Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
29 Cards in this Set
- Front
- Back
|
What is an intracranial hemorrhage?
|
Intracranial bleeding when intracranial blood vessels are ruptured or leak
Can result from: - physical trauma (as occurs in head injury) - nontraumatic causes (as occurs in hemorrhagic stroke) -- eg. ruptured aneurysm. |
|
|
What is the epidemiology of strokes?
|
~800,000/year in the US
- 88% ischemic - 9% intracerebral hemorrhage (ICH) - 3% subarachnoid hemorrhage (SAH) Non-Caucasians > Caucasians |
|
|
What is the epidemiology of intracerebral hemorrhages?
|
Deep intracerebral hemorrhages are more common
The ICH rate +18% in the last decade, possibly due to: - Longer lifespan - Anticoag/antiplatelet use (atrial fibrillation treatment) - Demographic changes (higher risk factor populations up) (-lots of people have HTN) |
|
|
What is a possible risk factor for an intracerebral hemorrhage?
|
Uncontrolled hypertension
|
|
|
Where do intracerebral hemorrhages occur?
|
![Location in the brain:
- Two general categories in terms of pathophysiology:
-- Lobar (towards the periphery, typically linked to cerebral amyloid angiopathy [CAA])
-- Deep (in the deep white matter of the cerebrum, typically linked to hypertension)](https://images.cram.com/images/upload-flashcards/927467/634921_m.png)
Location in the brain:
- Two general categories in terms of pathophysiology: -- Lobar (towards the periphery, typically linked to cerebral amyloid angiopathy [CAA]) -- Deep (in the deep white matter of the cerebrum, typically linked to hypertension) Location in vessels: - Bifurcations of small penetrating arteries from basilar, anterior, middle, or posterior cerebral arteries. (Anterior>>Posterior Circulation) - Small arteries may be ruptured at multiple sites - Artery walls may have layers of platelet and fibrin aggregates with breakdown of the elastic lamina; smooth muscle atrophy; wall dissection; and cell degeneration. |
|
|
What can cause intracerebral hemorrhages? (2 main categories) Where is each generally located?
|
1) Hypertension (HTN) -> deep intracerebral hemorrhages
- Most common cause of ICH - Lipid deposition, atherosclerosis, and fibrinoid necrosis in the subendothelium -> ischemic stroke (less common: formation of microaneurysms & vessel rupture) - Recurrence risk ~2%/y if BP controlled. 2) Cerebral amyloid angiopathy (CAA) -> peripheral/lobar hemorrhage (particularly in elderly) - Disease of small vessels - Deposition of amyloid-β peptide and degenerative changes in non-large arteries in cortex, leptomeninges, and cerebellum - Recurrence risk 5-15%/y - Microbleeds can be seen as dark spots on gradient echo MRI (common and often peripheral but sometimes asymptomatic). 3) Other causes: Anticoagulants, Vascular malformations/aneurysms, Tumors (renal cell and melanoma), Infarction with hemorrhagic transformation, Venous sinus thrombosis, Drug use. |
|

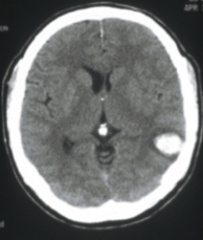
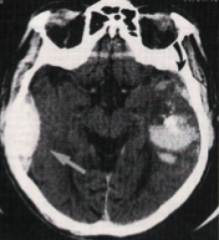
What is the likely cause of what is shown in the CT above?
|
CAA (Cerebral amyloid angiopathy) peripheral/lobar hemorrhage is mostly likely
|
|
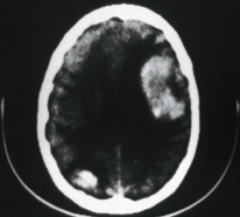
What is the likely cause of what is shown in the CT above?
|
CAA (Cerebral amyloid angiopathy) peripheral/lobar hemorrhage is mostly likely
|
|
What is the likely cause of what is shown in the CT above?
|
This is less clear, and it could be a CAA (Cerebral amyloid angiopathy) peripheral/lobar hemorrhage or a hypertensive hemorrhage (not quite a deep hemorrhage though)
|
|
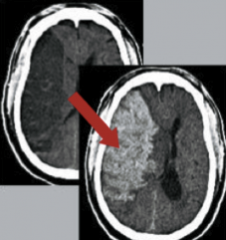
What is the likely cause of what is shown in the CTs above (left is earlier than right)?
