Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
132 Cards in this Set
- Front
- Back
|
Where is the artery of Adamkiewicz
|
Artery of Adamkiewicz usually originates from T9-T12 intercostal artery (75%), usually on the left; may arise anywhere from T7 to L4
|
|
|
Where does artery of adamkiewics arise
|

|
|
|
What are some findings of hemoptysis with bronchial arteriography
|
Enlarged bronchial artery > 3 mm
Hypervascularity Parenchymal stain Bronchial to pulmonary artery shunting Extravasation not usually seen |
|
|
What cause the figure of 3 sign in coarctation
|
prestenotic and postenotic dilation of the aorta
|
|
|
What percent of patients with congenital coarctation will have
|
70% assoc w/congenital cardiac anomalies, MC being bicuspid aortic valve
|
|
|
Where is the location of the adult type of coarctation
|
Juxtaductal (adult) type
Lies at or just distal to level of ductus arteriosus |
|
|
What is the infantile form of coarctation
|
Generally is a long-segment narrowing
|
|
|
What is the location of the infantile form of coarctation
|
Preductal (infantile) form (less common)
Generally is a long-segment narrowing |
|
|
What are the causes of portal vein thrombosis in pediatrics and adults
|
Peds: sepsis (MC)
Adults: idiopathic, HCC, adjacent inflammation, cirrhosis, hypercoagulable state, post-transplant |
|
|
What is the finding on the venous portion of a SMA gram
|
on venous phase of SMA-gram, filling defect in portal vein
|
|
|
What is the findings of PVT in chronic cases
|
In chronic cases, cavernous transformation with multiple collaterals in porta hepatis and GB fossa
|
|
|
What are the associated findings of PVT
|
calcified portal vein, liver atrophy, splenomegaly
|
|
|
Can portal htn lead to a SMV thrombosis
|
yes
|
|
|
What are the angiographic findings in portal vein thrombosis
|
filling defect in SMV, multiple collaterals, slow flow in SMA and slow washout of mesenteric branches
|
|
|
Can SMV thrombosis lead to bowel ischemia
|
yes
|
|
|
What are the causes of SMV thrombosis
|
portal HTN, hypercoagulable state, trauma, abdominal surgery, IBD
|
|
|
What are the causes of PVT in adults
|
idiopathic, HCC, adjacent inflammation, cirrhosis, hypercoagulable state, post-transplant
|
|
|
What is the tx of portal vein and superior mesenteric vein thrombosis
|
tPA, surgical thrombectomy, portomesenteric shunt? , liver transplant
|
|
|
If you wanted to evaluate for bleeding of the lesser curve of the stomach what artery should you selectively catheterize
|
the left gastric artery
|
|
|
What is the usual source of bleeding from the doudenum
|
With duodenal bleeding, source is usually duodenal branches of GDA or right gastroepiploic artery
|
|
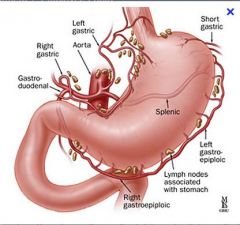
Gastrodoudenal and right gastric
|
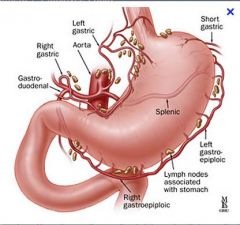
Gastroepiploic
|
|
|
What should be done if there is a clot in the IVC
|
If clot extends into IVC, put filter above clot via internal jugular vein approach
|
|
|
When should an suprarenal IVC be placed
|
this should be placed if there is a clot extends to the level of the renal vein, renal vein thrombosis, recurrent PE despite infrarenal filter placement (exclude upper extremity, SVC thrombus), PE after ovarian vein thrombosis, pregnancy
|
|
|
What should be doen if there is a PE after ovarian vein thrombosis
|
suprarenal IVC
|
|
|
What is the procedure if the patient requires an IVC filter and has duplicate IVC
|
put an IVC filter in both IVCs
|
|
|
What type of IVC filter is an option if there is an enlarged IVC
|
