Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
71 Cards in this Set
- Front
- Back
|
which blood test indicates liver synthetic ability over a long-period of time (ie CLD), long half-life
|
albumin
|
|
|
what does an isolated rise in GGT indicate
|
alcohol
|
|
|
what cause must you consider in all abnormal LFTs
|
drugs
|
|
|
what blood tests specific for:
- wilson's disease - haemochromatosis - a1-antitrypsin def |
- W: Cu & caeruloplasmin
- ferratin / trandferrin - a1-antitrypsin |
|
|
what blood tests specific for:
- autoimmune hep - PBC - PSC |
autoimmune hep: ANA, SMA, LKM-1
PBC: AMA (M2), IgM PSC: ANA, SMA |
|
|
important q's to ask in hx
|
stool & urine colour
SH:travel, transfusions, tattoos - occupation, unprotected sex, alcohol, smoker DH: OTC (inc paracetamol), herbal, illegal, supplements, steroids FH PMH: DM, hyperlipidaemia, interventions (ERCP), mumps, scorpion, |
|
|
what to look for on GENERAL (inspection) on examination (GI)
(i.e. not hands and stuff) |
nutrition (BMI), scars, distension (local/general), deformities, distended veins (caput medusa, JVP), masses, pulsations (AAA)
feverish, pallor, anaemia/jaundice. |
|
|
signs of liver disease on examination
|
spider naevi, palmar erythema, gynaecomastia
liver FLAP clubbing leukonykia (hypoalbuminaemia) jaundice/ anaemia low/ high BMI ascites/ caput medua hepatosplenomegaly ENCEPHALOPATHY |
|
|
what to look for on the hands in GI examination
|
clubbing /koilonykia
leukonykia nicotine stain palmar erythema liver flap pulse |
|
|
what's first line therapy for variceal/ upper GI bleeding
|
ABC & resuscitate (IVI)!!
ENDOSCOPY: - sclerotherapy - banding - glue CT- during active bleed |
|

what element used to treat angiodysplasia of the oesophagus via endoscopy
|
ARGON
|
|
|
ways of treating oesophageal strictures
- benign - malignant |
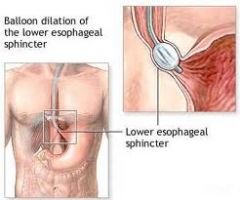
DILATATION (balloon eg for achalasia)
STENT (malignancy) |
|
|
what procudure used to remove intralumenal objects (eg gallstones)
|

