![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
133 Cards in this Set
- Front
- Back
|
What are the 3 Neurofirbomatosis disorders? |
1. Neurofibromitosis 1 2. Neurofibromitosis 2 3. Schwannomatosis |
|
|
What physical symptoms is neurofibromatsosis 1 characterized by?
|
Skin and bone abnormalities from tumors growing along the nerves.
|
|
|
What is neurofibromatosis 2 characterized by? |
Bilateral acoustic schwanomas Meningiomas Ependymomas (tumor arising from the lining of the ventricles)
(this type more directly affects the CNS) |
|
|
Which type of neurofibromatosis is most common? |
Type 1 IT IS AUTOSOMAL DOMINANT |
|
|
What are the diagnostic criteria for NF 1 (two of which need to be present for diagnosis)?
|

1. 6 or more cafe-au-lait macules on the skin
2. Two or more neurofibromas or one plexiform neurofibroma 3. Freckling of groin or axilla 4. Optic glioma 5. Two or more Lisch nodules (iris hamartoma) 6. A distinctive bony lesion 7. 1st Degree Relative with NF1 |
|
|
What percentage of people with NF 1 have tumors? What is the most common type? |
15% Benign Optic glioma (no cognitive impact) |
|
|
Which type of neurofibromatosis is most likely to cause seizures? |
Type 2 |
|
|
What MRI findings are common in NF 1?
|
T2 Hyperintensities (UBOs) are in the subcortical white matter, structures, and cerebellum
Found in 60-70% of NF 1 Patients |
|
|
Are the hyperintensities found in NF 1 associated with cognitive problems? |
Not often. |
|
|
How many NF 1 patients have Macrocephaly? |
30-50% |
|
|
What are the most common comorbid cognitive disorders in NF 1? |
Specific learning disorder (all types)
ADHD |
|
|
What is a neurofibroma? |
A benign nerve sheath tumor |
|
|
When do neurofibromas tend to flare up/increase during lifespan development? |
Puberty |
|
|
When during the life span do T2 hyperintensities resolve?
|
Young adulthood
|
|
|
Do cognitive symptoms worsen or improve over the lifespan of a person with NF1? |
Neither. If present, cognitive problems persist and cognitive strengths remain. |
|
|
How is FSIQ affected in NF 1? |
Average FSIQ is 89-98 Producing a "Leftward shift" |
|
|
What percentage of NF 1 have a learning problem? |
75% |
|
|
What are the most consistent cognitive deficits in NF 1? |
Attention and Dysexecutive Problems
Slowed processing speed
Visuospatial problems |
|
|
What Language problems are in NF 1? |
Higher level reading and writing
Verbal fluency |
|
|
What are common psychological and social problems in NF 1? |
Internalizing disorders (anxiety and depression)
Socially awkward at times. |
|
|
What cognitive domain is notably intact in NF 1? |
Verbal and visual MEMORY |
|
|
What is Tuberous Sclerosis Complex (TSC)?
|
An AUTOSOMAL DOMINANT NEUROCUTANEOUS disorder that affects multiple organ systems.
|
|
|
What are the most common neuropsychological disorders in TSC?
|
Autism
Intellectual disability
ADHD
|
|
|
How do cortical tubers affect the CNS? |
Disrupt the 6 layer structure of the cortex Focus of epileptiform activity |
|
|
What are the 3 neuropathological/structural findings in TSC?
|
1. Cortical tubers
2. Subependymal nodules
3. Subependymal Giant-Cell Astrocytomas (SEGA)
|
|
|
What are cortical tubers made of? |
Proliferation of glial cells and neurons. |
|
|
What are subependymal nodules? |
Hamartomas that form in the walls of the ventricles. |
|
|
What are SEGAs? |
Subependymal Giant Cell Astrocytoma |
|
|
What is the most common tumor in TSC? |
SEGA found in 10% of TSC |
|
|
How can SEGAs cause hydrocephalus?