Birds nest filter this is the only option for megacava, IVC > 28 cm; can place up to 40 cm
|
|
|
Name the retrievable filters
|
Gunther-Tulip, OptEase, Recovery Filter, ALN
|
|
|
Name 5 different indications for an IVC filter (not complete)
|
Contraindication to anticoagulation w/known PE/DVT
Complication of anticoagulation in pt w/PE/DVT Failed anticoagulation (new onset PE/DVT) Free floating iliofemoral or IVC clot Prophylaxis (poor cardiopulmonary reserve) |
|
|
What is always done before placing an IVC filter
|
Place pigtail catheter at iliac confluence and perform IVC gram
|
|
|
What are 4 things to look at when doing a IVC gram
|
Determine IVC size, presence of IVC variants, evaluate for clot, evaluate renal vein location
|
|
|
Whant type of filter is placed if there is a very large IVC
|
birds nest filter
|
|
|
Where is the IVC filter typically deployed
|
below the level of the renal veins
|
|
|
Name 5 complications of an IVC filter
|
malposition, vascular injury, migration, recurrent PE, caval occlusion
|
|
|
Can septic emboli look like nodules or cavitations
|
yes
|
|
|
What is a radiographic technique to analyze popiteal entrapment
|
have patient plantar flex foot while imaging
|
|
|
Name 4 intrinsic causes of popiteal occlusion
|
atherosclerosis, thrombosed popliteal aneurysm, embolus, trauma
|
|
|
Name 4 extrinsic causes of popiteal entrapment
|
popliteal artery entrapment, adventitial cystic disease, extrinsic compression from popliteal cyst or tumor
|
|
|
What demographic will typically be effected byt popiteal entrapment syndrome
|
young athletic males.
|
|
|
What is the typical presenting symptom of popiteal entrapment syndrome
|
claudication
|
|
|
What is the cause of popiteal entrapment syndrome
|
Abnormal relationship of popliteal artery and gastrocnemius muscle causing arterial compression
|
|
|
What percent of pt with popiteal entrapment have it on both sides
|
25% (men more than women)
|
|
|
What is the most important thing to know about popiteal entrapment
|
that on angiographic imageit will cause medial deviation of the popiteal artery
|
|
|
What is the treatment of popiteal entrapment syndrome
|
surgical release or arterial bypass
|
|
|
What are 3 potential complications of popiteal entrapment
|
aneurysm, occlusion, distal embolization
|
|
|
Are there different ways that popiteal entrapment syndrome can occur
|
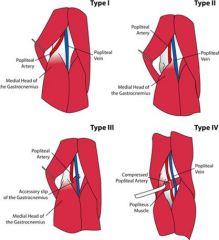
Yes
|
|
|
What is adventitial cystic disease
|
Adventitial cystic disease is a rare disease that occurs when a cyst filled with a mucus-like substance forms in one of the arteries, most commonly in the popliteal artery
|
|
|
What is a potential problem with adventitial cystic disease of the popiteal artery
|
As cysts enlarge, may rupture and occlude lumen
|
|
|
What is the typical presentation of adventitial cystic disease
|
Usually young men with sudden onset calf pain
|
|
|
What is pinch off syndrome
|
This is basically referring to the breaking off of a implanted device or catheter
|
|
|
where do most intravascular devices end up
|
Usually lodge in SVC, right heart, or pulmonary artery
|
|
|
What are the complications of 'pinch off sydnrome'
4 |
arrhythmia, clot formation, embolization, sepsis, vascular or hear perforation
|
|
|
What is the most commonly used snaring device that is used for removal of the FB in 'pinch off syndrome'
|
MC snaring device is Amplatz nitinol gooseneck snare
|
|
|
What is the ddx of non-occlusive mesenteric ischemia
|
drugs (ergots), hypotension
|
|
|
What is the most common size of the sheath that is used through the femoral vein access site