ERCP- SPHINCTEROMETRY
|
|
|
first line Ix for cholecystitis
2nd line |

★USS★- ?dilated BD?
stones- ERCP no dilated BD--> MRCP |
|
|
tests/ Ixs for pancreatitis
|
↑amylase
USS- exclude GS, assess obstruction/ complications (eg pseudocyst) ★CT★ |
|
|
Ixs for suspected perforation
(general/ localised peritonism, systemic fever, shock, infection) |
★CXR★- subdiaphragmatic air
CT- source, gas/fluid |
|
|
first line Ix for appendicitis
|
★USS★- more useful in children, exclude other causes
|
|
|
Ixs for diverticulitis (inflammation of diverticulosis)
|
★PR EXAM★
inflam markers: WCC, CRP AXR Ba enema sigmoidoscopy/colonoscopy ★CT★ |
|
|
first line Ix for distended abdomen
|
★AXR★
- ?small or large bowel - ?gas or fluid - ?volvulus/ ileus USS- fluid CT- cause |
|
|
ALARM symptoms for dyspepsia
|
dysphagia
GI blood loss (anaemia, haematemesis) persistent vomitin wt loss mass |
|
|
Ixs for dysphagia with alarm symptoms (3)
|
★H.pylori★ C-urea breath test
★ensoscopy★ +/- biopsy Ba swallow |
|
|
Ixs for change in bowel habit
|
★PR exam★
ba enema ★sigmoid-/ colon-soscopy★ AXR CT ?Chron's- white-cell scan |
|
|
Ixs for jaundice
|
BLOODS- FBC, U&Es, LFTs, CRP, virology, immunology, auto-abs
★USS★ - ?bile ducts dilated= post-hepatic - ? mets -? cirrhosis - ?ascites ?biopsy MRCP +/- ERCP CT |
|
|
what mneumonic used to think of differentials
|
VINDICATE
Vascular Infection Neoplasm Drugs Inflammatory Congenital Auto-immune Trauma Endocrine |
|
|
what organs/ structures likely to cause epigastric pain
|
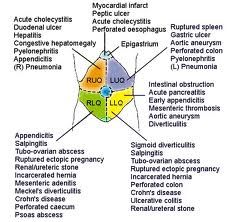
heart, oesophagus, stomach, duodenum, GB, bile ducts, liver, pancreas
|
|
|
organs/ structures likely to cause RUQ pain
|
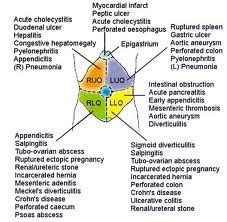
liver, GB, bile ducts, duodenum, PNEUMONIA!
|
|
|
organs/ structures likely to cause LUQ pain
|
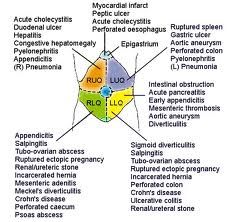
pancreas, stomach, splenic flexure (abscess, infarct), spleen, stomach, PNEUMONIA!
|
|
|
organs/ structures likely to cause central abdo pain
|
early appendicitis, pancreas, bowel, transverse colon
|
|
|
organs/ structures likely to cause RLQ
|
appendicitis, Chron's, colonic ca, ascending colon, (r.ovary & fillopian tube)
|
|
|
organs/ structures likely to cause LLQ pain
|
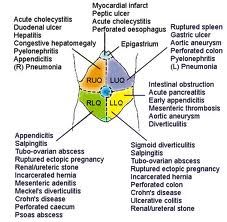
diverticulitis, colorectal / sigmoid ca (descending colon), colitis (likely ischaemic), ovary
|
|
|
apart from GI causes, what other systems must you consider in a pt presenting with abdominal pain
|
GU, repro
|
|
|
baseline tests & initial management of pt with an acute abdomen
|
O2, IV fluids, Abx's if infection (eg peritonitis)
analgesia +/- anti-emetic BLOODS: FBC, U&Es, LFTs, amylase, CRP, ABG, cross-match ?transfusion urine ECG, CXR, AXR, USS |
|

what do skin changes (bruising/ darkening) indicate
|

intra-peritoneal haemorrhage
acute haemorrhaginc pancreatitis |
|
|
S&Ss og mesenteric ischaemia
- acute - chronic |
AF with;
1) ACUTE SEVERE abdominal pain - constant, central/RIF hypovolaemia: low BP, high HR 2) SEVERE colicky post-prandial pain, PR bleeding, wt loss COLONIC ischaemia- left sided pain, BLOODy D |
|

Ix & results for mesenteric ischaemia
|
↑WCC, ↑Hb (due to plasma loss), ↑lactate
METABOLIC ACIDOSIS ↓HCO3- AXR/ Ba enem- no gas, "thumb-printing" (submucosal swelling) CT ★ANGIOOGRAPHY★ |
|
|
causes of mesenteric ischaemia (4)
|
★AF!★
vasculitis trauma strangulation of hernia/ volvulus |
|
|
&Ss bowel obstruction
|
anorexia, nausea, VOMITING (bile-stained) - relief
COLICKY abdo pain (contsant in colon) DISTENTION constipation |
|
|
examination findings in bowel obstruction
|
high-pitched tinkling BS
distention w/o shifting dullness visible PERISTALSIS tenderness |
|
|
differentiate bowel obstruction from a strangulation
|
strangulation- more SHARP CONSTANT, localised, ?fever ? high WCC
obstruction- CENTRAL COLICKY |
|
|
Ixs for bowel obstruction
findings |

