Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
86 Cards in this Set
- Front
- Back
|
function of vWF ?
|
activates platelet aggregation
|
|
|
vWF released during primary or secondary hemostasis?
From where? |
primary (platelet plug formation)...released from damaged subendothelial cells
|
|
|
Is fibrin accumulation part of primary or secondary hemostasis?
|
secondary
|
|
|
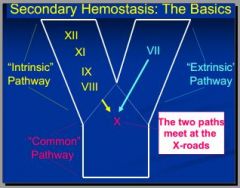
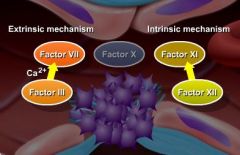
what 3 pathways of secondary hemostasis?
|
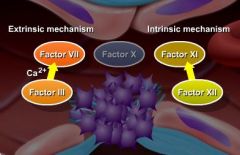
1. extrinsic
2. intrinsic 3. common |
|
|
Which secondary hemost. pathway is plasma based and slow?
|
INTRINSIC
*gets name b/c factors originate from "inside" vessel! PIS (plasma intrinsic slow) |
|
|
Which pathway (intrinsic or extrinsic) of clot form. is faster and more powerful?
|
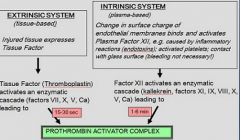
EXTRINSIC SYSTEM (tissue-based)
is only 15-30 second long. ~in contrast, Intrinsic system (plasma-based) takes 1-6 min E_ Too Fast |
|
|
Which secondary hemost. pathway is tissue based and rapid?
|
extrinsic
|
|
|
Which pathway includes F11,12 contact factors b/c activated by contact with other factors INSIDE injured blood vessel??
(also factors 8,9 involved) |
intrinsic (plasma based and slow)
"Why stay inside (intrinsic) and pay $11.98 or $12, when can go outside (extrinsic) and pay only $7?" |
|
|
Which pathway includes factors 10,5,2,and 1?
|
common
hint: divide each factor by 2 to get next one |
|
|
What happens during common pathway?
|
converts prothrombin to thrombin & forms cross- linked fibrin
(where 2 arms of Y come together) |
|
|
4 parameters for testing Hemostasis
|
1. Platelets counts
2. (Mucosal) Bleeding Time / in vivo 3. OSPT = 1 Stage Prothrombin Time 4. APTT = Activated Partial Thromboplastin Time |
|
|
APTT stands for?
measures ? normal APTT time? |
- Activated Partial Thromboplastin Time (name doesn't make a whole lot of sense, b/c thromboplastin is TF of extrinsic system)
- measures INTRINSIC and common pathway expected time 60-120 sec AI |
|
|
OSPT stands for?
measures ? normal OSPT time? |
OSPT = One Stage Prothrombin Time
-> measures EXTRINSIC and common pathways (expected time < 10 sec!) OE memory trick: Obama Elected '10 (2010) |
|
|
The INTRINSIC SYSTEM is plasma-based pathway. During first stage of clot formation, WHAT FACTOR is activated initially by change in surface charge of endothelial membranes?
What are some stimuli/injuries that can stimulate this? Is bleeding always involved? |
Change in surface charge of endothelial membranes activates **Plasma Factor XII**
e.g. caused by inflammatory reactions (endotoxins); activated platelets; contact with glass surface (bleeding not necessary!) |
|
|
Is Factor XII a plasma or platelet factor?
F12 activates a cascade of enzyme involved in intrinsic pathway. Name these 3 enzymes. |
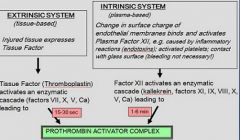
Plasma Factor, of plasma-based INTRINSIC SYSTEM
*activates an enzymatic cascade factors XI, IX, VIII of intrinsic then continues onto common pathway |
|
|
What is another name for Thromboplastin?
