Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
66 Cards in this Set
- Front
- Back
|
Most common primary intraocular tumor in adults
|
Melanoma arising from ciliary body and choroid
|
|
|
Most common intraocular tumor in adults
|
Metastatic lesions
|
|
|
Most common primary intraocular tumor in kids
|
Retinoblastoma
|
|
|
Most common primary orbital lesion
|
Cavernous hemangioma
|
|
|
Most common primary orbital malignancy of children
|
Rhabdomyosarcoma
|
|
|
Neural Crest
|
Corneal stroma and endothelium **
→Connective tissue of iris/iris stroma ** Melanocytes →Trabecular meshwork →Ciliary muscle Cartilage Sclera (except for temp portion which is mesoderm) ** → Choroidal stroma |
|
|
Surface ectoderm
|
Corneal epithelium **
Lacrimal gland Lacrimal drainage system ** Epithelium, glands, cilia of skin of eyelids and caruncle |
|
|
Neuroectoderm
|
Pigmented iris epithelium **
Nonpigmented iris epithelium ** Sphincter and dilator muscles of iris ** Pigmented ciliary epithelium Nonpigmented ciliary epithelium Neurosensory retina ** Retinal pigment epithelium ** |
|
|
Mesoderm
|
Fibers of EOM **
→Endothelial lining of all orbital and muscular blood vessels Temporal portion of the sclera ** →Uveal tract comprised of Iris, Ciliary body, Choroid Neural Crest and Mesoderm) |
|
|
Patchy iris atrophy?
|
Simplex
|
|
|
Secotral iris atrophy?
|
Zoster
|
|
|
tx: Albicans
|
Ampho-B, Vori
|
|
|
tx: Aspergillus
|
Ampho-B
|
|
|
tx: Fusarium
|
Natamycin
|
|
|
Type of Immunoreaction:
• Allergic conjunctivitis |
Type I rxn: atopic, IgE ab on mast cells
|
|
|
Type of Immunoreaction:
• Ocular cicatricial pemphigoid |
Type II rxn: cytotoxic; Ab bind to foreign Ag and activate compliament
|
|
|
Type of Immunoreaction:
• Stevens-Johnson |
Type III rxn: “immune complex reactions” activate complement
|
|
|
Type of Immunoreaction:
• Scleritis |
Type III rxn: “immune complex reactions” activate complement
|
|
|
Type of Immunoreaction:
• Allergic contact dermatitis |
Type IV rxn: delayed hypersensitivity recruit pre-sensitized immune cells
|
|
|
Crystals:
|
Historically Haemophilus (more rarely)
So Schnyders, Steroids Many Multiple Myeloma Great Gout Corneas Cystinosis Get Gold Very S. Viridans (alpha-hemolytic) Big Bietti Crystals Ciloxan |
|
|
Normal corneal endothelial density:
|
1,500 – 3,500 in adults
|
|
|
Endothelial Cell Counts
Risk of edema with CE: |
1,000 cells/mm2
|
|
|
Deposition:
Band Keratopathy |
B for Basement Membrane deposotion
|
|
|
Enlarged Corneal Nerves
|
• MEN type 2B
• Refsum Disease (Phytanic acid storage disease) • Leprosy (Hansen Disease) • Acanthamoeba • NF • Riley-Day syndrome |
|
|
Limbus to limbus dystrophies include:
|
• Macular
• Meesman • Ched • Fleck (no treament for it, because no visual impairment… deposits in stroma) |
|
|
Riley-Day Syndrome (also known as: Famlial Dysautonomia)
|
• Jewish;
• skin blotching, • neurotrophic keratopathy with decreased tearing when crying. • Enlarged corneal nerves |
|
|
• Brown and Hopps stain →
|
spores of microsporidiosis
|
|
|
Prussian blue →
|
iron
|
|
|
• Von Kossa stain →
|
the calcium salts which turn blank (band keratopathy)
|
|
|
• Masson trichrome →
|
the stromal hyaline in granular dystrophy
|
|
|
• Alcian blue →
|
the stromal mucopolysaccharide in macular dystrophy
|
|
|
Inheritance of Macular Dystrophy?
|
AR
(the only recessive of the 3) |
|
|
What encodes the keratoepithelin protein?