|
The first image (to the left) shows the darker contrast, indicating a probably ischemic occlusion (right MCA infarction), but the brighter contrast in the later image (to the right) then indicates a secondary hemorrhagic transformation of the initial ischemic infarct
|
|
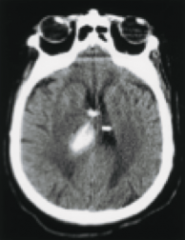
What is the likely cause of what is shown in the CT above?
|
Hypertension -> Deep hemorrhage is most likely
|
|
What is the likely cause of what is shown in the CT above?
|
Traumatic brain injury due to the multiple hemorrhage locations (coup/contrecoup)
|
|
|
What is the pathology of an intracerebral hemorrhage?
|
1) Hematoma formation after initial hemorrhage, impacting the surrounding brain tissue and causing further ischemia
2) Hematoma growth (early) -> Increased intracranial pressure, tissue shear/disruption 3) Secondary Events: triggered by the presence of blood in the brain - Toxic effects of blood products/oxidative effects - Inflammatory effects - Edema |
|
|
What is the clinical presentation of a patient with a cerebral hemorrhage?
|
Typical Presentation:
- BP > 150/90 (80% of patients) - History of HTN - Poor medication compliance - Cardiomegaly - No prodromal transient symptoms - Onset while patient is active. Red Flags: - Head trauma (distinguish between a spontaneous or traumatic hematoma) - Hematologic abnormality - *History of anticoagulants, aspirin - Symptoms prior to hemorrhage (ie. establishing if there was an underlying lesion if a patient had a symptom that went back months it could theoretically be a tumor whereas just days it could be an ICA) - Non-hypertensive site of bleeding. Symptoms: - Abrupt onset with gradual evolution over minutes to hours - A one-time event with rare recurrence (intracerebral hem = 1x event, in contrast to ischemic stroke) - Headache appears in only 50% - Neck stiffness - Vomiting - Focal seizures in approximately 10% - Focal symptoms a function of site/size of bleed - Symptoms and signs persist for months |
|
|
What is the significance of hematoma growth in intracranial hemorrhage?
|
It happens early and correlates with mortality and function.
The first 24 hours are the most important -> 10% increase in hematoma size = 5% increase in mortality + 18% increase in functional shift (independent -> assisted -> poor) |
|
|
What are the diagnosis methods for intracranial hemorrhage?
|
CT
- Fast (secs-mins), common (almost all ED) & available - Easy to read & very sensitive for acute blood (appears bright white); also may reveal secondary symptoms of ICH → hydrocephalus, edema, mass effect, and (potentially) tumor - Inexpensive (relative to MRI) MRI - Slower then CT (mins-hrs) → bad for unstable patients, less common/available - Also very sensitive (acute blood); much more sensitive (chronic blood) - More detailed look for other causes of ICH - Expensive Labs: CBC, Chem, Coags |
|
|
What can worsen prognosis of intracranial hemorrhage?
|
1) Anticoagulant use [eg. warfarin]
- Increased use of anticoagulant (atrial fibrillation treatment, venous thromboembolism, valve replacements) increases the risk of hematoma - Data has been produced to show higher deterioration in anticoagulated patients, but causation not established - Rapid reversal (fresh frozen plasma, VitK, prothrombin complex concentration [2,7,9,10]) recommended to resolve coagulopathy 2) Thrombolytics - tPA (tissue plasminogen activator) administration in the case of CNS ischemic infarction can increase the risk for hemorrhage - 20% of hemorrhages in these cases are distant from stroke site, but the other 80% is at the stroke site (secondary hemorrhage) due to leaky/weak vasculature - Risk factors: -- Age > 70 -- Stroke is large -- Early ischemic changes are visible on CT -- Serum glucose > 300 mg/dL 3) Vascular Malformation (cause of 5% of intracranial hemorrhages) - Arteriovenous malformations (AVM) - Dural A-V fistulas (dAVF) - Cavernous malformations - Aneurysms (berry, saccular, or infective) - May get an angiogram to distinguish between the above, generally up to physician's judgment |
|
|
What is the treatment for intracranial hemorrhage?
|
No definite treatment
Mostly supportive: - Seizure treatment (non-prophylactic) - Lowering BP may be helpful - Surgery is controversial, may save life at the cost of function - Skin breakdown, pneumonia, UTIs, DVT prevention due to disability of patients |
|
|
What is the outcome of intracerebral hemorrhage? How does it compare to ischemic stroke?