What pathway is it part of? Function? |
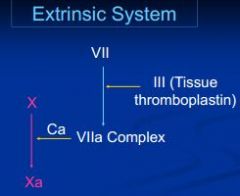
Tissue Factor (TF3) aka Factor 3 --> of EXTRINSIC PATHWAY = unique b/c released by injured tissue outside circulation e.g. subendothelial cells
>once reaches plasma, quickly binds to factor 7 + calcium then enzymatic cascade continues onto common pathway (X, V, Ca) leading to PAC |
|
|
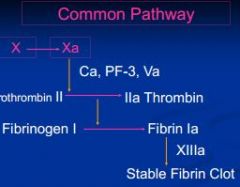
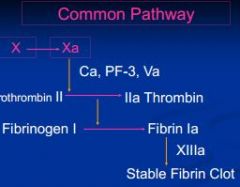
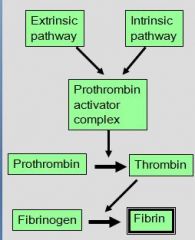
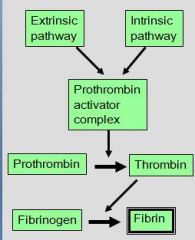
COMMON pathway begins when ?
|
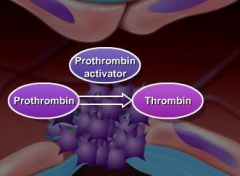
EXTRINSIC and/or INTRINSIC pathway, each produces unique factors capable of activating Prothrombin-Activator Complex.
COMMON pathway begins with Factor X (along with Factor 5) form Prothrombin-Activator Complex which converts Prothrombin (F2) to Thrombin (F2a) (represent merger of ext/intrinsic pathways) |
|
|
Again name 4 factors of common pathway!
|
10 (hageman factor),
5, 2 (prothrombin), 1 (fibrinogen) |
|
|
APTT measure?
what is contact activator added to tube/sample? what factors added? expected time? |
APTT = Activated Partial Thrombo- plastin Time
- measures INTRINSIC and common pathway <- measures clot formation after clean venipuncture in citrated tube and addition of contact activator (diatomaceous earth), Platelets Factors and Calcium (expected time 60-120 sec) A60 |
|
|
OSPT
expected time? what is added? |
1 Stage Prothrombin Time:
-> measures EXTRINSIC and COMMON pathways (expected time < 10 sec) - measures clot formation in citrated plasma after addition of Tissue Factor, Platelet Factors and calcium One 10 |
|
|
Which is tissue-based pathway during stage 1 of clot formation?
|
EXTRINSIC SYSTEM: comes from outside blood vessel, membrane disrupted
Injured tissue expresses Tissue Factor (factor 3) |
|
|
(Mucosal) Bleeding Time
what does it test? |
TESTS PLATELET PLUG FORMATION (not clotting)
*stop time until bleeding stops after standardized small incision into skin or mucosa (expected time 1-5 min) -> measures functional ability of platelets and vMF to plug minute injuries |
|
|
What is Tissue Factor?
What is it part of? What does it activate? |
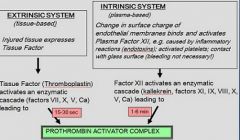
Injured tissue Factor (Thromboplastin), of extrinsic pathway, activates an enzymatic cascade (factors VII, X, V, Ca) leading to P.A.C
note: extrinsic comes from outside blood vessel, membrane disrupted |
|
|
Which is most important enzyme of clot formation depends relies of vitamin K?
Name Vit K antagonist..what does it cause? |
Factor 7 (most important, b/c shortest HL so conseq. of absence apparent sooner), Prothrombin
Coumarin = Vit K antagonist -> impairs liver synthesis of several clotting factors incl. Prothrombin |
|
|
SYNTHESIS of prothrombin, a hepatic alpha globulin, is dependent on ? (~two words)
Attaches itself to ? |
- its liver synthesis is **VITAMIN K** dependent (was not asking about activation!)
