Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
467 Cards in this Set
- Front
- Back
|
What should be considered for the renal patient, what stage of CKD do you need a nephro consideration?
|
CKD 3 or higher
pg 4 |
|
|
If pt has CKD 3 or higher what VAD is recommended?
|
IJ
|
|
|
Do you avoid placing a VAD on ipislateral side of a AVF?
|
Yes
|
|
|
When is the exception that a VAD can be placed on the same side of a AVF?
|
Hospice patient but always discuss with the nephrologist.
|
|
|
What should be considered for the renal patient, what stage of CKD do you need a nephro consideration?
|
CKD 3 or higher
pg 4 |
|
|
If pt has CKD 3 or higher what VAD is recommended?
|
IJ
|
|
|
Do you avoid placing a VAD on ipislateral side of a AVF?
|
Yes
|
|
|
When is the exception that a VAD can be placed on the same side of a AVF?
|
Hospice patient but always discuss with the nephrologist.
|
|
|
In the presence of a pacemaker or automatic intracardiac difibrillator (AICD), avoid PICC insertion on ipsilateral side for at least how long?
|
6 months
p6 |
|
|
When do you avoid placing a VAD in a pedi?
|
Avoid CVAD and PVAD insertion in lower extremities of crawling or ambulating patient.
|
|
|
Power injectable devices are made of polyurethane and engineered to withstand high pressures. What pressure can these devices withstand?
|
>300 pounds per square inch PSI
|
|
|
What is placed thru a power injectable device?
|
IV contrast during a CT (computerized tomography) or MRI (magnetic resonance imaging)
|
|
|
What is a PVAD?
|
Perpherally Vascular Access Device (MLC and PIV)
|
|
|
What is a CVAD?
|
Central Venous Access Device (PICC, IVAD's, non-tunneled and tunneled central catheters)
|
|
|
What is a IVAD?
|
Implanted (subcutaneous) Venous Access Catheter
|
|
|
When would PiCCs with antimicrobial properties be beneficial?
|
MAY be beneficial with patients with probable septicemia and neutropenia.
|
|
|
For Chemotherapy administration:
When is PICCs the device of choice |
When the duration is unknown
Short term <3 months |
|
|
For Chemotherapy administration:
When is a IVAD the device of choice? |
For complex chemo protocols
*infusion therapy > 3 months *intermittent and continuous infusion chemo |
|
|
For Chemotherapy administration:
When is a Tunneled CVAD the device of choice? |
Patients with acute leukemia and other blood ca and pts undergoing blood and marrow transplants.
|
|
|
What type of VAD in most frequently used in peds?
|
Tunneled CVADs p6
IVADs are used less due to size, pt fear of needle access and potential dislodgemt of needle with activity. |
|
|
TPN:(p8)
What VADs can be used for yrs in home health settings or alternative care settings? |
IVADs and tunneled VAD
|
|
|
TPN:p8
If TPN is given thru a multilumen VAD what should be considered? |
Consider ad dedicated lumen for TPN infusion.
|
|
|
Chemotherapy: p7
Should chemo be interupted? why? |
No.
Increased risk of exposure to hazardous materials to pt and clinician. |
|
|
Frequent Blood transfusions: p8
What would be the device of choice? |
IVAD
ex sickle cell |
|
|
Give an ex. of when intravenous meds that require reliable venous access for daily or continuous infusion?
|
Specific meds such as remodulin, prostacylin or flolan for pulmonary hypertension. These would be continuous infusions. p9
|
|
|
For continuous or daily infusions, what is the VAD of choice?
|
Single lumen tunneled CVAD is usually the choice.
PICC may be considered as a bridge. p9 |
|
|
For plasmapheresis and stem cell collections what type of VAD is used? What are the required flow in ml/minute?
|
Large bore catheter.
90 to 120 ml/minute |
|
|
What are the flow rates for a hemodialysis catheter?
|
350-400 ml/minute p10
|
|
|
How long after a lymph node is removed can lymphedema occur?
|
can occur yrs or decades after original lymph node dissection surgery. p11
|
|
|
If the pt has the inability to tolerate a pneumothorax, what VAD is contraindicated?
|
Subclavian CVAD insertion p12
|
|
|
Which patients would have the inability to tolerate a pneumothorax?
|
Existing pneumo
COPD pts who could decompensate bullous lung disease Bullous emphysema is one or more thin-walled, air-containing spaces, conflated by ruptured pulmonary alveoli. These air-containing spaces are termed as "bulla" (pl. bullae), which is a thin-walled air sacs in the lung tissue, more than 1cm, and filled with air with a tendency to burst. emphysema in which bullae form in areas of lung tissue so that these areas do not contribute to respiration |
|
|
What are some of considerations .when placing a VAD in a morbid obese patient?
|
* Requires US guidance and experience
*Consider potential sites in terms of ability to maintain a dry and intact dressing and ability to stabilize the CVAD *for a picc the cephalic vein may be most appropriate due to moist insertion site or dislodgement p13 |
|
|
What are the risks of placing a CVD on the ipsilateral side of a AICD (Automatic Implantable Cardioverter Defibrillator)?
|
*More recently placed the greater the risk of lead dislodgement
* risk of occlusion of the subclavin |
|
|
Which CVDs are contraindicated for sepsis/bacteremia?
|
Tunneled CVDs
Acute CVDs without antimicrobial protection Picc without antimicrobial protection |
|
|
What are the considerations for a patient with Reynauds Syndrome or peripheral vascular disease?
|
Pt is at increased risk of catheter related thrombosis due to compromised circulation
Use the smallest gauge to accomplish the therapeutic goal. |
|
|
if on evaluation of site determination it is noted that there is prominent superficial vein in the area of planned CVAD, what may that indicate?
|
Neighboring or central vein stenosis or thrombosis.
|
|
|
Avoid non-compressible or partially compressible target veins, why?
|
these veins may denote probable thrombosis.
|
|
|
Measuring by anatomical landmarks:
How do you measure for a PICC placed in the arm? |
1.position the arm 90 degrees from the body
2. measure from the planned insertion site to the right clavicular head 3.then down to the 3rd intercostal space. p17 |
|
|
Studies using landmark-based methods have reported failure rates and complication rates as high as what %?
|
Failure rates: 30%
Complication rates: 18.8% p17 |
|
|
Measuring by anatomical landmarks:
How do you measure for a PICC placed in the scalp? |
1. Identify planned insertion site
2. Measure from insertion site, along the jugular vein 3. to the right clavicular head and then to the 3rd intercostal space. p17 |
|
|
Measuring by anatomical landmarks:
How do you measure for a PICC placed in the lower extremity? |
1. Identify planned insertion site
2. Measure from the insertion site up the leg towards the umbilicus 3. to the xyphoid process p17 |
|
|
Measuring by anatomical landmarks:
How do you measure for a non-tunneled percutaneous catheters? |
1. Measure from the intended insertion site
2. Along the intended venous course 3. to the 3rd intercostal space 4. Along side the right side of the sternal border. p17 |
|
|
What is the function of the skin?
|
1. barrier against microorganisms
2. provides sensory regulation 3 provides temperature regulation |
|
|
What are the layers of the skin?
|

epidermis and dermis
|
|
|
Skin ranges in thickness
What is the thickness of the eyelids? heels/palms? average of most of the body? |
eyelids: 0.5mm
palms/heels: 4mm average of most of the body: 1-2mm |
|
|
What is the epidermis composed of?
|
Forms the protective covering. It is composed of epithhelial tissue.
|
|
|
What is the dermis composed of ?
|
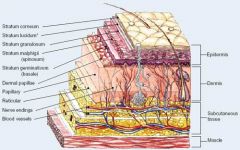
Composed of connective tissue
Highly sensitive and vascular...contains capillaries and nerve endings. |
|
|
What is composed of the superficial fascia or subcutaneous areolar/tissue connective tissue?
|
Adipose tissue, the superficial veins used for peripheral venipunctures are located in this layer.
|
|
|
Explain the systemic circulation on the venous side.
|
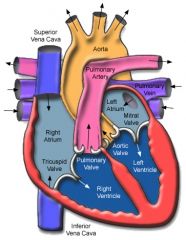
*Transports deoxygentated blood from the tissues back to the right side of the heart.
*located superficial and deep *thinner walls *collapsible and distendable |
|
|
Explain the systemic circulation on the arterial side
|
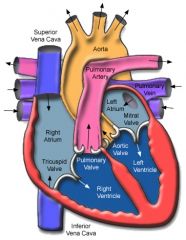
*Transport oxygenated blood from the left heart to the organs and tissues.
*Thicker walls *Elastic tissue in walls: maintains pressure during diastole to maintain forward movemt of blood *Generally located deep *Rapid flow rates compared to venous. |
|
|
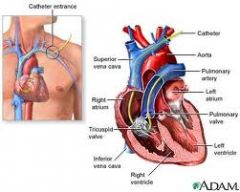
Explain the function of the pulmonary veins.
|
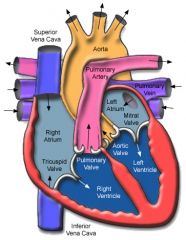
Pulmonary vein transport the oxygenated blood to the left side of the heart. (atrium)
|
|
|
Explain the function of the pulmonary arteries.
|
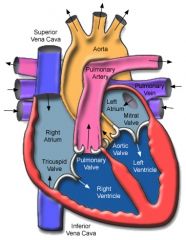
Pulmonary arteries transports unoxygenated blood from right ventricle to the pulmonary capillary bed for oxygen and carbon dioxide exchange.
|
|
|
What are the 3 layers of the vein?
|
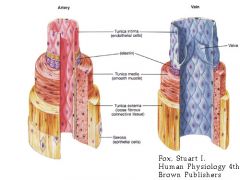
Tunica adventitia
Tunica media Tunica intima (endothelium) |
|
|
What is the tunica adventitia?
|
Vein: Outermost layer, Connective tissue, supportive layer
Artery: Outermost layer, thicker layer of connective tissue compared with veins |
|
|
What is the tunica media?
|
Vein: Middle layer
Composed of smooth muscle and elastic tissues Contains nerve fibers for vasoconstriction and vasodilation. Collapsible/distensible Artery: Middle layer Composed of more layers of smooth muscle and elastic tissues & more rigid compared to veins. Tend not to collapse Regulates blood flow Vasoconstricts with pain and anxiety. |
|
|
What is the tunica intima or endothelium?
|
Vein: Inner most layer
* Single layer of smooth muscle, flat endothelial cells, lining all bl vessels, including veins, arteries, heart and valves & capillaries. *Non-thrombogenic *Damage to this layer exposes underlying collagen layer & initiates activation of plt to create a plt. plug and activates clotting cascade to deposit fibrin in the plt plug. *Damage to this layer also allows fluid to leak across the vessel wall due to hydrostatic pressure as seen in infiltrates. Artery: innermost layer *Single layer of smooth flat endothelial cells, lining all bl vessels *Non-thrombogenic *Damage to this layer can cause thrombus formation; loosening of a large thrombus can cause significant embolic events...stroke, pulmonary embolus or other end organ or to the periphery |
|
|
Explan the basilic.
|
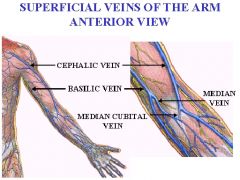
Basilic vein continues up the medial side of the arm, across the antecubital fossa, traversing up the medial side of the upper arm terminating where it joins the brachial veins to become the axillary vein
|
|
|
What is the vein of choice for PICCs or midlines?
|
Basilic
|
|
|
Explain the route of the brachial vein.
|
Orginates in the antecubital fossa, traverse up the middle of the arm along with the brachial artery.
|
|
|
Why use caution when using the brachial vein on pediatrics?
|
PICC insertion in young or nonverbal pts do not have the ability to verbalize symptoms of nerve injury which includes pain or numbness.
|
|
|
What does medial mean?
|
Relating to, situated in, or extending toward the middle; median.
|
|
|
What does dorsal mean?
|
toward, on, in, or near the back or upper surface of an organ,
|
|
|
Explain the route of the axillary vein
|
Begins at the junction of the basilic and brachial veins, transverses through the shoulder and terminates at the lateral border of the first rib.
|
|
|
Is the axillary vein easy to access?
