Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
40 Cards in this Set
- Front
- Back
|
Homocystinuria
|
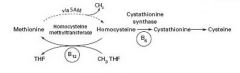
Homocystinuria results in mental retardation, marfanoid habitus, and lens subluxation (down & in). Increased risk of thromboembolic events in third decade.
3 forms: 1. Cystathionine synthase deficiency (requires vit B6 as a cofactor) 2. Decreased affinity of cystationine synthase for pyridoxal phosphate 3. Homocysteine methyltransferase deciciency |
|
|
Hypotensive infant at birth; elevated 17-hydroxyprogesterone
Physical exam: enlarged clitoris and partially fused labioscrotal folds |
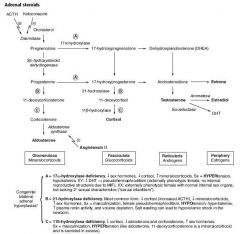
21-hydroxylase deficiency; only congenital adrenal hyperplasia that causes HYPOtension & salt wasting
Decreased ACTH and cortisol Masculinization, female pseudohermaphroditism |
|
|
Salt wasting
|
Hyponatremia + hyperkalemia; can cause hypovolemia
|
|
|
6-year-old boy is diagnosed with a worsening ataxic gait and a cardiac dysrhythmia
|
Freidreich's Ataxia - trinucleotide repeat disease
Trinucleotide repeat expansion diseases typically demonstrate anticipation and resulr in earlier manifestation of the clinical disease in subsequent generations. The unstable repeates in the frataxin gene impede protein translation, causing Freidreich's ataxia |
|
|
A 6-month-old child develops failure to thrive, developmental delay, and recurrent respiratory tract infections. The child is diagnosed with an autosomal recessive disease caused by a deficiency in N-acetylglucosamine phosphotransferase, which phosphorylates mannose residues
|
Failure to phosphorylate mannose residues results in targeting to lysosome instead of exocytosis
This is called I (inclusion) cell disease |
|
|
46-year-old patient who appears confused and is not oriented to time or place. The medical student notices the man's tense, distended abdomen, palmar erythema, and pronounced gynecomastia. The patient also has a hand tremor
|
Hepatic encephalopathy from chronic alcoholism. Hyperammonemia may result in asterixis, cerebral edema, and encephalopathy. In hyperammonemia, alpha-ketogluturate is consumed to make glutumate. Causes cessation of the citric acid cycle, which is an important source of energy for the brain. Ammonia is also neurotoxic.
|
|
|
Baby with ambigous genitalia, fused labia and hypotension.
|
HYPOtension - think 21 hydroxylase deficiency
|
|
|
2-year-old girl is brought to the clinic because she has recently developed muscle weakness and atrophy. Physical examination also reveals strabismus. A peripheral nerve biopsy reveals brown granules in Schwann cells and macrophages when stained with toluidine blue.
|
Arylsulfatase A deficiency aka metachromatic leukodystrophy. Lysosomal enzyme that cleaves sulfate from sulfatides. Results in accumulation of cerebroside sulfate. Appears brown when stained with toluidine blue.
|
|
|
A 3-week-old infant presents with failure to thrive, poor feeding, and lethargy. A physical examination reveals an enlarged liver and jaundice. Laboratory analysis reveals an elevated blood galactitol level and increased urinary reducing substance
|
Patiens with galactosemia lack the enzyme galactose-1-phosphate uridyltransferase. Build up of galactose-1-phosphate and galactitol. Reducing substance in urine.
|
|
|
Strabismus
|
Strabismus or tropia are the medical terms for eye conditions commonly called by various names: eye turns, crossed eyes, cross-eyed, wall-eyes, wandering eyes, deviating eye, etc. Strabismus is not the same condition as "lazy eye" (amblyopia).
|
|
|
Neurofibromatosis type 2
|
Bilateral schwannomas, juvenile cataracts. Tinnitus. Assoc w other CNS tumors including ependymomas.
|
|
|
Mechanism of angiotensin II signaling
|
Angiotensin II acts on smooth muscle cells to cause them to contract. It does this through angiotensin receptor type I, which is a seven transmembrane G-protein (Gq) coupled receptor that activates phospholipase C. PLC cleaves PIP2 to form IP3 and DAG. IP3 opens calcium channels and DAG activates PLC. Lisinopril, and ACE inhibitor, thus causes decreased activity of PLC in vascular smooth muscle, relaxing efferent renal arterioles, decreasing GFR.
|
|
|
Cystinuria
|
Defect in amino acid reabsorption in the proximal tubule. Recurrent nephrolithiasis. Pelvic pain. Increased lysine, arginine, ornithine and cystine in the urine. Only cystine precipitates at acidic pH. Treat with acetazolamide to hydrate and alkalanize the urine.
|
|
|
Seizure in a patient with 72 hours of vomiting and diarrhea.