-attaches itself to activated platelets |
|
|
What polymerize into long fibers and X-link into meshwork w/i and around the platelet plug?
Bonus: what is time frame? |
FIBRIN, this meshwork = STABLE CLOT
-> bleeding stops (within 3-6 min after injury) |
|
|
How is FIBRIN formed?
|
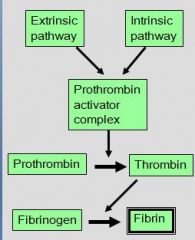
Thrombin hydrolyses FIBRINOGEN (=hepatic soluble protein; already bound to activated platelets) into FIBRIN monomers
|
|
|
The INTRINSIC SYSTEM is plasma-based pathway. During first stage of clot formation, WHAT FACTOR is activated initially by change in surface charge of endothelial membranes?
What are some stimuli/injuries that can stimulate this? Is bleeding always involved? |
Change in surface charge of endothelial membranes activates **Plasma Factor XII**
e.g. caused by inflammatory reactions (endotoxins); activated platelets; contact with glass surface (bleeding not necessary!) |
|
|
CLOT RETRACTION
|
W/i the next 30 minutes after stable clot (fibrin meshwork around plug), platelets contract more and pull fibrin threads together
-> clot tightens and pulls edges of injured blood vessel together |
|
|
Fibrinolysis
what is it? time rame? enzymes involved? |
Hemostasis: Fibrinolysis = removal of clot (1-2 days after clot formation)
tissue-Plasminogen Activator = tPA activates hepatic plasma factor Plasminogen to PLASMIN = proteolytic enzyme - plasmin nibbles at fibrin fibers |
|
|
PLASMIN
|
PLASMIN = proteolytic enzyme
- plasmin hydrolyses fibrin fibers + clotting factors! into FDPs (Fibrin Degradation Products); |
|
|
FDPs are removed by
|
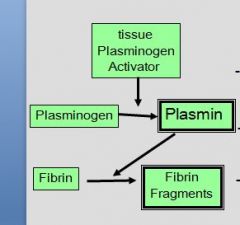
Fibrin Degradation Products are removed by macrophages
|
|
|
- _____ inhibit platelets adhesion
- secreted by ?? |
PROSTACYCLIN and Nitric Oxide -> inhibit platelets adhesion
secreted by intact endothelial cells and WBC |
|
|
What limits fibrin formation and positive feedback?
|
Fibrin binds Thrombin -> limits fibrin formation and positive feedback
(remember normally thrombin hydrolyzes fibronogen to form fibrin monomers, as well as +f/b of int/ext.systems) |
|
|
* ANTI-THROMBIN III
* ______from ____ combines with Anti-thrombin III and greatly augments its effectiveness |
ANTI-THROMBIN III (α globulin) deactivates Thrombin and other clotting factors
Heparin from Mast Cells / Basophils increases A-TIII's effectiveness |
|
|
In vitro anticoagulation
|
Calcium binding agents (e.g. citrate, oxalate, EDTA), heparin
|
|
|
In vivo anticoagulation
|
Heparin, Vit K antagonists, prostaglandin synthesis inhibitors (NSAIDs)
|
|
|
Why does calcium help with clotting?
|
Most clotting factors negatively charged, so Ca+2 helps bring in.