|
Most procedures done via femoral vein, through 8-10 Fr sheath
|
|
|
What is the technique to snare a FB
|
4-6 Fr guiding catheter advanced through sheath to foreign body and snare is inserted and opened and looped around free end of catheter
|
|
|
What should be if there is no free end to snare the FB
|
If there is no free end, use pigtail to reposition the fragment so that there is a free end
|
|
|
What is the ddx of non-occlusive mesenteric ischemia
|
diffuse mesenteric narrowing: ergots, hypotension, nonocclusive mesenteric ischemia
|
|
|
What are the angiographic findings in a patient with non-ccculusive mesenteric ischemai
|
slow flow in SMA, diffuse narrowing of SMA branches and arcades, segments of alternating narrowing and dilation, poor filling of vasa recta
|
|
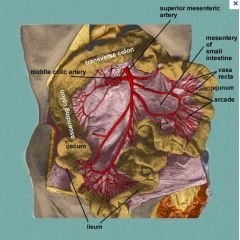
Arcades and vasa recta
|
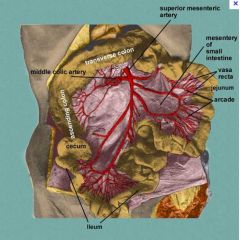
Arcades and vasa recta
|
|
|
If the contrast persist in the intestinal branches after 2 seconds should you be concerned for non-occlusive messenteric ischemia
|
yes
|
|
|
What is the medical treatment (including dose) for non-occlusive mesenteric ischemia
|
papaverine 60 mg bolus then 30-60 mg/h; in the case of narrowing related to hypotension, fix underlying cause
|
|
|
What type of medication will have ergots
|
meds for headache
|
|
|
What are the findings in hypothenar hammer syndrome
|
Focal pseudoaneurysm or occlusion of distal ulnar artery with multiple emboli to digital arteries with abrupt cutoffs
|
|
|
What is the treatment of hypothenar hammer syndrome
|
tPA for emboli, surgery for pseudoaneurysm
|
|
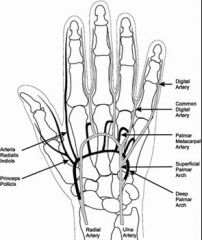
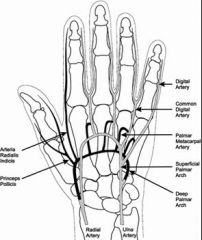
Arteries of the hand
|
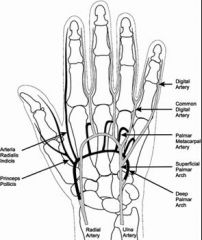
Arteries of the hand
|
|
|
Where is the branching of the deep palmar arches of the hand
|
|
|
|
What is the ddx of digital arterey occlusions
8 |
emboli
burger raynauds (scleroderma) DM idiopathic hypothenar hammer syndrome |
|
|
What side of circulation is affected by hypothenar hammer syndrome
|
ulnar side
|
|
|
What is the classic term used to describe buergers disease of the hand
|
corkscrew appearance
|
|
|
Can buergers disease effect other areas of the body besides the hand
|
yes, classically the hand but it can also affect other medium and small sized arteries
|
|
|
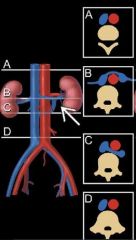
What are the findings of a circumaortic left renal vein
|
Subtle filling defect below left renal vein inflow. Normal preaortic segment enters IVC in usual location, and a retroaortic segment arises from the left renal hilum and drains into the low IVC
|
|
|
Do circumaortic renal veins have a vein infront of and behind the aorta
|
yes
|
|
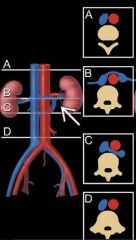
Circumaortic renal vein
|
Circumaortic renal vein
|
|
|
Can a renal vein be completely retroaortic
|
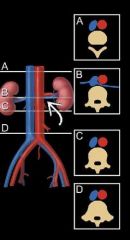
yes it is a normal variant
|
|
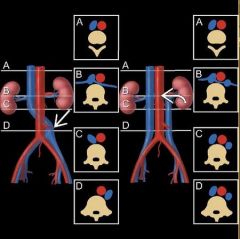
Transposition of the IVC and Duplication
|
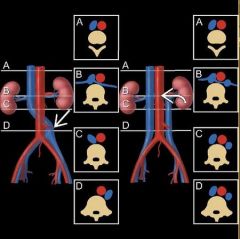
Transposition of the IVC and Duplication
|
|
|
Replaced: Replaced = arterial supply to an entire lobe is supplied by a vessel with an aberrant origin
|
Replaced: Replaced = arterial supply to an entire lobe is supplied by a vessel with an aberrant origin
|
|
|
Accessory = portion of a lobe is supplied by a vessel with an aberrant origin
|
Accessory = portion of a lobe is supplied by a vessel with an aberrant origin
|
|
|
Replaced or accessory artery arises of the liver from SMA in 20%, and from left gastric in 20%