|
Blocking the foramen of Munro |
|
|
What percentage of TSC patients have epilepsy? |
90% |
|
|
What percentage of TSC patients are diagnosed with either/or ID, Autism, or ADHD? |
50% |
|
|
Do cognitive problems progress in TSC? |
No. Like in NF 1, you keep what you have. |
|
|
What are the most common neuropsychological deficits in TSC? |
Attention and Dysexecutive problems
Problems with higher language functioning (e.g., abstract language, grammar, expressive vocabulary)
(Just like NF 1) |
|
|
What is the distribution of FSIQ like in TSC? |
BIMODAL 30% have profound ID 70% have normal IQ, but learning disability |
|
|
What type of emotional problems can be seen in TSC? |
Externalizing behavioral problems
Outbursts, Tempers, self injury |
|
|
What is the key feature of Sturge-Weber Syndrome? |

Port wine stain |
|
|
What neural abnormalities are present in Sturge-Weber Syndrome? |
Leptomeningeal Angiomas (Vascular Malformation) |
|
|
In which lobes are vascular malformations often found in Sturge-Weber? |
Parietal and Occipital Usually on the same side of the Port Wine Stain |
|
|
What is the correlation between the size of the Port Wine Stain in SWS and risk of brain involvement? |
Positive. Any port wine stain also increases risk of brain involvment 10-20% |
|
|
In addition to Leptomeningeal Angiomas, what other neurological abnormalities are seen in Sturge-Weber Syndrome? |
Cerebral atrophy and Calcifications in the parietal and occipital lobes.
|
|
|
What percentage of people with Sturge-Weber have seizures? |
75% |
|
|
What are common neuropsychological disorders in Sturge-Weber Syndrome? |
Intellectual disability that worsens with calcification, atrophy, and vascular events
Focal problems associated with vascular events and locations |
|
|
Does neuropsychological impairment progress in Sturge-Weber Syndrome? |
YES (unlike NF 1 and TSC).
Progresses with worsening seizures or vascular events. |
|
|
Who has a worse prognosis in SWS, younger or older patients? |
Younger. Those with seizures before before 6 months are at the highest risk. |
|
|
What is the most common type of behavioral problems in SWS?
|
Externalizing behavior problems, like ODD.
Depression is also seen, too, in cognitively intact people. |
|
|
What is the key physical feature of Williams Syndrome? |

Elf-Like Facial Features. |
|
|
What are the 4 structural CNS abnormalities in Williams Syndrome?
|
1. Reduced white matter resulting in Cerebral Volume loss with normal Cerebellum (i.e., gray matter is preserved)
2. Corpus Callosum is thinned
3. Abnormal cell density in Visual Cortex
4. Reduced Sulcal Depth in Intraparietal and Occipitoparietal Sulcus |
|
|
What structure has reduced activation in Williams Syndrome? |
Amygdala |
|
|
What are common neuropsychological problems in Williams syndrome? |
Visuospatial Dorsal Stream Problems (from Intraparietal/Occiptoparietal changes and Cell Density in Visual Cortex)
Hypersensitvity to threats and noise (due to amygdala abnormalities)
Intellectual disability
ADHD |
|
|
What is unusual about language development in Williams Syndrome? |
It's delayed by 2 years, but then is on par with peers.
They are known as "talkers" and hypersocial
They use single words before they learn to point |
|
|
What sensory motor problems are most prominant in Williams Syndrome? |
Sensorineural hearing loss.
Hoarse voice from connective tissue abnormalities |
|
|
In what skill are Williams Syndrome patients savants? |
Musical Skill.