|
|
|
Thrombocytopenia
|
decreased production (bone marrow; drugs; FeLV) or increased destruction (immune-mediated) or consumption
|
|
|
von Willebrand’s Disease (Form I,II,III)
|
= most common bleeding disorder in animals due to genetic lack / insufficiency of vWF -> platelets fail to adhere to injury sites -> spontaneous bleeding (or ); clinical signs can be mild / severe / fatal; described in ca 60 breeds of dogs with highest
prevalence in Dobermans |
|
|
Vit K deficiency / Rodenticide poisoning
|
Coumarin = Vit K antagonist -> impairs liver synthesis of several clotting factors incl. Prothrombin
Causes hemorrhagic anemia, regenerative so macrocytic, hypochromic, reticulocytes up, PP down, APTT prolonged, OSPT prolonged |
|
|
Thrombopoietin
|
Hormone produced mainly by liver and kidney that regulates production of platelets by bone marrow; stimulates production and differentiation of megakaryocytes, the bone marrow cells that fragment into large numbers of platelets
|
|
|
primary hemostasis
|
blood vessel constriction & platelet aggregation/adhesion
|
|
|
secondary hemostasis
|
coagulation cascade
When clot has stopped bleeding & blood vessels repair, tertiary hemostasis ->fibrinolysis -> perfusion restored. |
|
|
tertiary hemostasis
|
fibrinolysis --> perfusion restored.
|
|
|
T/F: Usually 70-80% clotting factor/platelet loss is needed to cause bleeding - may occur spontaneously – may occur after minor injury eg teething, minor trauma or surgery
|
True: Usually 70-80% clotting factor/platelet loss is needed to cause bleeding
|
|
|
T/F Coagulopathy is possibly hereditary in young animals
T/F: Coagulopathy can be acquired in older animals, from exposure to drugs or poisons |
True : Coagulopathy is possibly hereditary in young animals, & possibly acquired in older animals, from exposure to drugs or poisons – do check history carefully.
|
|
|
12,11,9,8 part of?
|
intrinsic
|
|
|
Factor 1 =
|
F1 = prothrombin
|
|
|
Factor 4 =
|
F4 = calcium
|
|
|
kind of tube used for coagulation test (OSPT/APTT)?
|
Sodium citrate (blue)
|
|
|
kind of tube used for coagulation test for platelet count?
|
EDTA (purple)
|
|
|
prolonged OSPT indicates?
|
Problem with extrinsic pathway:
Vitamin K problem, advanced liver disease, or DIC |
|
|
prolonged APTT indicates?
|
deficiency of factors VIII & IX, by heparin toxicity, angiostrongylus infestation and rarely by liver disease
|
|
|
If the mean platelet volume is raised, what could this indicate?
|
increased platelet production, especially in immune mediate thrombocytopenia
|
|
|
What is a crude test for platelet function and helps to detect thrombocytopathy?
|
clot retraction time
|
|
|
What does increased values of fibrinogen assay indicate?
|
inflammation in large animals, especially cattle
|
|
|
If clot lysis test results in lysis of clot in less than 24 hrs. than indicates?
|
excess plasmin
|
|
|
A defect in what tends to cause capillary bleeding with petechiae & ecchymoses in skin or mucosa over a period of time?
|
primary hemostasis
|
|
|
A defect in what tends to cause sudden, often severe bleeding into muscles, body cavities, eyes or joints, or into the gut or urinary or respiratory tract?
|
secondary hemostasis
|
|
|
What are the most common cause of coagulopathies?
|
platelet disorders and rodenticide poisoning
|
|
|
What syndrome occurs when severe inflammation or endotoxemia, necrosis, neoplasia, septicemia, viremia, or parasitemia, damage blood vessels, strip endothelium & bare the underlying collagen & cause multiple thrombi?
|
disseminated intravascular coagulation
|
|
|
What is the diagnostic test of disseminated intravascular coagulation?
|
Fibrin Degradation Products present
FDPs formed plasmin digests fibrin; incr. fibrinolyisis indicates incr. coag.! |
|
|
Vitamin K is essential in production of what factors?
|
2,7,9, and 10 (7 is the most important and has short HL)
|
|
|
What is usually caused by ingestion of warfarin and other rodenticides (brodifacoum and "storm")?
|
vitamin K deficiency
|
|
|
How would vitamin K defic. be diagnosed?
|
prolonged OSPT, defic. in factor 7, mild prolongation of APTT and ACT tests
|
|
|
What factor affected in hemophilia A in dogs, cats, and horses?