|
Most likely due to hyponatremia. In general, vomiting and diarrhea cause solute and water loss. Hypovolemia causes increased ADH secretion, leading to water conservation and hyponatremia. Hyponatremia results in neurologic dysfunction induced by cerebral edema. Nausea and malaise below 125 -130 mEq Na, followed by headaches, lethargy, and obtundation. Seizures, coma, and respiratory arrest below 115-120 mEq/L plasma Na.
|
|
|
Hypocalcemia
|
Distal paresthesias, Chvostek's sign (twitching of perioral muscles after tapping the facial nerve anterior to the ear) and Trousseaus sign (carpal spasm after inflation of blood pressure cuff above systolic pressure for three minutes). Severe hypocalcemia can cause seizure, bronchospams, and QT prolongation.
|
|
|
Hyperkalemia
|
Weakness that can progress to flaccid paralysis, metabolic acidosis, peaked T waves on EKG, cardiac arrest
|
|
|
Arsenic poisoning
|
Dysphagia, stomach pains, vomiting, diarrhea, and a metallic breath
|
|
|
Acute intermittent porphyria
|
Build up of delta ALA and porphobilinogen in urine, which can turn red in 30 minutes. No basophilic stippling as seen in lead poisoning. Abdominal pain, polyneuropathy, and psychiatric symptoms.
|
|
|
Iron poisoning
|
Vomiting, diarrhea, abdominal pain, GI bleeding.
|
|
|
Porphyria cutanea tarda
|
Accumulation of uroporphyrin in urine, which turns urine the color of tea. Photosensitive skin lesions.
|
|
|
A patient presents to the clinic with a glycogen storage disease that is characterized by muscle pain and cramps after periods of intense exercise. Urinalysis indicates myoglobinuria.
|
Deficiency in glycogen phosphorylase, which shortens the glycogen chains by removing glucose 1 phosphate.
|
|
|
Pompe's disease
|
Deficiency in acid maltase. Lysosomes cannot be degraded. Cardiomegaly and early death.
|
|
|
Vitamin K deficiency in newborns
|
Sterile gut. Vitamin K synthesized by intestinal flora.
Newborns are given a vitamin K shot shortly after birth in the US to prevent bleeding. |
|
|
Chronic alcoholic with neurologic signs. Blood finding.
|
High serum lactate level. Chronic alcoholics have impaired intestinal absorption and often have thiamine deficiency. Thaimine is a cofactor for pyruvate dehydrogenase in the conversion of pyruvate to acetyl CoA. Thiamine deficiency results in shunting of pyruvate to lactate dehydrogenase instead.
|
|
|
LFTs in viral hepatitis
|
High serum ALT:AST ratio
|
|
|
LFTs in alcoholic hepatitis
|
High serum AST:ALT ratio
|
|
|
Northern blot
Southern blot Western blot |
Northern blot - mRNA
Southern blot - DNA Western blot - protein |
|
|
Lead poisoning
|
Blocks delta ALA dehydratase
|
|
|
Bilirubin glucuronyl transferase
|
Hepatic enzyme responsible for conjugation of bilirubin with glucuronide. Deficiency results in unconjugated bilirubinemia.
|
|
|
Why does HbF have an increased affinity for oxygen?
|
Has gamma chains in place of beta chains. Gamma chains have serine residues instead of charged histidine residues like beta chains. Beta chains binds to 2,3 DPG via histidine residues, decreasing the affinity of Hb for O2.
|
|
|
HbA1C
|
Formed by glycosylation of HbA
|
|
|
Diagnosis of thiamine (B1) deficiency
|
Erythrocyte transketolase activity
|
|
|
Wernicke sydnrome
|
Caused by deficiency of thiamine (B1) in alcoholics. Results in decreased glucose utilization which is especially apparent in the CNS.
Wernicke's traid: 1. Ophthalmoplegia 2. Ataxia 3. Confusion |
|
|
Enzymes for which thiamine is a cofactor
|
Enzymes involved in glucose utilization
1. pyruvate dehydrogenase (converts pyruvate to acetyl CoA) 2. a-ketogluturate dehydrogenase 3. transketolase (enzyme in HMP shunt) |
|
|
Treatment of acute intermittent porphyria
|
1. Intravenous heme preperations
2. glucose loading These work by negative feedback on delta ALA synthase, decreasing production of urinary ALA and porphyrobilinogen |
|
|
Lactic acidosis
|
High anion gap metabolic acidosis
Caused by a number of conditions that result in reduced tissue oxygenation. Impaired tissue oxygenation results decreases oxidative phosphorylation, resulting in shunting of pyruvate to lactate after glycolysis. |
|
|
Diabetic ketoacidosis
|
Increased lipogenesis and ketogenesis
|
|
|
Impaired renal tubule bicarbonate reabsorption
|
Type II (proximal) renal tubular acidosis
|
|
|
Cause of lactic acidosis and increased lung opacities in 87 yo nursing home resident with a history of dementia, stroke, and hemiparesis
|
swallowing muscle dysfunction leading to aspiration pneumonia
Aspiration pneumonia - intoxication, neurological disorders |
|
|
Beta thalassemia minor
|
Defective mRNA processing resulting in decreased beta globin production. Increased HbF. Mild. Iron is of no use in these patients.
|