|
TGFG1
|
|
|
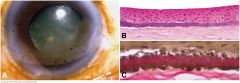
Band keratopathy. A. Clinical photo shows band of superficial opacification involving the interpalpebral part of the cornea. B. Fine basophilic granules of calcium stipple Bowman layer. C. Elastic stain highlights larger granules of actinic elastosis in case with noncalcific component. (B. H&E ×100, C. Verhoeff-Van Gieson elastic stain ×250)
|
|
|
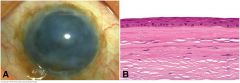
Degenerative pannus, chronic corneal edema. A. Chronically edematous cornea is opacified by subepithelial fibrosis. B. A thick layer of relatively acellular connective tissue is interposed between the corneal epithelium and intact Bowman membrane. (B. H&E ×100)
|
|
|
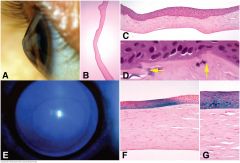
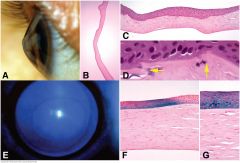
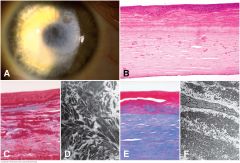
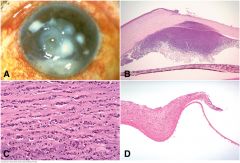
Keratoconus. A. Clinical photo shows conical shape of cornea. B. Sectioned ectatic cornea has wavy configuration. C. Photomicrograph shows severe thinning of apical stroma, compensatory hyperplasia of the epithelium and multiple dehiscences in Bowman membrane. D. Arrows point to characteristic dehiscences in Bowman membrane. E. Cobalt blue illumination highlights Fleischer ring surrounding apex of cone. F, G. Iron stain of Fleischer ring shows focal deposition of iron in corneal epithelium surrounding cone. (B. H&E ×5, C. H&E ×25, D. H&E ×250, F. Iron stain ×100, G. Iron stain ×250)
|
|
|
Epithelial dystrophies. A. Meesman epithelial dystrophy. The epithelium is thickened and contains small cystoid spaces. The epithelial basement membrane is markedly thickened. B. Cogan microcystic dystrophy. Slit lamp discloses intraepithelial deposits of putty-like cellular debris. C. Photomicrograph of microcystic dystrophy shows devitalized cellular debris trapped by duplication of the epithelium. D–F. Map-dot-fingerprint dystrophy. Photomicrographs of corneal scrapings show small intraepithelial cyst and intraepithelial segment of basement membrane (D) and marked thickening of epithelial basement membrane (E). Folds of thickened basement membrane protrude into corneal epithelium. (A. PAS ×250, C. PAS ×100, D. PAS ×100, E. PAS ×100, F. PAS ×250)
|
|
|
A. Reis-Bücklers dystrophy. Slit lamp discloses diffuse subepithelial scarring. B. Reis-Bücklers dystrophy. The “saw-toothed” epithelium rests on a thick multilaminar pannus composed of alternating layers of collagen and more eosinophilic material. Bowman material has been destroyed. Smaller deposits of eosinophilic material are seen in the stroma. C. Reis-Bücklers dystrophy. Abnormal material comprising part of multilaminar pannus in Reis-Bücklers dystrophy stains red with Masson trichrome, similar to deposits in granular corneal dystrophy. D. Electron microscopy of Reis-Bücklers dystrophy shows osmiophilic crystalloids resembling deposits in granular corneal dystrophy. E. Thiel-Behnke dystrophy. Abnormal material in multilaminar pannus stains red with Masson trichrome. F. TEM shows that abnormal material in Thiel-Behnke dystrophy is composed of “curly filaments.”
|
|
|
Band keratopathy. A. Clinical photo shows band of superficial opacification involving the interpalpebral part of the cornea. B. Fine basophilic granules of calcium stipple Bowman layer. C. Elastic stain highlights larger granules of actinic elastosis in case with noncalcific component. (B. H&E ×100, C. Verhoeff-Van Gieson elastic stain ×250)
|
|

|
Gelatinous drop-like dystrophy. A. Milky gelatinous nodules of amyloid elevate the corneal epithelium in case that recurred rapidly after penetrating keratoplasty. B. Massive subepithelial deposit of amorphous eosinophilic amyloid elevates irregular epithelium from Bowman material. Positive staining with Congo red (C) and characteristic apple-green birefringence with polarized light (D) confirms that material is amyloid.