|
Replaced or accessory artery of the liver arises from SMA in 20%, and from left gastric in 20%
|
|
|
What is polyarteritis nodosa
|
Necrotizing vasculitis of small and medium sized arteries
|
|
|
What are the findings of polyarteritis nodosa
|
small aneurysms in kidneys, GI tract, liver, and spleen
|
|
|
What is the ddx of intraparenchymal renal artery aneurysms
|
PAN, other vasculitides (Wegener), methamphetamine kidney, mycotic
|
|
|
What is the DDx of extrarenal artery aneurysm
|
atherosclerotic dz
FMD |
|
|
Can PAN affect the liver and the kidneys
|
yes
|
|
|
What is a major complication of biliary drainage procedures
|
hemobilia
|
|
|
What vessels can be involved in the cause of hemobilia
|
hepatic artery or the portal vein
|
|
|
What is the most common cause of hemobilia
|
Most are arterial, due to fistula from hepatic artery to bile duct
|
|
|
If a patient develops hemobilia following a drainage procedure what is the angiographic imaging that is used
|
celiac angiogram
|
|
|
What should be done if you do not see the source of bleeding during a celiac gram
|
If you do not see right hepatic artery, then do SMA-gram too. If no bleed seen, remove drain over a wire (drain may be tamponading bleeder)
|
|
|
What is treatment of a celiac gram
|
coil or Gelfoam embolization
|
|
|
What is the MC indication of percutaneous biliary drainage
|
Performed most often for obstruction and less often for leakage
|
|
|
What are the indications for biliary drainage
|
obstructive jaundice w/pruritus, cholangitis w/sepsis, brachytherapy access for malignant lesions, failed endoscopic biliary drainage, surgically altered anatomy (Billroth II, Roux-en-Y)
|
|
|
How is biliary brain performed
|
When obstruction is traversed, a biliary drainage catheter is inserted and locking loop is formed within duodenum
|
|
|
What is the maintainence procedure for a biliary drain
|
Should be flushed with 10 mL sterile saline two to three times daily
Routine catheter exchange every three months |
|
|
What does percutaneous biliary drainage involve
|
First do a typical biliary cholangiogram. Eventually place a cathereter through the obstructing portion so that the bile can drain into the doudenum
|
|
|
What is a percutaneous biliary cholecystomy
|
Cholecystostomy is used as a temporizing measure in critically ill patients with acute cholecystitis who cannot undergo cholecystectomy. After the symptoms resolve and the patient's condition is stabilized, definite treatment is still gallbladder removal.
In acalculous cholecystitis, percutaneous drainage may be the only treatment required. |
|
|
Where is the catheter draining in percutanous cholecystostomy
|
drain to external (through skin)
|
|
|
Where is the catheter draining in a percutaneous biliary drainage
|
the doudenum,
|
|
|
What are the indications for percutaneous biliary chocystostomy
|
Cholecystostomy is used as a temporizing measure in critically ill patients with acute cholecystitis who cannot undergo cholecystectomy. After the symptoms resolve and the patient's condition is stabilized, definite treatment is still gallbladder removal.
In acalculous cholecystitis, percutaneous drainage may be the only treatment required |
|
|
What is the treatment of a urinoma from utereral perforation
|
Percutaneous urinoma drainage along with diversionary percutaneous nephrostomy
|
|
|
What is a common cause of ureter injury
|
stone
|
|
|
How are upper ureteral injuries most commonly repaired
|
Upper ureteral injuries can frequently be repaired with ureteroureterostomy.
