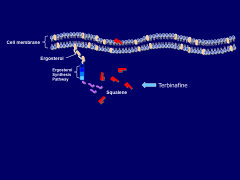
*Lamisil
*Allylamine- inhibits egrosterol synthesis at squalene epioxidase *hepatically metabolized by not CYP450 dependent; Long T ½ -24-36 hr, orally adminisitered at 250 mg/day *Primary indication: onychomycosis-12 wk- toes-6 wk fingers |
|
|
Discuss Iodines in antifungal therapy:
indications SE profile |
*SSKI-still used for lymphocutaneous forms of sporotrichosis
*Side effects-bronchorrhea, drooling, acne, thyroid disturbances *Start with 1 cc in Juice TID-increase to 4 cc TID as tolerated *Itraconazole has largely replaced SSKI-remains inexpensive alternative |
|
|
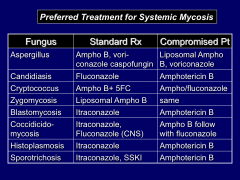
Breakdown of Preferred treatments for Systemic Mycosis by fungus type in Standard and Compromised Pts:
|
|