|
|
|
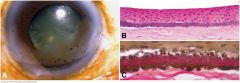
A. Prominent, anteriorly displaced line parallels limbus in clinical photo. B. Posterior embryotoxon is seen as ridge separating corneal endothelium and trabecular meshwork in scanning electron micrograph of infant eye. Ruptured iris processes bridge angle to embryotoxon. C. Large oval mound of connective tissue is interposed between the end of Descemet membrane (Schwalbe line) and the trabecular meshwork. This infant had multiple anterior segment anomalies. (B. SEM ×20, C. H&E ×50)
|
|
|
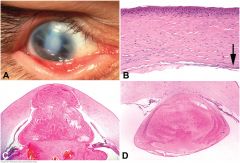
eters anomaly. A. Bands of iris stroma insert into the margin of a central corneal opacity forming iridocorneal adhesions. The lens was adherent to the posterior cornea centrally. Both eyes were affected. (Photo courtesy of Dr. Irving Raber, Wills Eye Institute.) B. The endothelium and Descemet membrane are absent in the region of a central “posterior ulcer.” Arrow denotes Descemet membrane at margin. The collagenous lamellae of the posterior stroma are thickened and irregular. Bowman membrane is absent and the epithelium is mildly thickened. A central corneal opacity was present clinically. C. Keratolenticular adhesion. Lens adheres to large defect in center of cornea. D. Peters anomaly with keratolenticular adhesion in child with fetal alcohol syndrome. The cataractous crystalline lens adheres to a posterior ulcer in the central cornea. The iris also attaches to the margin of the ulcer.
|
|
|
Acute keratitis. A. Clinical photo of acute keratitis with ulceration and hypopyon. B. Anterior chamber deep to corneal ulcer contains hypopyon. Iris is flattened by neovascular membrane. C. Acute keratitis. Polymorphonuclear leukocytes and inflammatory debris fill clefts between the stromal lamellae. Many polys have pyknotic nuclei and early stromal necrosis is present. D. Descemetocele, acute keratitis. An intact layer of Descemet membrane persists in the bed of deep corneal ulcer. The anterior layers of the cornea have been destroyed by inflammation.
|
|
|
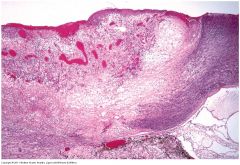
Pseudomonas sclerokeratitis. Pseudomonas keratitis often extends posteriorly as an infectious scleritis. The acutely inflamed cornea (at right) appears blue, reflecting necrosis and heavy infiltration by polys. Proteolytic enzymes released by the Gram-negative rods have dissolved the limbal sclera. The angle is closed.
|
|

|
Infectious pseudocrystalline keratopathy. A. Macrophoto shows radiating crystalline appearance of bacterial colony in cornea. B. Large basophilic colonies of relatively avirulent streptococci distend interlammelar clefts in relatively noninflamed part of the corneal stroma. C. Bacteria are Gram-positive.
|
|
|
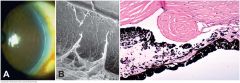
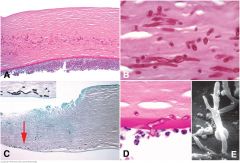
Fungal keratitis. A. Periodic acid-Schiff stain discloses numerous hyphae in mid stroma, seen at higher magnification in part B. The corneal epithelium is absent. A hypopyon adheres to the posterior cornea. C. Deep hyphae, fungal keratitis. The corneal epithelium and the anterior stroma are absent in the ulcerated area at left. Arrow points to GMS-stained hyphae in the deep stroma near Descemet membrane. Hyphae are seen at higher magnification in inset. A superficial scraping of the ulcer bed was negative for fungus. D. PAS-positive septate fungal hypha perforates Descemet membrane and invades anterior chamber, which contains polymorphonuclear leukocytes. E. Scanning electron micrographs shows branching fungal hyphae that have invaded anterior chamber.
|
|
|
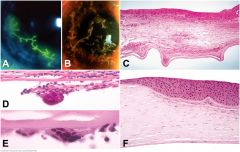
Herpes simplex keratitis. A. HSV dendritic keratitis. Branching Herpes simplex viral dendrite is full-thickness ulceration with terminal bulbs. Dendrite is stained with fluorescein dye. B. VZV dendritic keratitis. Dendritiform lesions of varicella-zoster keratitis are composed of heaped-up epithelium. (Both photos courtesy of Dr. Peter Laibson, Wills Eye Institute.) C. Chronic herpetic stromal keratitis. The stroma is thin, scarred and chronically inflamed. The inflammatory infiltrate contains lymphocytes, plasma cells and epithelioid histiocytes. Bowman membrane is largely destroyed and the epithelium is irregularly thickened. Descemet membrane is folded. D, E. Giant cell reaction to Descemet membrane, Chronic HSV keratitis. Although characteristic, this finding is not pathognomonic for HSV. F. Compensatory epithelial hyperplasia, chronic HSV keratitis. The epithelium is markedly thickened overlying an area of stroma loss. Bowman membrane persists in the area of stromal thinning.