When would this be accessed? |
Easy to access with ultrasound guidance.
Used for CVAD when trying to avoid the risk of pneumothorax or arterial puncture. p21 |
|
|
When should the axillary vein not be used?
|
Should not be used for CVAD in pts with CKD or ESRD unless cleared with a nephrologist.
|
|
|
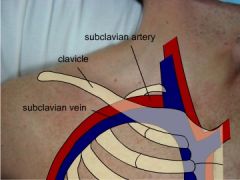
Explain the route of the subclavian vein.
|
Subclavian vein is a continuation of the axillary vein and runs from the outer border of the first rib to the medial border of anterior scalene muscle.
Joins with the internal jugular vein to form the brachiocephalic vein (innominate vein) p22 |
|
|
CVAD insertion into the subclavian increases the risk for what?
|
Risks include pneumothorax, hemothorax, subclavin arterial puncture and catheter pinch-off. p22
|
|
|
When should a subclavian not be placed?
|
Subclavian should NOT be placed in patients with CKD stage 3 or higher or ESRD unless cleared by a nephrologist.
|
|
|
What does IHI recommend the subclavian or the IJ?
|
Subclavian approach over the IJ site for lower CLABSI, intraclavicular sites have lower bioburden compared with the neck sites.
Bioburden: # of bacteria living on a surface before it is sterilized. |
|
|
Explain the route of the brachiocephalic on the left and right?
|
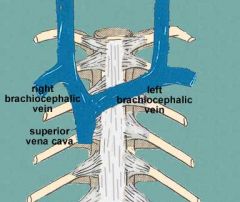
Each is formed at the root of the neck by union of the ipsilateral internal jugular and subclavian veins.
|
|
|
A catheter tip terminating in the brachiocephalic has a higher risk of what?
|
High risk of causing venous thrombosis.
|
|
|
Describe the route of the left brachiocephalic vein?
|
Left brachiocephalic vein is longer compared with the right brachiocephalic and enters the SVC at a near 90 degree angle.
|
|
|
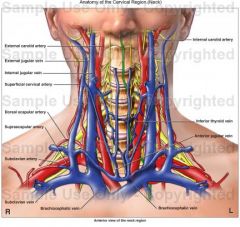
What is the largest vein in the neck?
|
internal jugular
|
|
|
What site is recommended for the tunneled CVADS and ports?
|
IJ p23
|
|
|
What type of insertion runs the risk for pinch off ?
|
subclavin, piccs
|
|
|
Vein of choice for short term dialysis catheters?
|
Vein of choice for insertion of dialysis short term CVAD as it avoids problems of stenosis that could impede creation of AVF on the ipsilateral side. p23
|
|
|
Explain the route of the external jugular
|
Superficial vein that originates near the angle of the mandible and courses over the sternocleidomastoid muscle. Ej dives into the subcutaneous tissue eventually emptying into the subclavian vein.
**Not used for venous access. |
|
|
When is an external jugular accessed (3)?
|
*It is superficial accessed for emergent and very short IV access.
*When can't get another access, and large amts of fluid needs to be given. |
|
|
What size IV catheter can the EJ accommodate?
|
18g or larger
|
|
|
When an IV is placed in the EJ, what is at risk?
|
thrombosis
extravasation |
|
|
What is the largest vein in the upper body?
|
SVC
|
|
|
What is the flow rates in the SVC?
|
2 L per minute
|
|
|
CVADs placed in the hepatic or thoracic veins or in the lower extremities should have their catheter tips located where?
|
In the inferior vena cava above the level of the diaphragm.
|
|
|
IVC may be accessed directly thru which approach?
|
Via translumbar approach
|
|
|
IVC may be accessed indirectly thru which approach?
|
Via common fermoral veins or hepatic vein (transhepatic approach) p25
|
|
|
When is the femoral site used for CVAD access?
|
When used for short term access.
In pts with severe coagulopathy or profound resp failure, at risk for hemothorax or pneumo When there are contradictions for placing a device in the neck or chest. |
|
|
How do you located the femoral for access?
|
Lies within the femoral triangle in the inguinal-femoral area.
Surface anatomy is identified for venipuncture by palpating the point of maximal pulsation of the femoral artery immediately below the level of the inguinal ligament and marking a pt approximately 0.5cm medial to this pulsation. |
|
|
Disadvantage to the femoral site?
|
It presents a field that is potentially contaminated because of the proximity of the perineal area.
|
|
|
Where is the hepatic vein located?
|
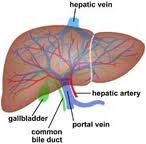
Near the liver and drains into the inferior vena cava
|
|
|
What vein is typically accessed for a transhepatic access?
|
Middle hepatic vein
|
|
|
When is a transhepatic access done?
|
Is an alternative approach into the IVC. it can be used in the setting of SVC occlusion and in pts with infrarenal vena cava occlusion.
Catheter tip terminated in the IVC. |
|
|
Describe the path of the posterior auricular vein.
|
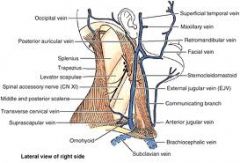
Superficial vein on side of head. Descends behind the ear to join the posterior section of the temporal maxillary vein into the external jugular
|
|
|
What vein is located behind the ear and the pathway is tortuous?
|
Posterior auricular
|
|
|
Describe the pathway of the azygos vein.
|
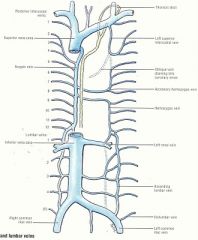
Azygos vein ascends from the abdomen and arches anteriorly to enter posterior wall of the SVC
|
|
|
When would the azygos vein enlarge?
|
Enlarges in the setting of SVC occlusion or stenosis.
|
|
|
If a catheter tip is in the azygos, what needs to happen?
|
Catheter must be repositioned or replaced.
**When left in a collateral vein for access, be cognizant of potential complications of occlusion of a dominant collateral, leading to venous outflow obstruction. |
|
|
Can the azygos be used to access for CVC placement?
|
While not typically used for CVC tip placements, azygos offers an alternative before other sites (such as direct IVC placement) are entertained.
|
|
|
Describe the pathway of the saphenous vein.
|
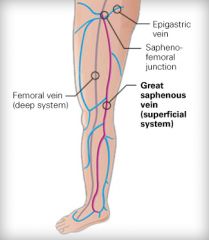
Begins at the inner side at the arch on the dorsum of the foot, ascends along the inner side of the leg and behind the knee. This vein terminates into the femoral vein.
|
|
|
What vein can be palpated or visualized above the ankle?
|
Saphenous
|
|
|
What are 2 considerations for lower-extremity CVC?
|
*Do not insert a lower extremity CVC in a crawling or ambulatory patient
* Numerous valves in the legs may cause threading difficulties. |
|
|
Describe the route of the popliteal vein.
|
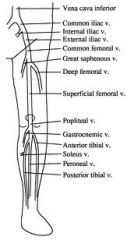
Formed by the junction of the anterior and posterior tibial vessels, ascends thru the popliteal space where it becomes the femoral vein p 27
* Can be palpated or visualized by the knee. |
|
|
Can the umbilical vein be used to place a CVC?
|

Yes.
|
|
|
How long is the umbilical vein available to place a CVC?
|
Patent vein in the umbilical cord available for up to 1 week post birth for vascular access.
|
|
|
Where is the catheter tip located after inserting into the umbilical vein for CVC placement?
|
catheter tip is placed above the level of the diaphragm for all types of infusates and CVC monitoring.
|
|
|
Can you use a single or dual lumen catheter for umbilical access?
|
Can use either
|
|
|
How to find a choice of arterial access?
|
Choice of artery is dependent on the ability to palpate a pulse or to locate it by Doppler flow or ultrasound guidance.
|
|
|
Which artery is the most popular site for an art line?
|

Radial
|
|
|
Describe the path of the radial artery
|
Begins at the bifurcation of the brachial artery, just below the bend of the elbow and pases along the radial side of the forearm to the wrist.
|
|
|
What are the 3 arteries used for art lines?
|
Radial
Femoral Brachial |
|
|
Where do you access for a brachial art line?
|
Several cms above the antecubital fossa, cannulation of the brachial artery may require ultrasound guidance as it courses deeper up the arm.
|
|
|
For peds: the patient will usually have piccs inserted in a procedure room, why?
|
To avoid violation of the "safe haven" of patients room p 29
|
|
|
What should be considered when placing a CVAD in a peds pt? (5)
|
1.Sedation: anxiolytics and mild, moderate and deep sedation
2. Anesthetics (topical, oral, IV) 3. Child life specialist involvement 4 Parental presence should be considered for planned PICC insertions. 5. Consider coordinating any CVAD insertion with other planned procedures |
|
|
What are considerations to look at prior to placing a CVAD in an infant?
|
1. consider sucrose water to decrease pain
2. for infants and toddlers, use of heel warmers may help to dilate the veins p30 |
|
|
What position is appropriate for CVAD placement?
|

Supine or trendelenberg
|
|
|
For the infant what is an effective way to position in order to get the cvad in?
|
For the young infant, bundling is an effective way to minimize movement and provide comfort. p30
|
|
|
What does the maximal sterile barrier precautions include?
|
cap
mask sterile gown sterile gloves large sterile drape (total body drape) Masks on all personnel in the room |
|
|
What is the difference between patient verification confirmation and time out?
|
Time out:
verbally confirm name and DOB or/and MRN and site Pt verification: Have pt state name and DOB or/and verify armband for correct name and MRN with other documentation. p31 |
|
|
What is the proper skin antisepsis used for CVAD excluding the femoral? And how is it used?
|
>0.5% Chlorhexidine with alcohol p40
Friction on the skin for 30 seconds and allowed to dry |
|
|
How long should the chlorhexidine be applied for a femoral site?
|
Should be applied for at least 2 full minutes using friction and allowed to dry. p31
|
|
|
The used of chlorhexidine as a skin antiseptic is not recommended for pts under what age?
|
under 2 months of age
|
|
|
Catheter is secured to the skin by what 3
methods? |
suture
staples securement device p32 |
|
|
What are the 4 ways to verify catheter tip position?
|
CXR
fluoroscopy (live xray) intravascular ECG intravascular doppler flow: method to determine blood flow velocity |
|
|
Peds:
Where is the optimal tip location for CVADs inserted in the upper chest or extremity? |
lower 1/3 of SVC or cavo-atrial junction
p33 |
|
|
Peds:
Where is the optimal tip location for CVADs placed in the IVC? |
diaphragm and the right atrium
|
|
|
Dialysis CVADs: where is the tip located in the short-term cuffed dialysis CVC vs the long term cuffed dialysis CVC?
|
Short term: distal SVC/right atrial junction
Long term: right atrium |
|
|
Where is the tip of the femoral dialysis CVC located?
|
IVC
p34 |
|
|
Hemodialysis requires high flow rates, what is that rate?
|
Usually >350ml/min
|
|
|
What is the difference between a seldinger technique vs the modified seldinger technique?
|
Seldinger involves accessing a vein or artery with a small needle introducing a flexible guidewire removing the needle and advancing the catheter over the wire.