They have a huge affinity for music, with amazing skills for Pitch and Timbre
|
|
|
What is the average FSIQ in Williams Syndrome? |
55 |
|
|
Are verbal or non-verbal skills stronger in Williams Syndrome? |
Verbal skills Non-verbal skills are affected by disruption of dorsal stream. |
|
|
What is the hallmark cognitive deficit in Williams Syndrome? |
VISUOSPATIAL PROBLEMS |
|
|
What are conversational stereotypies? |
Repetitive use of phrases in conversation. Often seen in Williams Syndrome |
|
|
What are the key physical defects of 22q11.2 deletion syndrome?
|

Cardiac defects in the heart and aorta
Cleft plate, long face, small ears, narrow eyes, pear shaped nose.
|
|
|
What are common neuropsychological disorders in 22q11.2 ? |
Borderline IQ Learning problems related to math |
|
|
What are the key neuropsychological deficits in 22q11.2 Deletion Syndrome?
|
POOR FACIAL MEMORY
VISUSOSPATIAL DEFICITS
INATTENTION ACROSS MODALITIES
DORSOLATERAL EXECUTIVE FUNCTIONING
MATH PROBLEMS
(Think nonverbal learning disability)
|
|
|
What neuropsychological abilities are relative strengths in 22q11.2? |
Verbal and Language abilities Verbal Memory Memory for rote information, not stories |
|
|
What is the most unique psychological/behavioral disorder in 22q11.2 deletion? |
Schizophrenia!
25 times more likely to develop schizophrenia/psychotic symptoms
|
|
|
In addition to schizophrenia, what other behavioral features are seen in 22q11.2 deletion syndrome? |
Flat affect
Specific fears and Separation Anxiety
Obsessions with some compulsions |
|
|
Describe developmental language delays in 22q11.2 Deletion Syndrome. |
Non verbal until age 3 Poor higher order language and pragmatics forever, even after language improves and develops |
|
|
What is Adrenoleukodystrophy? |
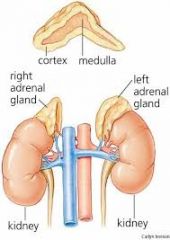
The answer is in the name...
Degenerative disorder affecting CNS myelin and adrenal cortex. |
|
|
What is the neuropathology of Adrenoleukodystrophy?
|
Accumulation of Very-Long-Chain-Fatty-Acid in plasma, brain, and adrenal cortex
|
|
|
What is life expectancy after diagnosis of Adrenoleukodystrophy? |
2-5 years once cerebrum is involved. Rapid neurodegenerative disorder |
|
|
What type of genetic disorder is Adrenoleukodystrophy? |
X-linked recessive (i.e., guys are screwed more often) |
|
|
What is the most common (i.e., classic) form of Adrenoleukodystrophy called? |
Childhood cerebral ALD 1/3 of all cases |
|
|
What age range is is Childhood Cerebral ALD typically diagnosed in? |
3-10 year olds |
|
|
Where in the brain is inflammatory demyelination seen in Andrenoleukodystrophy? |
Splenium of the Corpus Callosum back to the Parieto-occipital Cortex |
|
|
Describe progression of cognitive deficits in Adrenoleukodystrophy.
|
Normal development until diagnosis at age 3-8
1st Problems: Like ADHD
2nd Problems: Non-verbal and visuospatial skills.
3rd Problems: Executive dysfunction. Followed by a cascade affecting all cognitive functions.
Patients are minimally responsive in 2 years.
|
|
|
What are psychiatric signs seen in adults who develop Adrenoleukodystrophy? |
Mania and psychosis...often predate motor symptoms by years. |
|
|
What type of motor problems do adults with Adrenoleukodystrophy have? |
Gait disturbance Upper motor neuron problems (i.e., spasticity, babinski, weakness, pronator drift) |
|
|
What is Klinefelter Syndrome? |
MALE aneuploidy (i.e., abnormal number of chromosomes) from XXY sex chromosome. |
|
|
What are the key physical features of Klinefelters? |
1. Hypogonadism
2. Fertility problems
3. Tall Stature
|
|
|
What are the core CNS structural features of Klinefelters? |
1. Reduced overall brain volume
2. ********Greater left than right Temporal Lobe reduction*********
3. Less lateralized language (not really a structural finding, but needs to be said) |
|
|
What are the most common neuropsychological disorders in Klinefelters? |
ADHD
Dyslexia
Small number are also diagnosed with Autism
|
|
|
At what point in lifespan development do the features of Klinefelters become most prominent ? |
Puberty |
|
|
What are neuropsychological patterns for Klinefelters?
