Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
32 Cards in this Set
- Front
- Back
|
What is the mediastinum?
|
- The space between the two lungs and pleurae
- Contains all the structures of the chest except the lungs and pleurae - Extends from the superior thoracic aperture to the diaphragm, and from the sternum to the vertebrae - Mediastinum divided into superior and inferior parts, and the inferior part divided into anterior, middle and posterior parts |
|
|
Describe the contents of the divisions of the mediastinum
|
- Superior mediastinum found between the transverse thoracic plane (sternal angle to T4-T5) to the thoracic inlet:
→ Thymus anteriorly → The great vessels in the middle → The oesophagus, trachea and thoracic duct posteriorly - Inferior mediastinum between the transverse thoracic plane divided into: → Anterior inferior mediastinum = posterior to the sternum and anterior to the pericardium • Inferior thymus → Middle mediastinum • Heart and pericardium • Great arteries • Phrenic nerve • Main bronchi → Posterior mediastinum • Oesophagus • Thoracic aorta • Vertebral bodies |
|
|
What is the pericardium? Describe its layers
|
- A fibroserous sac that covers the heart and the beginning of its great vessels
- Composed of an outer fibrous layer - Inner serous part composed of 2 layers - a parietal pericardium close to the fibrous paricardium, and a visceral pericardium closest to the heart. Between these layers is secreted a layer of pericardial fluid - The pericardium helps anchor the heart and helps allow the heart to beat without friction (using the pericardial fluid) |
|
|
Describe the attachments of the pericardium
|
- Base fused with the central tendon of the diaphragm
- Fused with the tunica adventitia of the great vessels entering and leaving the heart - Anterior joined to the sternum via sternopericardial ligaments |
|
|
What are the 2 sinuses found in the pericardium?
|
- Formed by folding of the embryologial heart
- Transverse pericardial sinus is a recess within the pericardium, posterior to the aorta and the pulmonary trunk and anterior to the superior vena cava - The oblique pericardial sinus is a blind recess formed by the inferior vena cava and pulmonary veins |
|
|
Where is the base of the heart?
|
Located posteriorly and formed mainly by the left atrium
|
|
|
Where is the apex of the heart?
|
- Formed by the left ventricle and is posterior to the 5th intercostal space
|
|
|
What forms the sternocostal surface of the heart?
|
Mainly the right ventricle
|
|
|
What forms the diaphragmatic surface of the heart?
|
Mainly by the left ventricle, and part of the right ventricle
|
|
|
What forms the pulmonary surface of the heart?
|
Mainly the left ventricle
|
|
|
What makes up the borders of the anterior heart?
|
- Right = right atrium →venous side of the heart (SVC and IVC)
- Left = left ventricle and left auricle → arterial side of the heart (aortic arch, pulmonary artery) - Inferior = mainly right ventricle, and small part of left ventricle - Superior = right and left auricles |
|
|
What is pericardial effusion?
|
- Passage of fluid from pericardial capillaries into the pericardial cavity, or an accumulation of pus
- As a result, the heart becomes compressed and unable to expand or fill full because the fibrous pericardium can only stretch a little. This reduces cardiac output. - May also result from congestive heart failure = heart that fails to pump blood out at the same rate that it receives blood |
|
|
What is cardiac tamponade?
|
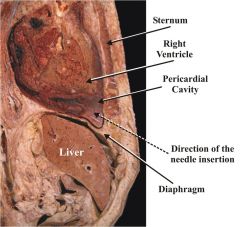
- Heart compression
- May be caused by pericardial effusion or haemopericardium (e.g due to a myocardial infarction or stab wounds). - Haemopericardium is more likely to be fatal because of the high pressure involved and the rapidity of the accumulation of fluids - Potentially lethal as the heart volume is increasingly compromised by the fluid outside the heart but inside the pericardial cavity - Treatment = pericardiocentesis → syringe at 15 degrees from surface of skin |
|
|
Describe the features of the right atrium
|

- Has the right auricle = conical muscular pouch that projects from the chamber, increasing its capacity
- Has a smooth, thin-walled posterior part, onto which the SVC, IVC and coronary sinus (between the right AV orifice and the IVC orifice) empty - Rough anterior wall composed of pectinate muscles - Smooth and rough parts of the wall separated by a vertical ridge, the crista terminalis, internally (sulcus terminalis externally) - Interarterial septim has the fossa ovalis - Tricuspid valve to the right ventricle |
|
|
Describe the features of the right ventricle
|
- Contains irregular muscular elevations = trabeculae carneae
- Thick muscular ridge, the supraventricular crest, separates the ridged muscular wall of the inflow part of the chamber from the smooth wall of the outflow part (conus arteriosus) - Papillary muscles = 3 conical muscular projections which pull chordae tendinae, which are attached to the cusps of the tricuspid valve. This closes the valve and helps prevent regurgitation - Septomarginal trabeculae (moderator band) is a curved muscular bundle that carries part of the right branch of the AV bundle - Pulmonary valve |
|
|
Describe the features of the left atrium
|
- Left muscular auricle which contains pectinate muscles
- Larger, smooth-walled part - Valveless pairs of right and left pulmonary veins enter - Thicker wall that the right atrium - Left mitral valve - Fossa ovalis with surrounding annulus ovalis (remnant of valve) |
|
|
Describe the features of the left ventricle
|