Modified ST: accessing a vein with a small needle (21 or 22 g) into which a guidewire is advanced the needle removed and an introducer/dilator is advanced, the catheter is advanced thru the introducer. |
|
|
Catheter tip malposition accounts for what % if CVC complications?
|
3%
|
|
|
Repositioning is indicated for CVC tips outside of the ca junc or distal svc, excluding dialysis cvads. explain how thru flushing?
|
tips may be repositioned by rapidly flushing with 20 ml of normal saline using a 10ml syringe or larger.
|
|
|
How should the patient be positioned to promote optimal tip location when malpositioned in the internal jugular?
|
HOB 45 to 90 degrees
Flush if real time ultrasound available visualize catheter in the vein to determine success of flush intervention using transverse and longitudinal views p38 |
|
|
How should the patient be positioned to promote optimal tip location when malpositioned in the contralateral subclavian vein?
|
Ipsilateral position, HOB elevated, Flush.
EX: catheter placement on the right, tip in the left subclavian, position patient on the right side. |
|
|
How should the patient be positioned to promote optimal tip location when malpositioned in the axillary vein?
|
Contralateral position, HOB elevated, flush
EX: catheter placement on the right, tip in the right axilla, position pt on the left side |
|
|
How should the patient be positioned to promote optimal tip location when malpositioned in the azygous vein?
|
Position of comfort with HOB 30 degrees...flush
|
|
|
If the CVAD is in the RA, what action is taken to correct placement?
|
retraction per doctors order.
|
|
|
What are the adult and pediatric heparin dosages for heparin locking a catheter?
|
10-1000u/ml for adults
1-10 u/ml for peds |
|
|
What dressing type is recommended to protect the insertion site of a CVAD?.
|
Transparent, semi-permeable (TSM) polyurethane dressing
TSM dressings allow direct visualization of the insertion site and allows natural moisture produced by skin to wick away p40 |
|
|
How often do gauze dressings get changed?
|
Every 2 days
|
|
|
If allergic to chlorhexidine, what is an alternative?
|
1% or 2 % iodine, iodophors and isopropyl alcohol
|
|
|
If institutional rates of CLABSI are higher than institutional goals consider what?
|
Chlorhexidine impregnated foam disc.
which is changed with each dressing change or if visibly soiled |
|
|
What is the only thrombolytic agent approved by the FDA?
|
Alteplase produced by Genentech Inc.
|
|
|
When is an antibiotic lock recommended?
|
Indicated for pts with long-term catheters and diagnosis of CRBSI with no signs of exit site or tunneled infection and for whom catheter salvage is the goal.
|
|
|
How is the antibiotic lock instilled and explain what is instilled?
|
Instill supra-therapeutic dose of an antibiotic, to which the causative microbe is susceptible, in the catheter lumen and allow dwell of hr or days. Usually given in conjunction with systemic antibiotics. p 42
|
|
|
Which microbe is most likely to respond to an antibiotic lock and which 2 microbes are not likely to respond?
|
Coagulase negative staphylococci most likely to respond
and S aureus and Candida are not p42 |
|
|
Which is harder to kill thru antibiotic lock, a sessile or planktonic bacteria?
|
Sessile bacteria
Sessile:fixed in one place; immobile |
|
|
What concentration does the antibiotic for an antibiotic lock need to be in order to kill sessile bacteria?
|
antibiotic conentrations need to be 100 to 1000 times greater to kill sessile bacteria
|
|
|
Catheter removal recommended for CRBSI for what 2 types of bacteria?
|
S aureus and Candida species
|
|
|
What constitutes an antimicrobial catheter?
|
Use of chlorahexadine/silver sulfadiazine
or minocycline/rifampin impregnanted CVCs |
|
|
When would an antimicrobial catheter be used?
|
In a pt whose catheter is expected to remain in place for greater than 5 days if CLABSI rates are not decreasing after successful implementation of a comprehensive strategy to reduce infection rates.
p43 Comp strategy: 1 educating persons who insert and maintain the lines 2 use of maximal sterile barrier precautions 3 used of 0.5% chlorahexadine with alcohol |
|
|
What is the primary risk of catheter removal?
|
air embolism
|
|
|
What is the removal procedure of a central catheter?
|
1 place pt in a flat or trendelenburg position.
2 pt should execute valsalva maneuver during which catheter is removed gently and swiftly. * if pt is on a respirator catheter removal should occur at maximum inhalation and removed quickly. 3 quickly place 4x4 gauze pad over the site while applying continuous pressure 4. apply antiseptic ointment at the sited and cover with dressing for at least 24 hrs. p44 |
|
|
Is it necessary to place the pt in a supine or trendelenburg position to remove a PICC?
|
No, since the PICC is in a peripheral vein.
|
|
|
What is placed over the site on a PICC that has been removed?
|
1 antiseptic ointment and sterile gauze over the site with continuous pressure
2 leave on for at least 24 hrs or until epithelialized. |
|
|
In an event of resistance on removal of a PICC what do you do?
|
1 secure the line to the arm
2 warm pack to vasodilate the vein 3 reattempt removal after 15-30 min |
|
|
What do you do if meeting persistant resistance after 2 attempts?
|
obtain an x-ray to rule out a knot in the line.
|
|
|
For a PIV:
Is less than how many inch? Intended for short term therapy for how many days? pH? osmolality? |
less than 3 in
1-6 days pH 5-9 osmolality <600 |
|
|
Midline Catheters:
_to _ inches in length? intended for how long? pH? osmolality? |
3 to 8 inches
6day to 4 weeks pH of 5-9 osmolality <600 mOsm/L |
|
|
Is the insertion of a midline a sterile procedure?
|
Yes
|
|
|
Which vein are used for the midline insertion?
|
basilic and cephalic
|
|
|
What size syringe is used to flush central lines?
|
10 ml or larger
|
|
|
Dressing Changes:
What type of dressing is rrecommended? |
(TSM) transparent semi-permable polyurethane dressing
|
|
|
How often is a TSM dressing changed?
|
every 7 days or as needed
|
|
|
How often is a gauze dressing changed?
|
every 2 days or as needed
|
|
|
What is the preferred skin antiseptic?
|
>0.5% chlorahexadine with alcohol
|
|
|
If allergic to chlorahexadine, what are alternative skin antiseptics?
|
1% or 2% tincture of iodine
70% alcohol iodophors |
|
|
Replace a PIV no more frequently than ________ to ______ hrs.
|
72 to 96 hours
|
|
|
Midline
When removed what is placed over the site and for how long? |
Place sterile gauze with anitseptic ointment over the site while applying continuous pressure. Leave dressing on for at least 24 hrs or until site is epithelialized.
|
|
|
How often do you replace a PIV in pediatrics?
|
Replace PIV in children only when clinically indicated
p49 |
|
|
What does the French scale measure?
|
It is the measurement of the outside diameter of the catheter.
An increasing Fr size corresponds to a larger diameter catheter. p51 |
|
|
What do the catheter Fr sizes range from?
|
1.9 Fr (neonatal PICCs) to 15 Fr (some dialysis CVADs)
p 51 |
|
|
Gauge scale abbreviated g, what does the g sizes range from?
|
Gauge sizes range from 30g (intradermal injections) up to 14 g.
the larger the g the narrower the bore of needle. |
|
|
Catheter materials in the US are radiopaque, why?
|
To facilitate location of catheter emboli in the event of shearing or fracture.
p51 |
|
|
What are the most commonly used catheter materials?
|
Silicone
Polyurethane |
|
|
What is the difference between silicone and polyurethane?
|
Silicone is not affected by chemicals such as alcohol
Polyurethane is affected by alcohol, some are designed to be "power injectable" withstand pressures of approximately 300 PSI |
|
|
PIV
what is the dwell time? |
72-96hrs
|
|
|
PIV
What is the g ranges? |
24g to 14 g
|
|
|
PIV
When using a butterfly or winged needle what is it intended for? |
single use administration
Not recommended for chemo administration |
|
|
Midline
Give a description of a midline |
Approx 20 cmin length and terminates in the upper arm at the level of the axilla.
p53 |
|
|
Midline
what is the dwell time |
2-4 weeks
|
|
|
Midline
What is the infusate parameters? |
pH of 5-9
osmolality <600mOsm/L |
|
|
Midline
What are the common veins accessed? |
basilic
brachial cephalic |
|
|
Nontunneled CVAD
What is the dwell time? |
up to 7 days
|
|
|
Non tunneled CVAD
What is a description of this? |
see p 54
|
|
|
Non tunneled CVAD
What are the common veins accessed? |
Internal jugular
external jugular (not common) axillary (not common) subclavian femoral (not recommended) |
|
|
PICC
common vein accessed? |
basilic
brachial cephalic IJ option for pts with poor access (not an RN access) p55 |
|
|
Tunneled CVAD
What is a description? |
Single, dual or triple lumen with tip in the distal SVC or CA Junc.