|
Average FSIQ
Nonverbal STRONGER than verbal (especially in childhood)
Reduced fine motor speed and Dexterity
|
|
|
Common psych problems in Klinefelters? |
Anxiety and depression |
|
|
What type of genetic inheritance does sickle cell anemia have? |
Autosomal Recessive (i.e., 25% risk if 1 parent has disease; 50% if both parents have it) |
|
|
What is the course of neuropsychological symptoms in sickle cell anemia? |
Variable |
|
|
At what age is is sickle cell anemia identified?
|
4 months
|
|
|
What is a sickle cell "crisis"? |
Sudden pain attack throughout the body that lasts for hours. |
|
|
What is often the first sign of sickle cell in infants? |
Swelling and pain in the hands and feet |
|
|
What is the primary neuropathology of sickle cell disease? |
Microvascular cerebral lesions accumulating over time. Sometimes large infarcts. |
|
|
What is the course of cognitive deficits in sickle cell?
|
Arrested academic skill development or frank regression
Depends on lesion load and location. |
|
|
What two types of cognitive deficits are very very unlikely in childhood cognitive disorders? |
Frank Aphasia Frank Amnesia |
|
|
What pattern of inheritance is PKU? |
Autosomal recessive |
|
|
What race is at highest risk for PKU? |
Whites |
|
|
What are the late cognitive deficits in PKU patients that get treated early for the condition? |
Attention/Dysexecutive, Verbal Fluency, Word retrieval, Memory
Normal general cognitive functioning
|
|
|
What cognitive disorder presents if PKU is severe or not treated? |
Intellectual disability
|
|
|
What is typically affected in childhood cognitive disorders, white matter or gray matter? |
White matter, by far. |
|
|
What is Turner Syndrome? |
A disease affecting girls because of a missing X chromosome |
|
|
What are key physical features of Turners? |

Webbed neck Short Stature |
|
|
What CNS structural changes are seen in Turner's?
|
Abnormal amygdala, orbitofrontal, cingulate, insula, and ventromedial PFC (LIMBIC system takes a hit)
Reduced parieto-occipital cortex.
Agenesis of Corpus Callosum. |
|
|
What is the most common learning disorder in Turner's? |
Math, Math, Math, MATH!! Key deficit
ADHD
|
|
|
What are key neuropsychological deficits in Turner's |
Social cognition
MATH
Motor skills
VISUOSPATIAL (like almost everything) |
|
|
What is Fragile X Syndrome? |
A >200 CGG repeat on an X chromosome
MEANS IT AFFECTS MALES MORE |
|
|
What is the the leading cause of inherited ID and leading gene disorder associated with autism? |
Fragile X Syndrome |
|
|
What are the CNS structural findings in Fragile X? |
Enlarged Hippocampus, Caudate, Thalamus, Amygdala Reduced Vermis |
|
|
What other type of epilepsy do seizures in Fragile X look like? |
Benign Rolandic Epilepsy It also resolves in childhood |
|
|
What chromosome is implicated in Prader-Willi Syndrome? |
15 |
|
|
What is the hallmark symptom of Prader-Willi? |

Hyperphagia |
|
|
What are key physical features of Prader-Willi? |
Hypotonia
Hypogonadism
Short stature
Obesity |
|
|
What is the key cognitive disorder in Prader-Willi? |
Mild to Moderate ID
|
|
|
What psychiatric disorder is often seen in Prader-Willi? |
Obsessive and compulsive behavior |
|
|
What is the cognitive profile in Prader-Willi?