|
factor 8
|
|
|
deficiency in christmas factor in dogs and cats refers to what clotting factor?
|
factor 9
|
|
|
What factor defic. occurs in friesian cattle and dogs?
|
factor 11
|
|
|
What animals does the Hagemann Factor (factor 11) occur in?
|
cats
|
|
|
For emergencies (horse with major blood loss) where don't know blood type, what blood groups should DONOR be negative for?
|
Aa and Qa negative
but i thought horses don't develop alloantibodies (Ab to blood/tissue for other of same species)??? |
|
|
These animals have 11 blood groups, but B & J are most important. Transfusion reactions are rare but it is best to give blood from a J-negative animal?
|
cows
|
|
|
What animals have 8 blood types, but DEA 1.1 and 1.2 are the most antigenic, also have no naturally occuring antibodies, so first transfusion without X matching should be safe?
|
dogs
|
|
|
cats have what blood groups?
which type develops strong allo-ab against the other? |
has blood groups A, B, and AB (rare).
B has strong Anti-A alloantibodies, (A has weak anti-B alloantibodies) |
|
|
In America >95% of cats are in what blood group? Europe?
|
A in US; in Europe most cats are group B
|
|
|
What breeds of cat are more likely to be bloodgroup B? (4)
|
abyssinian, birman, maine coon, persian
|
|
|
How often can dogs donate blood?
|
every 3-4 weeks
(15 ml / kg BW each time) ~300 ml |
|
|
Describe an ideal equine donor?
What dz must be negative for? |
weight at least 1000 pounds, have normal PCV and plasma protein, tested for equine infectious anemia, and not have had a blood transfusion or a FOAL!
|
|
|
What should be given if there is severe edema?
|
albumin; PP loss in circ. leads to reduced osmotic pressure in vessels
|
|
|
Can transfuse blind in what species?
|
dog (except stray dogs) & cow,
|
|
|
What is caused by fungal proliferation on mouldy clovers, and releases a form of coumarin? Consequence of this?
|
"sweet clover" poisoning; Vit. K poisoning = bye bye factor 7
|
|
|
8.)Which of following most accurately describes function of tPA?
A. Inhibition of platelet aggregation B. Degradation of factors 5 & 8 C. Inactivates Thrombin, Plasmin, Kallekrein, and a few other clotting factors D. Catalyzes Plasminogen activation during fibrinolysis E. All of the above |
8. (D) is correct – tPA or tissue Plasminogen activator converts Plasminogen -> Plasmin -> degrades Fibrin -> releases FDPs!
Wrong answers: A. Inhibition of platelet aggregation by PGI2 and NO B. Degradation of factors 5 & 8 actually negative feedback from thrombin itself C. Are functions of ATIII |
|
|
6.)Which of following is NOT one of three most common causes of severe thrombocytopenia? (more than one answer possible)
A.IMTP B.Ehrlichia C. Disseminated intravascular coagulation (DIC) D. Anaplasma E. von Willebrand’s Disease |
D, E
|
|
|
4.) Which of following is most likely to get Hemophilia A?
A. Female doberman B. Male Jack Russell Terrier C. Female german sheperd D. Male springer spaniel |
4.) B. Male Jack Russell Terrier
- Sex-linked (males only) - Jack Russell Terriers - German shepherds |
|
|
True or False: ACT will always be prolonged if APTT is prolonged, but some animals with “normal” APTT have prolonged ACT.
|
False: Both ACT & APTT evaluate intrinsic & common clotting mechanisms. But APTT is MORE sensitive than ACT. (ACT only screening test.) Therefore, APTT will always be prolonged if ACT is prolonged.
|
|
|
Why might nephropathy lead to excessive coagulation elsewhere in body? (be specific)
|
Loss of Anti-Thrombin III thru glomerulus (PLN)
|