Antimicrobial cuff is present on the catheter below the skin surface and helps secure the CVC once the cuff has been embeded Aval in power injectable |
|
|
Tunneled CVAD
What is the dwell time? |
Years
|
|
|
Tunneled CVAD
Common veins used? |
Subclavian
internal jugular |
|
|
Implanted ports
What is the dwell time? |
Years
|
|
|
Implanted ports
Common veins accessed? |
subclavian
IJ |
|
|
Implanted ports
How many ports can be available? |
single or double
|
|
|
Implanted ports
When is the port the device of choice? |
Preferred device for frequent or long term intermittent IV therapy due to ease of use and low CRBSI rates
p 58 |
|
|
Implanted ports
What type of needle is used to access a port? |
Non-coring needle
|
|
|
Short term dialysis & apheresis
What is the dwell time? |
No more than 1 week
|
|
|
Short term dialysis & apheresis
What is the 1st choice and 2nd choice of veins accessed? |
1st choice: Right IJ
2nd choice: Left IJ |
|
|
Short term dialysis & apheresis
What veins are avoided to preserve the vasculature for future fistula placement? |
Subclavin
axillary cause of high rates of stenosis p60 |
|
|
Short term dialysis & apheresis
Large bore catheter are used what is the Fr size |
12-15 Fr
|
|
|
Short term dialysis & apheresis
What is the flow rates for dialysis? |
at least 350 ml/minute
|
|
|
Short term dialysis & apheresis
What is the flow rates for apheresis? |
90-120 ml/minute
|
|
|
Short term dialysis & apheresis
What is the tip placement for short term catheters? |
distal/ca junction
|
|
|
Long term dialysis
What is the tip placement? |
Proximal right atrium
|
|
|
What is the difference on the placement of long vs short term dialysis catheters?
|
Long term dialysis is inserted with a short tunnel on chest or thorax
p60 |
|
|
Long term dialysis
What is the dwell time? |
weeks to months
|
|
|
Long term dialysis
Common veins accessed? |
Right IJ 1st
Left IJ 2nd Avoid the subclavin and axillary because of high stenosis rates p60 |
|
|
Which has higher infection rates Long term dialysis catheters or AVF?
|
Long term dialysis catheters
|
|
|
What is a pulmonary artery catheter?
|
Swan-ganz catheter
Used primarily for diagnostic purposes |
|
|
Where does a pulmonary artery catheter/ swan-ganz catheter originate and where does it terminate?
|
Common veins accessed:
R or L IJ Subclavin Femoral advanced to the pulmonary artery |
|
|
What is a pulmonary artery catheter used for?
|
Allows for pressures in the R atrium, R ventricle, pulmonary artery and wedge pressures (filling pressures of the left atrium)
detect heart failure sepsis evaluate the effects of drugs monitor therapy |
|
|
What is a SvO2 catheter?
|
Temporary CVAD with a special probe which is advanced and lodged into the ventricle wall providing instant readings of SvO2 or oxygen saturation of the ventricle tissues. p 62
|
|
|
What is the SvO2 catheter designed to do?
|
Designed to monitor mixed venous oxygen saturation and provides on going measurements of oxygen consumption and ability to assess dramatic changes in the critically ill patient. p62
|
|
|
Common veins accessed for the SvO2 catheter?
|
IJs
Subclavian Axillary |
|
|
Dwell time for the SvO2 catheter?
|
Days
|
|
|
Common veins used for an aquapheresis catheter?
|
IJs
Axillary Subclavian |
|
|
What is the dwell time for an aquapheresis catheter?
|
No more than a few days
p63 |
|
|
What is an aquapheresis catheter used for?
|
Remove excess salt and water from pts suffering with severe fluid overload that cannot be readily treated with traditional diuretics as seen in end stage heart failure. p 63
|
|
|
What are arterial catheters used for?
|

Used in CC settings for continuous blood pressure monitoring,
used for blood gas measurements and lab specimens |
|
|
What is the dwell time of arterial catheters?
|
Days
|
|
|
What can be infused thru the art line?
|
No infusions other than NS flushes.
|
|
|
Common veins used for the art line?
|
Radial artery
Brachial artery Femoral artery |
|
|
Art lines should not be used for injection or IV meds, why?
|
Can cause arterial spasms, tissue damage and amputation.
p63 |
|
|
When is an umbilical venous catheter used?
|
Short term access in critically ill infants and neonates, up to 1 week of age.
p64 |
|
|
Umbilical venous catheters come in how many lumens?
|
single or double
|
|
|
Umbilical venous catheters have a dwell time of?
|
Up to 14 days.
p64 |
|
|
Where is the tip location of a umbilical venous catheter?
|
Tip of the catheter should be in the IVC above the level of the diaphragm.
This allows for CVP monitoring, infusion of meds/solutions or TPN. p64 |
|
|
US guidance:
What is it used for? |
US is used to
locate veins determine vein depth, diameter and compressibility p 65 |
|
|
US guidance:
Is there high success rates with US guidance and IJ placements? |
CVAD placement in IJ site is associated with high success rate, decreased mechanical complications and more rapid catheter placements.
p65 |
|
|
US guidance:
What are the thoughts of rate of success for the subclavian insertions? |
Mixed results reported with use of US guidance during subclavian catherization due to difficulty visualizing subclavian vein p65
This technique requires training and is recommended especially for internal jugular vein or axillary vein catheterization. |
|
|
What is the transverse plane on the US?
|
The cross sectional dimension of an object/ able to view the diameter of a vein.
p67 |
|
|
Medical Imaging Technology: What are the three devices used?
|
Fluoroscopy
Tranillumination Infrared and near infrared vessel identification |
|
|
Medical Imaging Technology:
How does fluoroscopy add in insertion and placement of a CVAD? |
Fluoroscopy facilitates the initial puncture and also subsequent manipulations (stenosis, kinks, sharp angle and inadvertent entry into collateral pathways)
|
|
|
Medical Imaging Technology:
What is transillumination? |
Veins are visualized because red blood cells absorb colors of the light.
Used for peripheral IV and lab draws Useful for patients with poor access or obesity |
|
|
Infrared and near infrared vessel identification technology, how does it work?
|
primary application uses the fact that the transmission and absorption of near infrared (NIR) light in human body tissues contains information about hemoglobin concentration changes.
p69 |
|
|
How does transillumination work?
|
veins are visualized because red blood cells absorb colors of the light. p69
|
|
|
Infrared and near infrared vessel identification technology illuminates what color?
|
green
|
|
|
Infrared and near infrared vessel identification technology and transillumination, which can penetrate subcutaneous tissue to a certain depth?
|
Infrared and near infrared vessel identification technology
p69 |
|
|
What is an intravascular doppler?
|
a stylet that has a doppler built into the tip to determine direction of bloodflow in the great vessels of the thorax: helps guide catheter towards distal SVC p70
|
|
|
What is a breakaway needle? And who are they used on?
|

1 Needles with prescored line down the back of the middle of the needle, used for shallow approaches
2 After catheter insertion breakaway neeldle is carefully w/drawn over the catheter 2 wings are grasped and broken Used primarily on neonates for PICCs smaller then 2 fr. |
|
|
What gauge needle is used for PICCs
|
21 g
|
|
|
What gauge is used for larger CVADs?
|
16-18 g
|
|
|
Topical anesthetics are routinely used for who and when?
|
For pediatrics
Routinely used for all types of venipunctures, including IV insertion and blood sampling. p72 |
|
|
What type of lidocaine is routinely used for PIV, PICCs and CVC insertions?q
|
1 or 2 %
|
|
|
What size gauge needle is used to inject lidocaine?
|
25-30 g
|
|
|
What is added to lidocaine to buffer it or lessen the burning?
|
Sodium bicarbonate
p 73 |
|
|
What normal saline also has similar effects as lidocaine for decreasing venipuncture pain?
|
Bacteriostatic normal saline
|
|
|
What type of needle is used to access a port?
|
A non coring needle
|
|
|
Non-coring needles are used to access what (3)?
|
implanted venous ports
hepatic arterial port/pumps intra-peritoneal ports p73 (see addit. sheets) |
|
|
When inserting a non-coring needle into a port what is ideal?
|
The needle should reach the bottom of the port reservoir and
the external portion should lie relatively flat against the skin. p73 |
|
|
What are the risks associated with non-coring needles?
|
Needle is very sharp, rebound injuries are common due to unusual force needed to overcome resistance of dense silicone septum.
needle designs can be active or passive p74 |
|
|
Needleless connectors were mandated by what?
|
Bloodborne Pathogen standard from the OSHA (Occupational Safety and Health Administration).
p74 |
|
|
Needleless connectors external surface must be cleansed with what and for how long?
|
Alcohol wipe or chlorhexidine and alcohol using friction for at least 15 to 30 seconds.
p74 |
|
|
How do you flush a split septum cap to prevent blood reflux into the catheter?
|

Split septum is on the left.
Clinician must apply positive pressure to last milliliter of flush or lock solution in syringe, clamp (if present) then disconnect syringe from needleless connector. p75 |
|
|
What are the 3 types of Mechanical valve/luer activated valves for needless connectors?
|
Negative displacement
Neutral displacement Positive displacement p75 |
|
|
How is a needless connector with a mechanical valve and negative displacement flushed?
|
apply positive pressure on flush syringe while clamping catheter then disconnect.
p75 |
|
|
How do you flush a positive pressure needleless connecter with a mechanical valve? Neutral displacement?
|
Clinician must disconnect flush syringe from needleless connector and clamp catheter after the syringe disconnection.
Clinician must disconnect syringe from needleless connector with no specific clamping sequence. p75 |
|
|
What does the maximal sterile barrier precautions include?
|
cap
mask sterile gown, sterile gloves large sterile drape (total body drape) masks worn by all in room p75 |
|
|
Why use a 10ml syringe or larger when flushing?
|
This allows the clinician to feel resistance or pressure when flushing against resistance.
p76 |
|
|
What is typically used to flush a catheter?
|
Normal saline 0.9%
p76 |
|
|
If there is a known incompatibility of infusate with NS or other elecrolyte solutions, what is used as a flush?
|
10ml of 5% dextrose solution followed by 10ml of NS flush.
p76 |
|
|
Is there a clear minimum vol of flush solution that has been proven to be most efficacious in every situation and for every device?
|
No, but it has become customary to flush with 10 ml of NS f (NaCL)or adult and older ped population.
p76 |
|
|
Pediatrics flush volumes of NS vary in what amounts?
|
0.5ml to 10ml
p77 |
|
|
Are stopcocks used as a single patient use?
|
Yes
p77 |
|
|
When should stopcocks be changed?
|
Should be changed with regularly scheduled IV tubing changes
p77 |
|
|
When are topical hemostatic agents used?
|
Used to stop bleeding within minutes with applied pressure immediately after CVC insertion procedures or post- insertion if bleeding is problematic.
p77 |
|
|
What is the only FDA approved agent for thrombotic catheter occlusions?
|
alteplase 2mg (Cathflo) or Cathflo Activase
generic: alteplase trade: Cathflo Formally known as t-pa or tissue plasminogen activator. p78 |
|
|
What is the mechanism of action of Cathflo?
|
t-PA is a naturally occurring enzyme in the body that dissolves fibrin in clots when the body's natural fibrinolytic system is activated to dissolve clots when no longer needed.
p78 |
|
|
When is t-PA indicated?
|
For suspected thrombotic catheter occlusions or dysfunction when external mechanical occlusions have been ruled out; inability to infuse and/or lack of brisk bl return p78
|
|
|
What is the dosage for Cathflo?
|
2mg/2ml for adults and children >66lbs or 30kg and at least 2wks of age.
p78 |
|
|
What is the efficacy of alteplase?
|
83% restoration of patency with up to 2 doses, each dose instilled for up to 2 hrs.
p78 |
|
|
What agent is used to dissolve a lipid precipitate/fat emulsions?
|
70% ethanol (ethyl alcohol)
|
|
|
What dosage of 70% ethanol is used to dissolve a lipid precipitate? And what is the dwell time?
|
Catheter fill volume and 1 hour
p79 |
|
|
What are the precautions when using 70% ethanol in a catheter?
|
Do not use with polyurethane catheters as alcohol is known to degrade polyurethane over time with repeated and prolonged exposure.
p79 |
|
|
What agent is used to dissolve mineral/acidic precipitate (pH1-5) in a catheter?