- Walls 3 times as thick as right ventricle
- Walls covered with trabeculae carneae which are more numerous and finer than those on the right - 2 papillary muscles, which are larger than the right, with cordae tendinae attached, to the aortic valve - Aortic vestibule, leading to the aortic valve |
|
|
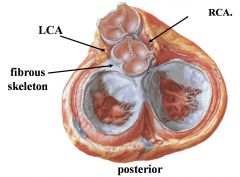
Where do the coronary arteries arise?
|
- Left coronary artery arises from the left anterior cusp of the aortic valve
- Right coronary artery arises from the right anterior aortic sinus just above the right anterior cusp of the aortic valve |
|
|
Describe the 3 tissue layers of the heart wall
|
- Epicardium aka visceral pericardium
- Myocardium = thickest layer and contains muscle cells which attach to the heart skeleton, providing a base for contraction. Atrial myocardium secretes ANP (atrial natriuretic peptide) when stretched, promoting salt and water excretion. Ventricular myocardium secretes BNP (brain natriuretic peptide) when stretched - Endocardium = 3 layers. An outermost connective tissue layer (containing nerves, vessels and Purkinje fibres), an middle connective tissue layer, and a inner endothelium of flat endothelial cells |
|
|
What is the heart skeleton?
|
- Consists of fibrocollagenous rings of dense connective tissue encircling the base of the aorta and pulmonary trunk and the atrioventricular openings
- The heart valves and muscles attach to these to form the base of muscle contraction - Also electrically insulates the atria from the ventricles except along the interventricular septum, which contains the bundle of His |
|
|
What is the most important point to remember about heart valves?
|
They are avascular so if bacteria invades the valves there will be little immune reaction and infective endocarditis may result. Also, serious problems healing
|
|
|
Describe 3 cardiac-specific radiographic views
|
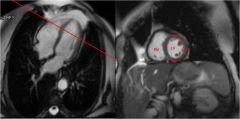
1. Short axis
- Slices perpendicular to long axis of LV - LV and RV chambers well seen - Volume measurements - Easy to see wall thickness 2. Horizontal long axis - Perpendicular plane through vertical long axis - 4 chamber view - As seen from below looking upwards and see left and right - Chamber size, septum, mitral and tricuspid valves well seen 3. Left ventricular outflow tract - Through and perpendicular to plane of aortic valve - Oblique coronal plane - Thick wall LV, brachiocephalis trunk, common carotic artery → functional anatomy of heart |
|
|
Describe the anatomical positions of the heart sounds and where you would listen to heart sounds
|

- Note that you listen to valves in the direction of the flow of blood from the valve
|
|
|
Describe the 2 pericardial sinuses
|
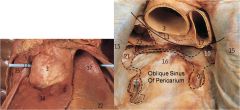
- Two sinuses:
1. Transverse sinus - posterior to the pulmonary trunk and ascending aorta and anterior to the superior vena cava. Superior to the atria; 2. Oblique sinus of the pericardium - posterior to the base of the heart, anterior to the oesophagus |
|

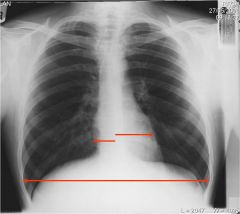
What is this and what is its cause?
|
- GLobular heart shadow on CXR
- Heart loses shape due to pericardial effusion - Pain worsens when sit forwards - AXR shows large extra swelling of fluid within the pericardium of the heart |
|
|
How can radiography be used to assess cardiac hypertrophy?
|
- Heart should occupy 50% of the maximum internal thoracic diameter on a standard PA erect view → if it is larger than this hypertrophy is present
- Cannot comment on heart size on AP view because magnification of the heart is seen |
|
|
What is dextrocardia?
|

- Heart found on RHS
- Very rare = 1/20,000 - Usually associated with other situs invertus |
|
|
Describe the path of the phrenic nerve in the mediastinum
|
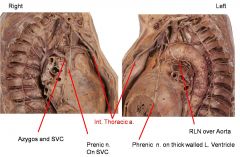
- The right phrenic nerve travels down the SVC and across the LA to the diaphragm
- The left phrenic nerve travels more anteriorly, along ascending aorta and pulmonary trunk, to travel along the left ventricle to the diaphragm |
|
|
Describe the 2 types of cardiac vavles
|

1. Semilunar vavles
- Passively opened and closed - Pulmonary artery and aorita - 3 cusps 2. Atrioventricular vavles - Passively opened and closed - Actively held closed by papillary muscles pulling on the chordae tendineae |
|

What is there problem here?
|
- Calcification of the aortic valve → aortic stenosis and possible left sided hypertrophy
|
|
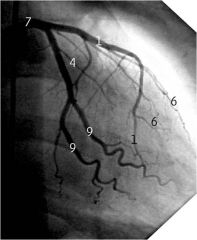
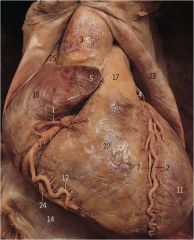
Label 1, 4 and 7
|
1 = Left anterior descending (anterior interventricular) artery
4 = Circumflex artery (NOT LAD) 7 = Left coronary artery |
|
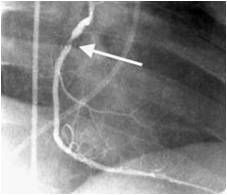
What is the problem here and how may it be treated?
|
- Coronary heart disease of right coronary artery
- Treatment 1. Coronary bypass graft (CABG = cabbage) = from internal thoracic artery or long saphenous vein 2. PTCA = coronary angioplasty → remodelling the artery through the skin 3. Stents = keeps the artery open |