AXR: DISTENTION of gas PROXIMAL to obstruction
- SMALL b.: plicae (pic) - LARGE b.: haustra ?ba enema |
|
|
management/ treatment of bowel obstruction:
- incomplete - complete and strangulation |
INCOMPLETE: conservative
- IV fluids, NG tube + NBM, replace electrolytes COMP+STRANG: emergency surgery!!! |
|
|
causes of bowel obstruction (BATH VIPS)
|
BOLUS- food, faeceas, gallstone (impacted ileus)
Adhesions (congenital, iatrogenic) TUMOUR Hernias- strangulated Volvulus INTUSSUSCEPTION Pseudo-obstruction Strictures (chron's diverticulosis) |
|
|
causes of bowel distention
|
5F;s:
Fat Fluid Faeces Food Feotus |
|
ddx of rectal bleeding (7)
|
anal fissure
perianal haematoma colorectal polys/ ca diverticular disease proctitis (inflam anal canal + rectum)/ gastroenteritis IBD haemorrhoids |
|
|
S&Ss haemorrhoids (piles)
|
★PAINLESS★
FRESH blood PR perianal itching ★CONSTIPATION/ straining!!!!!★ anaemia (sometimes: mucus) |
|
|
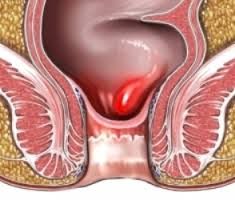
what are piles (haemorrhoids)
|
displaced & protuding rectal/ anal CAPILLARIES
- gravity, increased anal tone, straining prone to rupture & bleed (NB: not varicose veins) |
|
|
Ixs for haemorrhoids
|
★PR exam★- only prolapsing piles visible, internal piles NOT PALPABLE!!!!!
proctoscopy sigmoidoscopy |
|
|
management of haemorrhoids
|
high fibre diet
topical SCLEROSANTS band LIGATION 4th deg: haemorrhoidectomy |
|
|
rectal prolapse can be:
1) partial 2) complete - presentation S&Ss |
incontinence
protruding mass blood & mucus PR poor anal tone |
|
|
presentation S&Ss of anal fissure
|