|
hydrochloric acid (HCl)
p79 |
|
|
What is the dosage of hydrochloric acid for a mineral/acidic precipitate (pH1-5)? And the dwell time?
|
1ml of 0.1 Normal HCl
20 min, may repeat 1-2 times p79 |
|
|
What agent is used to dissolve alkaline precipitate/high pH 9-12 in a catheter?
|
sodium bicarbonate (NaHCO3)
p79 |
|
|
What is the dosage of sodium bicarbonate (NaHCO3) for an occluded catheter? And the dwell time?
|
1ml of 8.4% of NaHCO3 and for 1 hr.
p79 |
|
|
Antiseptic
|
A chemical agent that destroys or inhibits microorganisms on skin or tissue and has an effect of limiting or optimally preventing infection.
p80 |
|
|
Disinfectant?
|
A chemical agent that destroys microorganisms on inanimate objects.
p80 |
|
|
Bactericidal
|
Kills microorganisms
|
|
|
Bacteriostatic?
|
Temporarily prevents microorganisms from multiplication, disrupts minor chemical reactions and slows metabolism resulting in increased time
|
|
|
Properties of ideal skin antiseptic agents (6)?
|
1. broad spectrum of activity
2. rapid bactericidal activity 3. persistence or residual properties on the skin 4. maintain its activity in the presence of organic material 5 be non-irritating or have low allergic and/or toxic responses 6. no or minimal systemic absorption p.80 |
|
|
Name the 3 types of solutions used on the skin?
|
Chlorhexidine
Iodophors Alcohol |
|
|
Chlorhexidine is a broad spectrum antiseptic what is it effective against?
|
gram positive
gram negative fair fungicidal agent effective against most viruses p81 |
|
|
Chlorahexidine has a strong skin-binding property with up to how many hours of residual activity?
|
6 hours
p81 |
|
|
What % of Chlorahexidine with alcohol is preferred for insertion and maintenance site care of CVAD?
|
>0.5% of Chlorahexidine
p81 |
|
|
Pediatrics:
What age group can chlorahexidine be used? |
Not currently labeled for infants <2 months of age but there is supporting evidence to support its safety and effectiveness.
p81 |
|
|
Iodophors, what is it?
|
Solutions of iodine in complexes that contain a low amount of free iodine.
p81 |
|
|
Povidone-iodine (Betadine) solutions contain up to ___% of an iodine complex and provide up to ___% free iodine for skin antisepsis.
|
10% and 1%
p82 |
|
|
Iodine tinctures and iodophors are safe antimicrobial agents effective against what?
|
gram positive bacteria
gram negative bacteria fungi virsus have minimal effect on bacterial spores p82 |
|
|
How long does iodine antiseptic need to be on the skin to be effective?
How long is the residual effect? |
2 minutes or more to release free iodine.
2 hours (residual effect) p82 |
|
|
What happens when iodine comes into contact with organic matter such as blood?
|
It is neutralized and no longer effective.
p82 |
|
|
Is iodophors recommended for skin antisepsis for the neonate population?
|
Percutaneous absorption of iodine has been noted in neonates, with hypothyroidism induction in the newborn.
Iodophor solutions are usually not used in neonatal and infant populations. p82 |
|
|
What is the most common concentration (%) of isopropyl alcohol used for skin antisepsis?
|
70%
|
|
|
Alcohol demonstrates bactericidal effect on what organisms (4)?
|
gram positive bacteria
gram negative bacteria fungicidal virucidal p82 |
|
|
What is the residual effect of alcohol?
|
gone once it evaporates
p83 |
|
|
Adhesive remover should not be used where?
|
Do not use directly on insertion site.
p83 |
|
|
What are the benefits of a skin protectant?
|
Protects skin intergrity in pts with thin fragile skin
Enable dressing to adhere to skin, especially in diaphoretic pts Do no use directly on the insertion site p83 |
|
|
How many liters of blood flow per minute with the body at rest?
|
5 liters per minute
p88 |
|
|
What is a direct measures of hemodynamic monitoring? (1)
Indirect measures of cardiac output (3)? |
direct: pulse rate and quality
indirect: bl pressure central venous pressure continuous ECG p89 |
|
|
What is considered acidic/alkaline?
|
pH<5 for acidic
pH>9 for alkaline p91 |
|
|
What 3 factors will increase the risk of catheter-related venous thrombosis?
|
Inflammatory diseases
Solid tumor malignancies Increased dwell time of catheter. p92 |
|
|
Which veins are of critical importance for the creation of hemodialysis fistula?
|
Veins of the forearm, upper arm and subclavian.
p93 |
|
|
Internal jugular vein is preferred vessel for central venous access, what french size and inserted how?
|
<8 french and inserted via subcutaneous tunnel (reduces risk of CLABSI)
p93 |
|
|
When are the 3 times a PICC would be appropriate for placement in a dialysis patient?
|
Short life expectancy
Previous failure of arteriovenous access Severe peripheral arterial disease with no possibility of future fistula construction in that limb. p94 |
|
|
What are the reasons for increase in number of leukocytes in the circulating blood?
|
Infection
hemorrhage coronary occlusion malignant process or growth pregnancy toxemia |
|
|
When is it considered to place CVAD when the WBC is elevated?
What is the risk of placing CVAD when WBC is elevated? |
newly dxed leukemia pt often presents with elevated WBC. Immediate insertion of tunneled or PICC may be indicated for chemo.
May initiate bacterial "seeding" of catheter. p94 |
|
|
WBC normal range ?
Leukocytosis? |
4.5 - 10 thousand per microliter
Increase in # of leukocytes (above 10,000/mm) in circulating blood. p94 |
|
|
What is the normal range of plts?
|
150-450 thousand per mcL
p94 |
|
|
What is the usual lower limit for safe CVAD insertion into major thoracic vein?
|
6 - 37 thousand per mcL
p94 |
|
|
What is the device of choice for lower plt counts?
|
PICC (<150 thousand per mcL)
p94 |
|
|
What does creatinine measure?
How is it measured? |
Creatinine is a measure of kidney func
Chemical waste molecule generated from muscle metabolism and transported via blood to kidneys and filtered into the urine. p95 |
|
|
An elevated serum creatinine of what value or greater should have expert vascular access assessment before placement of any vascular access device?
|
2ml/dl or greater
p95 |
|
|
What does PT and INR measure?
|
extrinsic pathway of coagulation. p95
Extrinsic Pathway - Is initiated with material outside of or "extrinsic" to the blood. This material, Tissue Thromboplastin (Factor III), is released by damaged tissue cells. Factor III permits the clotting process to take a chemical shortcut. As a result, the extrinsic pathway is a very rapid process, i.e., within 12 to 15 seconds. However, the production of Thrombin is low and the resulting clot is small. This pathway is most effective as a "quick patch" process. |
|
|
PT and INR are used to do what? (4)
|
Monitor clotting tendency of blood
Measure warfarin anticoagulation Measure liver function Assess prior to invasive procedures such as CVAD insertion. p95 |
|
|
What are normal ranges for PT and INR?
|
PT 11-16 seconds
INR 0.8-1.2 seconds **INR indicative of therapeutic anticoagulation may be higher INR up to 2.5 when anticoagulants such as warfarin are used. p96 |
|
|
What does the PTT measure?
|
Partial thromboplastin time measures intrinsic coagulation pathway. p96
Intrinsic Pathway - Is initiated by the blood coming in contact with exposed collagen in the blood vessel wall, i.e., material within the blood or blood vessel wall. This process is considerably slower (5 to 10 minutes) but results in the formation of larger amounts of thrombin. This allows the formation of larger clots. |
|
|
Air Embolus:
Arterial air embolism can result in what? |
Produces ischemia of any organ or extremity with poor collateral circulation.
p96 |
|
|
Air embolism:
What are the causes? (7) |
1. Fracture of detachment of catheter connections.
2.Inadequate priming and/or failure to clamp lumens with open to air. 3. Presence of a persistent catheter tract following CVAD removal 4. Deep inspiration during insertion or removal (increases neg pressure within thorax) 5. Upright position reduces central venous pressure 6. Hypovolemia reduces central venous pressure. 7. Malfuction of self sealing valves in introducer sheaths. p98 |
|
|
What are the signs and symptoms of an air embolism?
|
Dyspnea
Substernal chest pain Sense of doom Hemodynamic collapse p98 |
|
|
How does one prevent an air embolism?
|
Position pt in supine or Trendelenburg during insertion/removal
Ask pt to Valsalva or hold his breath at CVAD insertion into chest veins and at removal Occlude hub of the central venous catheter during insertion Treat hypovolemia prior to catheter placement if possible Use only luer lock connections p98 |
|
|
What is the intervention for an air embolism?
|
*Place pt on the left side in Trendelenburg position
* Quickly identify the source of air entry and prevent further air embolization * Administer oxygen if available * Notify physician * Monitor pt and vital signs closely * Pt needs to be in an acute care setting. *Supportive care (mech ventilation, vasopressors, vol resuscitation) *Aspirate air from venous system only if central line is present. *Closed chest cardiac massage p98 |
|
|
What is the second most common complication of non-imaging guided central venous access?
|
Arterial puncture
p100 |
|
|
Incidence of arterial puncture during attempted venous access performed without imaging guidance can be as high as ________%?
|
7%
p100 |
|
|
What are the 3 complications of an arterial puncture?
|
Hemothorax
Major hematoma (especially the subclavin) Compartment syndrome (serious condition that involves increased pressure in a muscle compartment. It can lead to muscle and nerve damage/problems with blood flow) * especially damaging if artery in arm is punctured and unrecognized. p100 |
|
|
Why is it easy to have an arterial stick when placing a CVAD in a peds pt?
|
In small infants, arteries can be compressed.
p100 |
|
|
What are the s/s of an arterial puncture?
|
*Bright red pulsatile bl return
*Pulsatile bl return may not be present in pts with very low bl pressure and catheter placement in the extrermity. *Abrupt swelling at puncture site *Pain, numbness, pallor or absence of pulse in affected extremity distal to punc site. *Retrograde flow of blood in IV tubing p100 |
|
|
How to prevent an arterial puncture? (7)
|
* Knowledge of general anatomic location of arteries in access area
* Real time ultrasound guidance in all CVC/PICC insertions * Careful assessment of vessels prior to access * Awareness of pts baseline coags * Assessmt of bl return thru introducer needle prior to the dilator. * Ability to visulize needle bevel as it enters the vein * If not using USG, careful palpation of vessels to discern superficial artery vs vein. p100 |
|
|
What is the intervention with an arterial puncture?
|
* If an artery vs vein placement is uncertain obtain bl gas sample for immediate interpretation.
