Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
50 Cards in this Set
- Front
- Back
What is this an XR of?
|
pneumothorax
|
|
|
Describe where you would find the apex of the lung anteriorly.
|
about 2-4cm above the inner 1/3 of the clavicle.
|
|
|
At what level is the lower border of the scapula?
|
rib 7/7th intercostal
|
|

What is this an XR of?
|
Plueral effusion
|
|
|
Normal respiratory rate for adults
|
14-20 breaths per minute
|
|
|
Normal respiratory rate for children?
|
<2 mos = <60
2-12 months= <50 1-5yrs= <30 5-12yrs= <25 |
|
|
AP diameter changes with..? Also what is it called in pathologic states?
|
-age
-COPD, emphysema called "barrel chest" |
|
|
"pink buffers" and "blow bloaters"?
|
Pink buffers refers to pts with emphysema
Blue bloaters refers to pts with chronic bronchitis |
|
|
Hoover's sign
|
paradoxiclal movement during breathing (chest inward on inspiration, anbdomen outward) because of inward instead of downward movement of the diaphragm; a/w COPD, nl in newborns
|
|
|
Pectus excavatum
|
caved in (funnel) chest
|
|
|
Pectus carniatum
|
Pidgeon chest
|
|
|
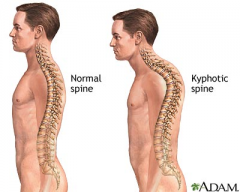
kyphosis; can be in combination with scoliosis and = thoracic kyphoscoliosis
|
|
|
Causes of asymmetric chest wall expansion?
|
-paralyzed hemidiaphram
-endobronchial mass obstructing air flow -pleural effusion -pneumothorectomy often best appreciated when standing at foot of bed |
|
|
Superior Vena Cava Syndrome
|
- direct obstruction the SVC by malignancies such as compression of it by R upper lobe tumores or mediastinal lypmphadenopathy; most common cause = bronchogenic carcinoma; sxs= SOB, swelling in face/arm
|
|
|
Cyanosis
|
blueish coloring, sign of hypoxemia
Central cyanosis (see in lips) vs acrocyanosis (extremities) |
|
|
Clubbing indicative of
|
chronic pulmonart, cardiac, liver diseases
|
|

|
Sign of Leser-Trelat
appearance of seborrheic keratosis in xmas tree pattern on the back, highly indicative of cancer |
|
|
6% of pts in ER with chest pain who had costochondritis (inflammation of the costal cartilage) had what?
|
an acute MI
|
|
|
Percussion..what fingers
|
3rd plexor strikes the DIP of the other 3rd pleximeter
|
|
|
5 sounds on percussion
|
Flat- thigh
Dull- liver Resonant- healthy lungs tympanitic- puffed of cheek Hyperrresonant- kronigs |
|
|
Kronigs sign
|
Absence of one of the 2 hyperresonant strips between the neck and shoulders (over the shoulders); suggest disease in the apical lung to pleura on that side
|
|
|
Diaphragmatic excursion usually...
|
should be symmetric and 5-6cm
abnormally high diaphragm can suggest plueral effusion, atelectasis, diaphragm paralysis |
|
|
How would a pleural effusion sound on percussion? What about fremitus?
|
dullness over aran of fluid collection, hyperresonant area just above it- "Skodaic resonance". No fremitus over area
|
|
|
Auscultation--what in general produces high or low frequencies?
|
high frequencies are air moving through narrowed spaces (ex wheezes, stridor)
low frequencies is air moving through water (ex: rhonchi |
|
|
Breath sounds are usually louder where?
|
lower posterior lung fields
|
|
|
pectoriloquy
|
when whispered sounds sound louder than normal on auscultation; indicative of consolidation
|
|
|
egophany
|
eee to ay change on ausculation; consolidation
|
|
|
Pneumonia
|
-increased fremitus
-egophany, pectoriloquy -bronchial or bronchiovesicular sounds (broncial=pause between insp and exp, predominantly ex) |
|
|
rales
|
aka crackles
sounds like hair between fingers early inspiratory- coarse rales: chronic brochitis, asthma late inspiratory- fine rales: pneumonia, CHF pulmonary fibrosis |
|
|
rhonchi
|
low frequencies sounds, secretions
|
|
|
Still's murmur
|
most common midsystolic murmur heard in children, ceased by carotid compression
|
|
|
differences in thorax of an infant
|
rounder, thinner musculature, xiphoid protrudes
|
|
|
Normal RR for infants
|
30-40 breaths per min alternating with periodic breathing
|
|
|
split S2 best heard on
|
inspiration
|
|
|
Persistent S2?
|
ASD, indicate R ventricular volume overload
|
|
|
Smoking and "5 A's"
|
23% of US adults smoke
ask, advise, assess, assist, arrange f/u |
|
|
Heart rate
|
-Adults normal 55-90
Children 1-2: 110 2-6: 100 6-10: 95 |
|
|
5 korotkoff sounds
|
1) 1st tapping noise (systolic)
2) soft lung sounds 3) louder sounds 4) muffled sounds 5) disappeared sound (diastolic) |
|
|
BP cuff
|
-should be 40% of arm width, 80% arm length
-2.5 cm over cubital space -too loose? will give low reading on small arm, high reading on large arm -too small: give high reading |
|
|
LOEx pulse much lower than upper extremity?
|
coarctation of the aorta
|
|
|
JVP
|
Reflects R atrial pressure which in turn reflects ventral venous pressure and R ventricular end diastolic pressure; use R internal jugular, bed at 30; biphasic (can see a and v waves), disynchonrous with arterial. Should be no more than 4cm above sternal angle
|
|
|
a,c,v waves
|
a- atrial contraction
c- AV valve closure v- ventricular contraction |
|
|
bruits
|
normal sounds of turbulence in kids, arterial obstruction in adults
|
|
|
PMI
|
5th intercostal space, MCL, 4-5cm from sternum
|
|
|
LSSB is what part of heart?
|
R ventricle
|
|
|
Erb's point
|
3rd intercostal space, can hear both aortic and pulmonary valves here
|
|
|
S1
|
-represents AV valves closing (end diastole early systole)
-Split can be heard best LLSB (M1 then T1) -high pitch -louder at apex than base |
|
|
S2
|
-closure of aortic and pulmonary valves
-split S2 can be heard on inspiration -louder at base than apex |
|
|
S1 path?
|
softer S1? mitral insufficiency, long PR, L ventric dysfunction
louder S1? mitral stenosis, short PR, high CO wide split S1- RBBB |
|
|
ejection click
|
opening of aortic or pulmonary valve, abnormally heard
Pulmonary- softer with ins LUSB Aorta- doest not alter with resp, RUSB and apex |