|
|
|
How often are ureteral stents changed
|
Ureteral stents changed at least every 6 m
|
|
|
What is important to describe if the ureter is ruptured
|
Important to determine whether urethra is intact or partially or completely disrupted
|
|
|
If there is forniceal rupture what is the clinical considerations
|
Most common signs/symptoms: Pain due to mass effect, fever if infected
Other signs/symptoms: Ileus, electrolyte imbalance Small urinomas typically resolve spontaneously Large urinomas require percutaneous or surgical drainage |
|
|
What is the treatment for iatrogenic ureteral rupture
|
Stent placement that is antegrade, retrograde, or combined
|
|
|
What is the treatment of a transected urethra
|
All transected ureters need stenting and a double J stent is used for this purpose (6, 8). A retroperitoneal drainage to limit urinoma formation and bladder decompression by Foley’s catheter is recommended.
|
|
|
What is important to know about treatment of ureteral injuries
|
the managment of a ureteral injury is variable upon the amount of urinoma, the location, the type of laceration or if it is completely transected.
|
|
|
What are the complications of percutaneous nephrolithotomy
|
Nephrolithotomy
|
|
|
What are the worrisome signs of percutaneous nephrolithotomy
|
Worrisome signs: drop in hematocrit, grossly bloody urine after 3-5 days, new clots in collecting system on follow up nephrostograms
|
|
|
What is a worrisome sign if a pt has bleeding related to nephrolithotomy
|
Worrisome signs: drop in hematocrit, grossly bloody urine after 3-5 days, new clots in collecting system on follow up nephrostograms
|
|
|
What is the treatment of significant bleeding following nephrolithotomy
|
Renal artery angiogram should be performed with embolization of any injured vessels
|
|
|
What are some of the angiogrphaphic findings in patients with bleeding following nephrolithotomy
|
pseudoaneurysm, AVF, arteriocaliceal fistula, or frank extravasation
|
|
|
What should be done if the initial angiogram is negative but you still have strong clinical concern for a bleeding
|
If initial angiogram is negative, remove nephrostomy tube over a wire because it may be tamponading the bleed
|
|
|
What is the indication of hepatic chemoembolization
|
liver-dominant malignancies which are not amenable to curative resection
|
|
|
Name 4 mets that chemoembolization is commonly used for
|
HCC, neuroendocrine malignancy, colorectal CA mets
|
|
|
What are some lab considerations in pts undergoing chemoembolization
|
Bilirubin cutoff of 3 mg/dL described
Positive predictors: Child-Pugh A/B w/albumin > 3.4 g/dL Negative predictors: MELD > 10 |
|
|
What are the preprocedure medications for chemoembolization
|
IV NS, antiemetics, steroids
|
|
|
What angiographic imaging is done prior to chemoembolization
|
Angio of SMA, celiac + evaluation of PV patency
|
|
|
Why is lobar/selective chemoembolization done if there is wide spread lesions
|
Tx of entire liver in one session assoc w/increased mortality
Avoid cystic artery if possible (increased pain; does not result in significant risk to GB itself) |
|
|
What agents are used during chemoembolization
|
Particles and cytotoxic agent
|
|
|
What percent of pts will have complications from radiofrequency ablation
|
10%
|
|
|
What is postembolization syndrome
|
Postembolization syndrome : fever, pain, increased WBC count; expected outcome
|
|
|
What are the complications of chemoembolisation
|
post-embolization syndrome
abscess liver failure death |
|
|
What is the post procedure antibiotics that are givne
|
Abx for 3-7 d to cover gram-negative enteric pathogens
|
|
|
Are narcotics and antiemetics also commonly given to pts after chemoembolization
|
yes
|
|
|
When is post treatment imaging performed
|
F/u imaging at 4-6 w and then every 3-4 m
|
|
|
What are the signs of tumor necrosis
|
Signs of tumor necrosis: Ethiodol uptake (CT) and absence of arterial-phase enhancement (CT/MR)
Residual/recurrent tumor: gross enlargement, nodular enhancement |
|
|
What is the cause of subclavian steal
|
Results from stenosis or occlusion of proximal subclavian artery
|
|
|
What is the path of blood flow in subclavian steal
|
Blood flow from contralateral vertebral to basilar to ipsilateral vertebral to subclavian
|
|
|
What may occur as a result of subclavian steal
|
May lead to cerebral ischemia with arm exercise
|
|
|
What is the angiographic findings in subclavian steel
|
Angio: vertebral not filled on initial images, but fills later
|
|
|
What is the treatment of subclavian steel
|
angioplasty/stenting of subclavian, surgical bypass
|