|
|
|
Abnormal epithelial turnover
Thick BM Microcysts 6%-18% of population has it! 10% of pts will have corneal erosions 50% of pts with erosions have evidence of anterior dystrophy |
Epithelial Basement Membrane Dystrophy (EBMD)
|
|
|
*resembles Meesman (both have microcysts)
Broad band-shaped, feathery lesions in “whorled” pattern (not in Meesman!) Densely-crowded clear microcysts (Meesman are not as densely crowded) Painfree but may get decreased visual acuity No erosions No treatment required! |
Lisch
|
|
|
“peculial substance” granular and filamentary material
frequent mitosis and thickened basement membrane with increased glycogen tiny epithelial vesicles, extending to limbus (tiny bubblelike blebs) Diffuse, evenly spaced cysts with clear spaces between cysts Slight decrease in vision Recurrent erosions |
Meesman Corneal Dystrophy (MECD)
|
|
|
Subepithelial and stromal amyloid deposits
Disruption of epithelial tightj unctions 1st-2nd decade of life Mulberry configuration Larger nodular lesions = kumquat-like lesions Recurrence is 100% following corneal transplant!! Recurrent erosions |
Gelatinous = TACSTD2 gene : tumor-assoc calcium signal transducer 2
|
|
|
Pathognomonic wavy “saw-toothed” pattern
“curly-fibers” distinguish from RBCD 1st of 2nd decade Subepithelial reticular (honeycomb) opacities Recurrent erosions are less frequent and severe than RBCD |
Thiel-Behnke
|
|
|
Dominant
Masson-trichrome stain Electron microscopy needed to distinguish from Thiel-Behnke Recurrent epithelial erosions More severe and frequent than Thiel-Behnke |
Reis-Bucklers = TGFB1 gene
|
|
|
Cause? Local disorder of corneal lipid metabolism (abnl accumulation of lipid and cholesterol)
When? Diagnosed in 2nd to 3rd decade Progressive? Unusual progression Both? Bilateral What layers? Bowman and stroma Appears as? Central subepithelial crystals Stain? “Oil red-O” (stains phospholipdis red) Strange progression: central → periph → mid-periph → loss of sensation Disruption of nerve plexus Patients cas see better in the dark, because the pupil is dilated Pts have abnormal lipid levels, so check their cholesterols, too |
Schnyder corneal dystrophy (SCD)
|
|
|
When? Present at birth
Progressive? Nonprogressive or very slowly Both? Bilateral opacification of What layer? central stroma (at all levels) while peripheral cornea is clear Appears as? Whitish flakes Visual loss? Moderate-to-severea visual loss **unlike Schnyder’s, this condition is non-progressive of very slowly progressive. Mutation: decorin gene on Ch12 |
Congenital stromal corneal dystrophy (CSCD)
Congenital Hereditary Stromal Dystrophy (CHSD) = decorin gene : Chromo 12 |
|
|
Cause? Affected keratocytes are vacuolated and contain 2 abnormal substances: excess glycosaminoglycans, Lipids
Stains? (Alcian Blue, colloidal iron → glycosaminoglycans) (Oil red O, Sudan black B → Lipids) Vision is fine No treatment |
Fleck
|
|
|
Thin, flat corneas lead to hyperopia
No increased risk for glaucoma Sheet like opacity Minimal loss in vision |
Posterior amorphous corneal dystrophy
|
|
|
Endothelial cells are larger and polymorphic
Disrupted by excrascences of excess collagen Reduction in Na+/K+-ATPase pump sites |
Fuchs endothelium dystrophy
|
|
|
Similar changes that are not limited to the cornea are seen in ICE syndrome
Endo cells are multilatered and behave like epi cells or like fibroblasts |
Posterior polymorphous corneal dystrophy
|
|
|
Corneal Verticillata: FACTS IN
|
• Fabrys
• Amiodarone • Chloroquine/Chlopromazine (Thorazine) • Tamoxifen • Subconj Gentamycin • Ibuprofen/Indomethacin • Naproxen |
|
|
Iridocorneal endothelial syndrom
|
Corneal edema
Abnormal corneal endothelium Variable degrees of iris atrophy Secondary angle-closure glaucoma |
|
|
• Cogan-Reese (iris nevus)
|
ICE
**most common– multiple pigmented iris nodules produced by the contracting endothelial membrane |
|
|
• Chandler
|
ICE
pathology is confined to the inner corneal surface; corneal edema may results from subnormal endothelial pump function |
|
|
• Essential iris atrophy
|
ICE
abnormal endothelium spreads into the surface of the iris, the resulting contractile membrane may produce iris atrophy, corectopia, and polycoria (hallmark signs) |
|
|
Cloudy Cornea at Birth
|
STUMPED
• Sclerocornea • Trauma • Ulcer • Mucopolysaccharidoses • Peters anomaly **most common indication for transplant in children • Endothelial (CHED) • Dermoid Peters in the most common indication for corneal transplant in children |
|
|
Chlamydia trachoma
|
Leads to limbal follicles and their sequelae (i.e. Herbert pits), tarsal conjunctival scarring, and a vascular pannus that is most marked on the superior limbus. Conjunctival follicles are also most numerous on the superior tarsus.
|