* Prompt removal of needle/dilator/sheath/catheter when known arterial punc *Apply pressure 5-10 min *Apply pressure dressing * May need to apply hemostatic dressing. *Observe for additional bleeding *Document adverse event/s/s/ interventions p100 |
|
|
Whatt is a Hemothorax?
|
Blood in the pleural cavity?
|
|
|
Accessing which veins will put you at risk for a hemothorax?
|
axillary
subclavin IJ p101 |
|
|
How is a hemothorax caused?
|
Rare complication.....
likely dure to forceful insertion of introducer or catheter against vessel wall. p101 |
|
|
What are the s/s of a hemothorax?
|
dyspnea
shallow breathing chest pain hypotension tachycardia restlessness anxiety |
|
|
How do you prevent a hemothorax?
|
ultrasound guidance
avoid forecful insertion of dilator/sheath/catheter p101 |
|
|
What interventions are taken in the event of a hemothorax?
|
*Transfer pt to a higher level of care
*CXR or CT scan *Chest tube placement to remove blood and/or air *Repair injury to vessel *Stabilize the pt p101 |
|
|
What is a pneumothorax?
|
Air in the pleural space between the lung and the chest wall
|
|
|
What is the most common insertion where a pneumothorax can take place?.
|
Subclavin...most common with attempts at insertion into the subclavian vein as the apex of the lung lies above the subclavian
p102 |
|
|
What are the causes of a pneumothorax?
|
Not using US guidance and using just landmark insertion
multiple unsuccessful attempts in the upper chest (subclavian) p102 |
|
|
What are the s/s of pneumothorax?
|
*There may not be any s/s
*S/S are determined by air leak size and speed by which it occurs chest pain SOB p102 |
|
|
How does one prevent pneumothorax on insertion?
|
*Insert CVAD into an axillary vein located outside border of the first rib (beyond the apex of the lung field)
*US guidance *Avoid back walling p102 |
|
|
What interventions are taken when a pneumothorax has happened on insertion?
|
*CXR to determine size of the pneumo
*Small pneumo typically resolves without tx especially in pts without underlying lung disease. *Observe pts for 48 hrs for s/s *For larger or symptomatic ones a chest tube or needle may be inserted to remove air *Repeated or unsuccessful attempts are an indication for follow up CXR to rule out pneumo or other detectable complications. p102 |
|
|
What are causes of difficult catheter advancement?
|
*Congenital aberrant vascular anatomy
*Acquired vessel damage from trauma and/or accidents *Repeated CVAD insertions *Prolonged dwell times causing progressive thrombosis and stenosis of vessels along the route of intended catheter placemt *Poor catheter tip location *Large diameter catheter in small vein. *Infusion of caustic and irritating causing vessel damage *Mod to severe dehydration *Environment too cold *Venospasm *Pt with pain *Pt with anxiety p103 |
|
|
What are the s/s of difficult catheter advancement?
|
Unable to advance catheter based on feel and/or based on indicators when using catheter navigation system.
p103 |
|
|
What are ways to prevent difficult catheter advancement problems?
|
Obtain a pt hx/assessment
hx of anxiety hx of difficult hospitalization Peds *Assess need for sedation *Apply warm packs to aid vasodilation *Obtain detailed hx of previous CVADs *Assure pt is adequately hydrated *Assure rm temp is comfortable for pt or use warming blankets as needed. p103 |
|
|
Interventions for difficult catheter advancement?
|
*If meeting resistance stop and assess how far catheter has advanced
*W/draw catheter a short distance and redirect *Adjust arm position *Ask pt to cough *Ask pt to turn head to side *Refer to IR p103 |
|
|
What is the risk of a malpositioned catheter?
|
Risk of dysfunctional catheter, venous thrombosis and vessel erosion
p105 |
|
|
What are the causes of a malpositioned catheter?
|
*Misdirection of CVAD on insertion
*Aberrant vasculature *Stenosis/thrombosis *Pacemaker/AICD *Venospasm *Over insertion *Inadequate catheter length *Increased intra-thoracic pressures ventilated pts coughing forceful flushing High central venous pressure CHF Pulmon hypertension p105 |
|
|
What are interventions for a malpositioned catheter?
|
*If in the ipsilateral jugular vein, rapid flushing with saline may help small bore cath to flip back.
*Reposition the arm or pt *Pull back cath that is too deep *Consider cath exchange or IR referral if grossly malpositioned. p105 |
|
|
What are the complications of a catheter or wire embolus?
|
*thrombosis
*infections such as septic thrombophlebitis *post-phlebitic syndrome *pulmonary emboliism p106 *arrhythmias *cardiac and vascular damage |
|
|
What are the causes of catheter or wire embolus?
|
*Operator error
*Over-insertion of guidewire *Shearing of catheter or guidewire by pulling/withdrawing wire or catheter thru introducer against resistance *Complete rupture of catheter internally due to excessively forceful flushing of cath with small syringe. p106 |
|
|
S/S of catheter or wire embolus?
|
*often asymptomatic
*Sometimes recognized at the end of the procedure. *Symptoms SOB/Dyspnea Anxiety Tachycardia Sudden pain at insertion site Flank pain p106 |
|
|
What are ways to prevent catheter or wire embolus?
|
*Use US guidance
*Avoid CVAD in subclavian beneath the clavicle .....devices placed via the SVC must enter laterally so device resides within the vein before passing thru the costoclavicular space to diminish risk of pinch off syndrome. *Hold distal end of wire at all times *Do not remove wire if there is resistance *PICCs placed using MST, insert guidewire 15-20 cm into the vein *Avoid forceful flushing p106 |
|
|
What are the interventions for a catheter or wire embolus?
|
PICC with suspected or known catheter embolus
*Apply tourniquet high in the axilla in attempt to retain fragment or embolus * Apply tourniquet tightly enough to restrict venous bl flow but not arterial bl flow * Notify MD * Pt on bedrest * Order radiographic studies * Assess pulses distal to the tourniquet every 5 min * Refer to IR * Individualize mgmt of high risk pts according to operative risk associated with leaving material in-situ p106 |
|
|
How does a cardiac arrhythmia occur during a CVAD insertion?
|
Catheter tip touching sino-atrial node or ectopic foci in the right atrium.
May manifest as tachycardia/PVCs Can occur during pre or post insertion. **Exception is dialysis CVAD: tips should reside in the proximal right atrium for adequate flows p108 |
|
|
What causes cardiac arrhythmias in CVAD insertions?
|
*Over-insertion of guidewire or catheter into right atrium
*Pts with ectopic foci may be sensitive to abnormal triggers *Post-insertion migration *Inadequate catheter securement at exit site p109 |
|
|
S/S of cardiac arrhythmias?
|
*Pt senses palpitations, rapid heart pounding and/or irregular heart rhythm
*Irregular pulse *Arrhythmia noted on cardiac monitor p109 |
|
|
How does one prevent cardiac arrhythmias?
|
*Careful measurement and documentation of external anatomic landmarks
*If pt is on a cardiac monitor, observe for new arrhythmias during insertion/withdraw guidewire/catheter if indicated *Place catheters in lower 1/3 of SVC or CA junc p109 |
|
|
What is the time frame that a CLABSI is a primary BSI in a patient that had a central line and is not bloodstream r/t an infection at another site?
|
48 hours
p110 |
|
|
What are the causes of a CRBSI or CLABSI?
|
Microbes present on pts skin are primary source of infx r/t percutaneously inserted CVAD...contamination by:
*Improper preparation of skin at insertion site *Poor hand hygiene *Femoral CVAD *Improper use or lack of MSBP *Contamination during insertion *Inserter inexperience *Failure to adhere to insertion checklist/protocol Patient Factors: *Age (elderly or premature infants) *Critically ill and co-morbidities *Immune disorders and neutropenia Maintenance care issues: p111 |
|
|
What are the s/s of a CRBSI AND CLABSI?
|
*Sepsis (fever, chills, flu-like symptoms)
*Presence of CVAD inserted within the past 48 hrs with no other obvious source of infection. *purulence, erythema at catheter exit site (not necessarily correlated with CRBSI) p111 |
|
|
How does on prevent a CLABSI/CRBSI?
|
*Adherence to evidence-based guidelines from insertion to maintenced
*Clinical staff education *Education to family/patients/caregivers PREVENTION STRATEGIES: *Hand hygiene *Avoid femoral *MSBP *Chlorhexidine for 30 seconds and allow to dry *Checklist Consistant care *Drsg change every 7 day or as needed *Use biopatch if CLABSI rates do not decrease despite adherence to all other CLABSI prevention strategies. *Selection of needleless connector with external and internal design to minimize microbial colonization and microbial entry. *Scrub the hub Maintain catheter patency as thrombotic catheter complications are associated with higher infection rates. *Daily review and documentation of line necessiity *Promptly remove unnecessary lines p112 |
|
|
What are the interventions to a CRBSI/CLABSI?
|
*Assess for s/s of catheter related infx
*Carefully examine pt to rule out other possible sources of infx. *Consider Time-to-Positivity Blood Cultures to determine if the cath is the source. *If blood culture drawn from catheter grows out faster by at least 2 hrs compared with peripheral blood culture drawn at the same time and both cultures grow out the same microorganism, the cath is the source of infx. *Antimicrobial therapy is based on identified/presumed microorganism *Draw blood cultures prior to initiation of antimicrobial therapy. p111 |
|
|
Can nerves be seen on ultrasound?
|
Nerves cannot be visualized with percutaneous insertion of catheters and cannot be seen on ultrasound except as nerve bundles in certain situations.
p113 |
|
|
What are the causes of nerve injury/irritation?
|
*Nerve contact with needle
*Insertion of needle/guidewire/dilator/sheath/ catheter thru a nerve bundle *Catheter resides in place with s/s of nerve damage *Temporary nerve irritation can occur with prolonged positioning of arm during cath insertion. p113 |
|
|
S/S of nerve injury/irritation?
|
*reports sudden electric shock like pain if in arm, pain may shoot down arm.
*In comatose/confused pts, arm may move reflexively and rapidly when nerve is touched. *Paralysis of extremity * Tingling/weakness p113 |
|
|
How does on prevent nerve irritation/injury?
|
*Inserter possesses knowledge of anatomic location of nerve
*If brachial vein is to be accessed visualize and identify median nerve with ultrasound. p113 |
|
|
What are the interventions to nerve injury/irritation?
|
*Recognition of nerve irritation or injury
*Prompt removal of needle or other material *Document s/s of injury/irritation and explain situation *Provide emotional support *Notify physician p113 |
|
|
Forceful flushing of a severely occluded CVAD can lead to
|
catheter breakage
catheter embolus venous thrombosis CRBSI p114 |
|
|
S/S of cath dysfunction/occlusion?
|
*There may not be any s/s
*Difficulty/inability to infuse *Inability to draw blood back, sluggish *Pain discomfort *flushing noise in ear *Leaking around the exit site *Leaking along cath track with infusion or flushing. p114 |
|
|
What are the interventions to prevent cath dysfunction or occlusion?
|
*Appropriate intervention depends on type of occlusion
*CXR may determine malposition or improper tip location *If completed occlusion or blood return is sluggish ...alteplase **For complete fibrin sheath, refer to IR for cath contrast study **Catheter stripping of fibrin can also be done on larger more permanent CVADs by IR p115 |
|
|
What causes extravasation?
|
*Infusion of hyosmolar solution or infusate that causes trauma to endothelial lining of tunica intima
*Inadequate securement of a VAD *Traumatic insertion *Multiple venipunctures *Nonverbal or sedated pt *Small or frail veins *PIV site in area of flexion *Use of an infusion pump or power injection *For CVADs: presence of a fibrin sheath, dislodged noncoring access needle in port. p116 |
|
|
How to prevent extravasation?