fresh BLOOD
PAINFUL on defaecation constipation (holding back from pain) ITCH mucosal TAG |
|
|
3 mananagement options for anal fissure
|
increase dietary FIBRE
GTN ointment lateral sphincterotomy |
|
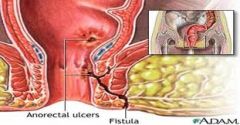
presentation S&Ss of anal FISTULA
|
BLOOD
MUCUS chron's TB Ca opening distal from site of anus |
|
|
causes of an abdominal mass
(don't thing just GI...also repro & GU) mneumonic: A CHEMICAL |
AAA
Chron's inflam Hernia Enlarged organ Malignancy Intussusception Cyst/ abscess Appendicitis Lymphadenopathy |
|
|
physical examination of a mass
|
shape, size
fluctuating (respiration/ palpation) rashes/ lesions/ colour pulsations character: smooth/ craggy, hard, soft tender percuss: gas, solid, liquid (shifting) BS? bruits (AAA) |
|
|
3 cardiac/ vascular complications post-op
|
haemorrhage
MI DVT/ PE |
|
|
3 GI complications post op
|
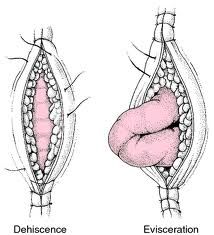
ileus
anastomotic dehiscence (pic) adhesions |
|
|
what's an ileus (complication post-op)
presentation (S&Ss) |
painful obstruction of ileum/ small intesting
PARALYSIS of motility ABSENT BS & peristalsis VOMITIN distention dehydration (need electrolytes correcting) |
|
|
presentation S&Ss (helpful hx) in suspecting adhesions
|
bowel OBSTRUCTION
vomiting, distention, constipation, abdo pain (colicky) "tinkling" BS/ absent prev abdo surgery |
|
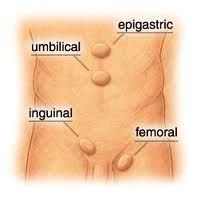
cause of hernias
main type |
natural opening/ weak/ defect in muscle wall area
stretching, surgery, increased abdominal pressure INGUINAL |
|
|
what does an irreducible hernia indicate
|
obstructed (bowel contents cannot move through)
or strangulated (blood supply compromised) - risk gangrene if arterial supply compromised |
|
|
what type of people at risk of femoral hernias
|
old, thin FEMALES (x10 more common than M)
|
|
|
what structure lies anterior and lateral to femoral canal
|
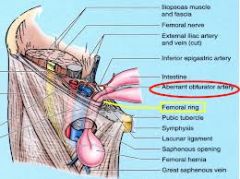
anterior: inguinal lig
lateral: femoral vein |
|
|
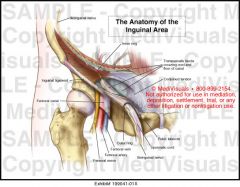
relation to inguinal canal:
- floor -roof - anterior - posterior - medially |

FLOOR: inguinal lig
ROOF: transversalis fascia & internal oblique ANT: external oblique anponeurosis POST: transversalis MEDIAL: conjoint tendon |
|
|
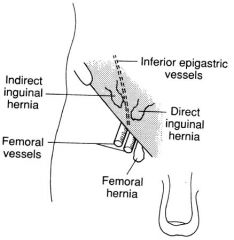
differentiate an indirect & direct inguinal heria
- anatomically - clinically |
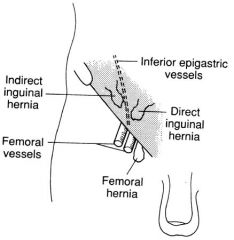
INDIRECT; lateral to inf epigastric vessels, through inguinal canal --> scrotum
DIRECT: medial to inf epi vessels, directly through wall. REAPPEARS with cough test |
|
|
what point is 1/2 way between pubic tubercle and ASIS
|
DEEP inguinal ring
|
|
|
which type of inguinal hernia better controlled with digital pressure
|
indirect hernia
|
|
|
what layer does the processus vaginalis take from the soma wall, what does it subsequently become
|
from the parietal peritoneum
descends ahead of the testis into the scrotum becomes the tunica vaginalis |
|
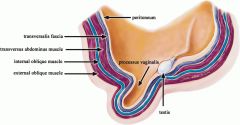
in the male, what layers of the abdominal wall does the testis descend through, which does it take into the scrotum
|
parietal peritoneum--> tunica vaginalis (doesn't surround testis, lies in FRONT)
transversalis fascia --> internal spermatic fascia transversus abdominus (not taken) internal oblique--> CREMASTER muscle external oblique APONSEUROSIS --> external spermatic fascia |
|
|
what structure if formed by joining of internal oblique and transversus abdominus, connecting these muscles to the pubic tubercle. Lateral to the inguinal canal
|
conjoint tendon
|
|
|
which layer of the abdominal wall does the cremaster muscle come from
which nerve is it supplied by |
INTERNAL oblique
genitofemoral nerve |
|
|
what structures past through the inguinal canal in the MALE
which are within the spermatic cord? |
SPERMATIC CORD:
- Vas deferens - testicular artery - pampiniform plexus - genitofemoral nerve (lymphatics & autonomic nerves) ILIOINGUINAL nerve- outwith cord |