(Hint: there is a striking difference in which domains are typically affected in kids) |
Different that most genetic diseases!!! Language is weak while visuospatial is relative strength.
Mild to Moderate ID
HYPOTONIA THROUGHOUT LIFE |
|
|
How are Prader-Willi and Angelmann Syndrome alike? |
The are both due to a lack of gene expression on chromosome 15.
Prader-Willi is paternal
Angelmann is maternal |
|
|
Are seizures more common in Prader-Willi or Angelman? |
Angelman with 90% having seizures. |
|
|
Besides epilepsy, what are neurological signs of Angelman? |
MOTOR WEIRDNESS
Ataxia
Tremulous limb movement/Hyperkinesis
Sensory seeking behaviors
Stereotyped behaviors (hand flapping, etc) |
|
|
Like Prader-Willi, what is the key neuropsychologial deficit in Angelman? |
SEVERE SPEECH LANGUAGE DELAYS (like Prader-Willi, but more severe) |
|
|
What is behaviorally unique about Angelman patients? |

HAPPY, HAPPY, HAPPY!
Easily excited with hand flapping
Excessive laughter |
|
|
Name the autosomal disorders |
1. Downs Syndrome 2. Prader-Willi 3. Angelman 4. Williams 5. PKU 6. Spina bifida cystica 7. NF1 (dominant) 8. Sickle cell (recessive) 9. TSC (dominant)
|
|
|
Name the sex-linked disorders.
|
1. Turners 2. Klinefelters 3. Fragile-X 4. Rett's 5. XYY 6. Adrenoleukodystrophy |
|
|
Name the neurocutaneous disorders |
1. Tuberosclerosis 2. Neurofibromatosis 3. Sturge-Weber 4. Ataxia-Telangiectasia |
|
|
What is cranium bifidum? |
Incomplete closure of the skull that leads to a bubble full of CSF on the head. |
|
|
What is anencephaly? |
Lack of cranial vault. Brain is usually a vascular mass. |
|
|
What is a Dandy-Walker malformation? |
When the posterior portion of the upper neural tube fails to develop. RESULTS IN CEREBELLUM AND MEDULLA staying in EMBRIONIC STAGE |
|
|
What are signs of Dandy-Walker? |
HYDROCEPHALUS Agenesis of the Corpus Callosum Macrocephaly |
|
|
What are symptoms of Dandy-Walker |
Mental retardation
PSYCHOMOTOR RETARDATION |
|
|
What is an Arnold Chiari Malformation? |
When the cerebellum and medulla develop too low and go down through foramen magnum. |
|
|
What condition does Arnold Chiari Malformations produce in kids? |
Congenital hydrocephalus Psychomotor retardation |
|
|
What symptoms might adults with hydrocephalus report if they are "asymptomatic"? |
Bulbar Palsy Neck pain Headaches |
|
|
What is spina bifida occulta? |
An asymptomatic abnormal fusion of the lumbar vertebrae. |
|
|
What are the two types of spina bifida cystica? |
Meningocele (less common) Meningomyelocele (far more common) |
|
|
What is spina bifida meningomyelocele? |
Tangle of rudimentary lumbar and sacral spinal cord with meninges protruding into a sac. |
|
|
What condition is most associated with meningomyelocele? |
Chirai malformations causing hydrocephalus |
|
|
What are common cognitive symptoms of meningomyelocele? |
Mental retardation Psychomotor Retardation |
|
|
What is hydranencepahly? |
When the hemispheres are replaced with CSF filled sacks Leads to death |
|
|
What is Porencephaly? |
When bilateral massive cysts develop in the hemisphere
Gyri often from radial pattern around cysts. |
|
|
What causes focal dysplasia (heterotopies)? |
Disruption of neuroblast migration Patients have LD and epilepsy |