|
*Routine assessment of PIV and CVAD insertion sites
*Be familiar with agent know to produce tissue damage *Instruct pt to inform staff of pain and burning at insertion site. *Avoid using the dorsal surface of hand and areas of flexion where tendon and nerve damage is more likely *Give vesicants last when multiple drugs are ordered p116 |
|
|
What are the interventions for extravasation?
|
Nonpharm measures:
*Elevate extremity *Contact physician *Cooling applications are used for most except VINCA ALKALOIDS, VINCRISTINE and EPIPODOPHYLOTOXINS *Detailed documentation to include photo per policy *PHARM MEASURES: antidotes not generally recommended based on limited data except for sodium thiosulfate for mechlorethamine hydrochloride and concentrated cisplatin extravasations p116 |
|
|
What are the vinca alkaloids?
|
Cancer drugs
Vinblastine Vincristine vindesine Vinorelbine p116 |
|
|
What is Epipodophylotoxins?
|
Medication to treat cancer
Etoposide Teniposide p116 |
|
|
What medication is used to treat extravasation of mechlorethamine hydrochloride (Mustargen)?
|
sodium thiosulfate
p116 |
|
|
NMC
If there is an extravasation of Dobutamine Dopamine Epinephrine Norepinephrine Phenylephrine Vasopressen What medication is given? |
Phentolamine
near p116 |
|
|
NMC
If there is an extravasation of (only listed some) Calcium Salts Dextrose (greater than 10%) Potassium TPN Vanco What medication is given? |
Hyaluronidase
near p 116 |
|
|
When a CVAD is inserted where, does one find a greater risk for pinch off syndrome?
|
Occurs when a long term CVAD is inserted into the subclavin vein close to the head of the clavicle, positioning the catheter in the small gap b/w the first rib and clavicle.
p117 |
|
|
What is the cause of pinch off syndrome?
|
Infraclavicular approach (between the first rib and clavicle)
p117 |
|
|
What are the s/s of pinch off syndrome?
|
*intermittent catheter occlusion that can be relieved by a change in position (raising the arm, rolling the shoulder)
*Catheters that are positional or appear to be occluded. p117 |
|
|
How to prevent pinch off syndrome or complications of pinch off syndrome?
|
*Use internal jugular vein
*Position pt's hand at his side for post CXR and not with the shoulder in a raised or forward position. *Radiographic followup of long term infraclavicular indwelling CVADs should be performed routinely to detect pinch off syn, fracture or embolization. p117 |
|
|
What is the intervention for pinch off syndrome?
|
*Pinch off syndrome can occur immediately or there have been reports of detection after 5 yrs of dwell.
*If the subclavian vein is used and upright CXR should be obtained after the procedure and periodically thereafter *In case of pinch off syndrome GRADE 2 it is recommended that the CVC be removed. p117 |
|
|
Pinch off Syndrome is graded from 1-3, describe each of them?
|
Grade 1: abrupt change in the course of the catheter w/o luminal narrowing.
Grade 2: Luminal narrowing. Grade 3: Complete catheter fracture. near p 117 |
|
|
What are the causes of a broken/leaking catheter?
|
*Excessive pressure when inserting or flushing catheter
*Manipulating catheter when there is resistance *Sharp instruments near external portion of catheter *Use of toothed clamp on external portion of the catheter. p118 |
|
|
What are the s/s of broken/leaking catheter?
|
*S/S may be absent
*Obvious breakage of the external portion of the catheter. *Leakage at exit site *Wet drsg *Moisture/leakage noted when flushing or infusing p118 |
|
|
How does one prevent broken/leaking catheter?
|
*Never w/draw against resistance or flush against resistance
*Do not flush with smaller than 10ml syringe. *Secure external portion of catheter to prevent tension p118 |
|
|
What are the interventions to a broken/leaking catheter?
|
*Have repair kit that is designed specifically for device
*Determine risks/benefits of repairing and/or removing catheter. p118 |
|
|
What is the risk of a dysfunctional catheter secondary to cath malposition/migration?
|
venous thrombosis
vessel erosion p119 |
|
|
What are the causes of a catheter malpostition/migration?
|
only listed some
*High central venous pressures as seen in : CHF, pulmonary hypertension *Vigorous exercise *Erosion by catheter tip into an extravascular area *if picc, arm movement up/down p119 |
|
|
S/S of catheter malpostition/migration?
|
*There may be no signs
*Lack of blood return or sluggish *Difficulty flushing or infusing *CXR reveals malposition *Swelling/pain *Hearing odd sound in the ear *Arrhythmias *Dyspnea *Hypotension p119 |
|
|
Prevention of catheter malpostition/migration?
|
*Optimal cath placemt
*device stabilization and drsg secured *Daily assessmt of line and pt (pain hearing sounds, etc) *Consider institutional policy for periodic CXRs to confirm cath tip location for long term CVADs p119 |
|
|
What is a venous thrombosis?
|
Formation of fibrin along the vessel wall. Fibrin production is stimulated by vessel injury or presence of a catheter. Fibrin can coat the cath surface and cause partial or total occlusion of vessels.
p120 |
|
|
What are the causes of Venous thrombosis?
|
*Ca dx
*Size and # of lumens *Microtrauma to the subclavian vein from repetitive overhead arm mvmt or vigorous exercise *Renal disease *Infammatory/infectious process *Pregnancy *Oral contraceptives *Vessel trauma on insertion *Cath tip malposition *Rigid cath *Prior CVC *Dwell time greater than 2 wks *Surgery/trauma *vessels in radiation field *Pt immobility *Effort related thrombosis (Paget-Schroetter syndrome) p120 |
|
|
What are the s/s of Venous thrombosis?
|
not all listed
* most are asymptomatic *Inability to aspirate/infuse *Leakage at insertion site *Erythema, pallor, edema of extremity *pain/numbness *pulmonary embolus *appearance of collateral veins *abnormalities of the costoclavicular junc. p120 |
|
|
How does one prevent Venous thrombosis?
|
*Pre insertion hx
*Vessel assessment prior to insertion *Vessel selection choose smallest cath that meets infusion needs *Use USG and MST *Routine flushing of CVAD *Avoid restrictive wrap of extremity *Instruct the pt to avoid heavy lifting/ repetitive motion with affected arm. p120 |
|
|
What anticoagulant is recommended for Venous thrombosis?
|
low molecular-weight heparin (LMWH)
unfractionated heparin vitamin K antagonist for at least 3 m per MD order p120 |
|
|
What are the interventions of Venous thrombosis?
|
*Cath removal is not routinely recommended
*Do not remove a cath when s/s of DVT are mild *Anticoagulant : LMWH or unfractionated heparin *Cath removal *Vitamin K antagonists (warfarin) for at least 3 months per md order p120 |
|
|
When is cath removal warranted in Venous thrombosis?
|
*Cath related infection
*malfunc not resolved with conservative interventions *anticoagulant therapy is contraindicated *massive or worsening s/s of DVT *Cath is no longer indicated p120 |
|
|
What is phlebitis?
|
Inflammation of the vein
p121 |
|
|
What are the 3 types of phlebitis?
|
CHEMICAL:
Administration of infusates or solutions that are acidic, alkaline or hyperosmolar MECHANICAL: *Insertion of large g cannula into small vessel *Vessel trauma during insertion *Excessive mvmt for manipulation of cannula *Inadequate securement *Extended dwell time of PIV BACTERIAL: Inadequate skin antisepsis and/or break in aseptic technique p122 |
|
|
What are the s/s of phlebitis?
|
*erythema (reddness of the skin)
*swelling *pain/tenderness *cording *red streak formation p122 |
|
|
How often does one assess a PIV in a peds for continuous infusions?
|
assess PIV site every hr
p122 |
|
|
How to prevent phlebitis?
|
*administer infusates with a pH b/w 5-9 and osmolarity <600
*use proper venipuncture techniques *Use proper securemt devices *Insert appropriate size PIV cath based on pts vessel size and prescribed therapy *Change PIV every 96 hrs p122 |
|
|
What are the interventions for phlebitis?
|
*Stop infusion at once
*Apply a warm pack (increases blood flow) *Consider starting a new PIV *Consider alternative VAD p122 |
|
|
Who requires that Manufacturer instructions for use (IFU) to include all info any user needs to reliably and safely use the product?
|
FDA
p123 |
|
|
FDA requires IFUs to include the following information?
|
*Proprietary and established product name
*Intended use for the product or equipment *Explanation of why the product is useful *Info on appropriate use at the time of insertion, implantation and/or use during dwell time *Instructions for use *Quality control requirements *Instructions for management of inherent residual risk/avoidance of misuse *Cleaning/sterilization instructions *List of accessories/consumables validated by the manufacturer *Requirements for safety inspections *Requirement for planned maintenance *Technical/clinical performance characteristics (accuracy, reliability) *Explanation of potential adverse outcomes *manufacturer name, place of business and contact info *date & most recent revision of pkg insert to verify most current info. p124 |
|
|
What are the different CXR views (4)?
|
Posterior-Anterior (PA)
Anterior-Posterior (AP) Oblique Lateral view p125 |
|
|
What is an anterior-posterior (AP) view on x-ray?
|
Back against the film as applies with a portable CXR.
*greater potential for distortion *Heart is further away from film: parallax effect with greater change in position. p125 |
|
|
What is a PA (posterior-anterior) CXR?
|
Board placed on the chest- image reflected on the board
*Heart sits anterior in chest *less distortion *greater radiation energy p125 |
|
|
What is an oblique CXR?
|
Pt's torso is angled to enhance visualization of catheter tip, away from anatomic structures such as spinal processes or artificial devices in chest such as wires, rods or catheters
p125 |
|
|
What are the radiographic anatomic landmarks to identify catheter tip placemnt?
|
1. 3-5 cm below the carina
2. Right tracheobronchial border 3. 1-2 cm below atrial appendage p125 |
|
|
What are the factors that interfere with interpretation of catheter tip?
|
*Wet lungs caused by fluid overload, pneumonia
*Morbid obesity, especially >300lbs and CXR is AP *Pacemaker/AICD wires *Other CVADs *Spinal rods *Pt position (from supine position to standing position, cath tip can move as much as 2-3 cm) *Arm position Catheter placed in the basilic vein will move more than those in the cephalic *Picc tips with move at least 2 cm closer to the right atrium, piccs placed in the right arm will move more than those place in the left. p126 |
|
|
Definitions:
Novice Advanced Beginner |
Novice: no experience in the skill needed to perform
Advanced beginner: able to demonstrate marginally acceptable performance p126 |
|
|
Definitions:
Competent Proficient Expert |
C: able to adequately perform the skill after conscious, abstract and analytic contemplation of the problem or situation.
P:Holistic understanding of the problem or situation and confidently performs the skill. E: intuitively grasp problems and situations and appears to effortlessly perform the skill p126 |
|
|
Professional licensure examines is a measure of what?
|
Measures minimal competency in a professional field.
p127 |
|
|
Competency assessment?
|
an eval measuring a set of skills and knowledge. Eval includes technical skills, critical thinking skills and ability to apply skills and knowledge in the right way at the right time.
p127 |
|
|
Certification?
|
Formal recognition of specialized knowledge, skills and experience demonstrated by achievement of standards identified by a professional organz or entity.
p127 |
|
|
Professional development?
|
The process of assessing and developing professional competencies
p127 |
|
|
Standards of practice?
|
authoritative statements by which a profession describes responsibilities for which its practitioners are accountable.
p127 |
|
|
Clinical practice guidelines?
|
systematically developed statements of appropriate care; issued by reputable authoritative organizations and based on current and relevant research.
p127 |
|
|
Nursing and medical education r/t vascular access and infusion therapy generally focuses on _____?
|
theory
p127 |
|
|
Is Hands on skill in vascular access usually acquired in the nursing workplace and physician residency programs? (T or F)
|
Usually, True
p127 |
|
|
What are the vascular access teaching techniques and aids?
|
* Simulator training using models and devices
* Virtual simulator training (model or device links to computer screen) * Virtual reality products (models respond with bleeding, vein collapse) *Anatomical models (Chester chest, Peter PICC line) *Tissue models and cadavers (human and animal) p128 |
|
|
What is the purpose of medical documentation?
|
*Provides enduring record of pt care
*Promotes communication among healthcare providers *Supports billing and reimbursement *Supplies data for internal/external analyses (disease incidence, outcome indicators, adverse events) p128 |
|
|
What are the documentation issues that increases risk of legal liability? (7)
|
1. Lack of doc of informed consent, treatment, pt teaching or discharge
2. Unexplained delays in treatment 3. Substandard or inappropriate tx 4. Charting inconsistencies or conflicting documentation 5. Late entries 6. Improper alterations of the medical record 7. Missing and/or destroyed records. p128 |
|
|
What are the 2 regulatory agencies for incident reporting on medical devices?
|
FDA MedWatch reporting
Manufacturer and User Facility Device Experience (MAUDE) p130 |
|
|
What are the 2 federal statutes (laws enacted by Congress) and regulations associated with product use?
|
Needlestick Safety and Prevention Act (2001)
Safe Medical Device Act (1990) p131 |
|
|
What is the Needlestick Safety and Prevention Act?
|
Mandated revision of the 1991 OSHA Bloodborne Pathogens Standard to include more engineering controls: requires exposure control plans, solicitation of employee input and detailed recordkeeping.
p131 |
|
|
What is the Safe Medical Device Act?
|
Requires device users to notify the FDA and device manufacturer (if known) of incidents in which a medical device may have contributed to serious injury, serious illness or death of a patient.
p131 |
|
|
What are the elements of negligence (4)?
|
* Duty of care
* Breach of duty * Causation * Legally compensable injury p131-2 |
|
|
Breach of duty?
|
Clinicians failure to provide care that is consistent with the standard of care.
Example: acts of commission ( med error) acts of omission (failure to properly monitor the pt p132 |
|
|
Causation?
|
Patients injuries must be the result of clinicians negligent conduct.
p132 |
|
|
Legally compensable injury?
|
Final element that must be proven when negligence/malpractice is allegedto have occurred. Pt must prove that injury has occurred and that it is the type of injury in which the law allows compensation.
Ex.:pain&suffering is allowable under some state laws but not in others. p132 |
|
|
What is the code of ethics for nurses?
|
*Practices with respect and compassion
*Has a primary commitment is to the pt *protects the pt and is an advocate for the pt. *Takes action when questionable or impaired practice occurs *is accountable & responsible for actions/practice *Owes the same duties to self as to others (self-respect, professional growth) *participates in advancement of the profession *collaborates with other health prof *articulates nursing values and maintains the integrity of the profession p133 * |
|
|
What are the ethical principles?
(Be just autonomous Veracity Truth) |
beneficence: the obligation to do no harm
Justice: fair and unbiased actions Autonomy: the right of a person to make independent decisions Veracity: obligation to tell the truth p133 |
|
|
Federal and state healthcare regulations mandate that pts have certain rights, what are the 5 rights?
|
1. Refusal of treatment
2. Discharge planning 3. Freedom for restraints and abuse 4. Confidentiality 5. Informed Consent p141 |
|
|
Patients have the right to confidentiality, what Act protects patients and what does it protect?
|
HIPAA, 1996 - Health Insurance Portability and Accountability Act:
provides federal protections for personal health info held by covered entities (hospitals, clinics, etc) and gives pts rights r/t that info. p141 |
|
|
What are the 2 organizations involved in patient safety goals r/t vascular access?
|
The Joint Commission National Patient Safety Goals (NPSG)
Institute for Healthcare Improvement (IHI) p145 |
|
|
What organization issued the Universal Protocol for Preventing Wrong Site, Wrong Procedure and Wrong Person Surgery and to perform the "time out" before starting a procedure?
|
Joint Commission National Patient Safety Goals (NPSG).
p145 |
|
|
IHI (Institute for Healthcare Improvement) patient safety provides resources for tracking 3 types of safety measures, what are they?
|
Outcomes
Process Balancing Outcomes:determine if changes are actually leading to improvemt. ex. central line infx incidence Process: determine if improvemts to core processes are occuring or being adhered to. Ex Central line bundle compliance Balancing: if changes in one part of the system is causing problems in other parts of the system. p146 |
|
|
What are some of the IHI initiatives r/t vascular access?
|
1. Prevention of central line infections
2. Prevention of surgical site infxs 3. Prevention of adverse drug events p146 |
|
|
What are the interventions that improve cultural competence in healthcare (5)?
|
1. Recruitment and retention of staff who reflect cultural diversity of the community served.
2. Use of interpreter services or bilingual providers for clients with limited English language and literacy proficiencies. 3. Ongoing cultural competency training for providers 4. Use of linguistically and culturally appropriate health educ materials 5. Culture specific healthcare programs p148 |
|
|
What is peer review?
|
Evaluation of work or performance by individuals in the same field in order to maintain or enhance the quality of the work or performance.
The word peer is often defined as a person of equal standing....generally used in a broader sense to refer to people in the same profession of the same or higher rank. p148 |
|
|
Statistics terms:
Incidence? |
Occurrence of new cases of disease for injury in a population over a specified pd of time.
p152 |
|
|
Statistics terms:
Prevalence? |
The number of cases, both old and new, present at a point in time in a defined population.
Ex: 10% of pts in the intensive care unit have positive bl cultures during the stay. p152 |
|
|
Statistics terms:
Morbidity? |
rate of which an illness or abnormality occurs, calculated by dividing the number of affected people in a group by the entire number of people in the group.
Ex. Morbidity of diabetes is 30% among hospitalized patients. p152 |
|
|
Statistics terms:
Mortality? |
Death rates
p152 |
|
|
Research:
Qualitative? |
Detailed descriptions of specific situations using interviews, observations and document review.
You describe things as they are. p153 (read) |
|
|
Research:
Quantitative? |
Numerical descriptions (frequency, average, mean, median, mode)
You measure things as they are. p153 (read) |
|
|
Research:
Randomization? |
A study in which there are two or more interventions and study participants are allocated at random (by change alone) to receive on of these interventions.
p153 |
|
|
Research:
Effect size? |
The difference b/w the groups studied and is a measure of strength of the relationship b/w two variables.
Effect size is one factor to determine necessary sample size. Large effect size increases the probability of statistical significance and power. p154 |
|
|
Research:
Meta-analysis? |
Method of summarizing and synthesizing results of findings accumulated from a variety of sources and studies. Combines results of several studies on one topic into one large study with many participants.
a. general aim is to more powerfully estimate the true "effect size" as opposed to a smaller "effect size" derived in a single study under a given single set of assumptions and conditions. b. Considered more informative than any one of the included studies in the analysis considered alone. p154 |
|
|
What is considered when evaluating research reports? (8)
|
* Read and critique the entire study
* Examine the significance of the prob * Determine if the literature review is current and complete * review the study design and study population and determine appropriateness to research question being posed. * Identify strengths (randomized study) and limitations of the study (conducted at one institution) * Review findings and their interpretation. Have inappropriate generalizations been made? * Determine the feasibility of replicating the study * Review usefulness of the findings to practice (Do study findings justify or support a change in clinical practice) p154 |
|
|
What is empirically-supported treatment?
|
evidence-based practice
p154 |
|
|
What is evidence-based practice?
|
a problem solving approach to the delivery of healthcare that intergrates the best evidence from well-designed studies and patient care data and combines it with patient preferences and values and (clinicians) expertise.
p154 |
|
|
What is considered the "gold standard of care"?
|
Evidence based practice.
p155 |
|
|
What are barriers to evidence-based practice?
|
*Lack of organizational culture and readiness
*lack of ebp mentors and champions *inadequate ebp knowledge and skills *lack of ebp valuing *large amt of aval info and literature *contradictory research findings *pt expectations and demands *conflicting priorities (workload may impair time for research activities) *level of clinician authority to initiate practice p155 |
|
|
What are the seven steps of evidence-based practice?
|
1. cultivate a spirit of inquiry
2. ask clinical questions in specific format (PICOT) *P: pt pop of interest *I: Intervention or area of interest *C:Comparison intervention group *O:Outcome *T:Time 3.Search for best practice 4.Critically appraise evidence 5.Integrate evidence with clinical expertise and pt preferences and values 6.Evaluate outcomes of practice decisions or changes based on evidence 7.Disseminate EBP results p156 |
|
|
Evidence based practice resources (3)?
|
1. Agency for Healthcare Research and Quality
2. Cochrane Database of Systemic Reviews 3.Clinical Evidence p156 |
|
|
What is "mistake proofing" for vascular access products?
|
use of design features to prevent errors or negative outcomes. Ex: coloring added to skin prep solution to enhance identification of areas missed during application
p156 |
|
|
Vascular access products:
What is failure mode effects analysis? |
The process of analyzing a product design to learn how it can fail.
Ex: identifying "work arounds" or short cuts used by clinicians when programming infusion pumps and using this info to improve pump design and function. p157 |
|
|
All equipment used to deliver infusion therapy is regulated by who (2)?
|
FDA
Center for Devices and Radiologic Health p 156 |
|
|
The device class determines the Center for Device and Radiologic Health review process.
What is a Class I, II and III device? |
Class I:devices with the lowest risk of pt harm (cath stabilization device, Iv poles)
Class II:devices with a moderate risk (catheters, introducers, wires) Class III: devices with the greatest risk (cardiac pacemakers, mechanical heart valves) p157 |
|
|
VA products:
Pre-market notification process? |
process of documenting that a new device is substantially equivalent to a similiar product sold in the US. Usually does not require clinical studies and is commonly used process for approving class II devices
p157 |
|
|
VA products:
Pre-market approval? |
process in which laboratory, animal and clinical studies are usually required to demonstrate that the device is safe and effective when used as directed. This process is used for most class III devices.
p157 |
|
|
VA products:
Post-market surveillance? |
Also known as a medical device reporting system (MDR). Involves device manufacturers, healthcare facilities and clinicians with the goal of identifying adverse events associated with the device. It is the process of reporting device malfunctions and serious injuries or deaths associated with a device to the FDA.
p158 |
|
|
Evaluation of new products:
What is life-cycle thinking? |
the process of considering the products life and the environment, including use and disposal
p158 |
|
|
Performance Improvement, a term introduced by who?
|
The joint commission for assessment and improvement of performance.
p159 |