|
6 month mortality is 30-50%, with < 20% being independent
After 1 year, 50% patients undergo functional recovery $125,000 lifetime cost per person (1990) Compared to ischemic stroke, the outcome is much worse with ICH, with higher mortality and higher loss of function |
|
|
What determines the prognosis of intracerebral hemorrhage?
|
1) Size (hematoma volume):
- 35-50% overall mortality - ~75% mortality from massive ICH 2) Site: - worse prognosis for midline, infratentorial (higher risk for brain stem compression, little room to expand elsewhere) 3) Other factors: - age, presence of IVH (intraventricular hemorrhage, presence of blood in the ventricles), edema (probably as a marker for a midline shift), exam on presentation 4) Early withdrawal of care (careful of self-fulfilling prophecy: pts do poorly after we offer poor prognosis despite incomplete prognosis data): current recommendations are to hold off DNR for 24 h |
|
|
What are ways to predict intracerebral hemorrhage outcome?
|
MORTALITY
- Glascow Coma Scale (lower on the scale is a more severe coma, worse) - ICH volume (cc) (larger is worse) - Intraventricular hemorrhage (present is worse) - Infratentorial hemorrhage (present is worse) - Age (higher worse) FUNCTION → functional outcome instead of just mortality. Can they eat? move? etc. Glascow Coma Scale ICH volume (cc) pre-ICH cognitive impairment Age |
|
|
What is a subarachnoid hemorrhage?
|
Bleeding into the subarachnoid space (the area between the arachnoid membrane and the pia mater surrounding the brain)
May occur spontaneously, usually from a ruptured cerebral aneurysm, or may result from head injury. |
|
|
What is the epidemiology of subarachnoid hemorrhages?
|
1-7% of all strokes (region-dependent) -> 26,000/yr
Unruptured aneurysms seen in 2% of routine autopsies 45% mortality rate Majority caused by ruptured aneurysms, less commonly caused by arteriovenous malformations, other causes being trauma or ICH extension into the subarachnoid space F:M::1.6:1 45-65 age group most susceptible Japan and Finland have especially high rates |
|
|
What are risk factors for subarachnoid hemorrhages?
|
Modifiable:
- Smoking, hypertension, heavy alcohol use, sympathomimetic (eg. cocaine) use Non-modifiable: - Genetics (AD PCKD, Familial Intracranial Aneurysm Syndrome, Ehler-Danlos Syndrome [Type 4]) |
|
|
What is the clinical presentation of subarachnoid hemorrhages?
|
1) "Worst headache of life" [WHOL]
- Sudden onset and intensity, no history of migraines (which would also have a more gradual onset) 2) Neck stiffness due to meningeal irritation 3) May have vision changes 4) Possibly previous headache days before the WHOL (1/3-1/2 of survivors) -> possibly "sentinel bleeds" - leakage of subarachnoid blood from aneurysm 5) Mass effect - Diminished consciousness, papilledema, retinal/subhyaloid hemorrhage, cranial nerve palsies, size-dependent focal neurological symptoms |
|
|
What are predictors for subarachnoid hemorrhage?
|
The Hunt and Hess scale uses a calculated score to predict a value from 1-5 (asymptomatic to coma) - these are also correlated with survival levels (lower H/H is better)
|
|
|
What are tests for subarachnoid hemorrhage?
|
CT - Check for blood (and possibly hydrocephalus), generally around the vessels themselves
Lumbar puncture (rare done now due to sensitivity of CT) - Higher RBC count in CSF (103-106 RBC/mm^3), with xanthochromia (persistent pigment even after centrifuging) Angiogram - Vascular imaging in general can help visualize aneurysm |
|
|
What are the steps in treatment for subarachnoid hemorrhage?
|
1) Monitoring and control breathing, circulation
2) Blood pressure control (usually <140 mm Hg systolic) to prevent recurrent hemorrhage 3) Evaluation of hydrocephalus (common complication) and the need for management with extraventricular drainage (EVD) → to alleviate pressure. 4) Rapid evaluation of the intracranial vasculature and early surgery or endovascular coiling as indicated (avoids re-rupture) 5) Seizure prophylaxis until the source of the hemorrhage has been identified/controlled 6) Bedrest and stool softeners. 7) Nimodipine, a calcium channel blocker, was originally considered as prophylaxis against vasospasm; though it had no effect on vasospasm, it did have a measurable, as-yet-unspecified neuroprotective effect which improved 6-month outcomes markedly |
|
|
What are the complications of subarachnoid hemorrhage?
|
Hydrocephalus
- Can be communicating (no obstruction in flow, but obstructed resorption) or non-communicating (obstructed CSF flow) - Confusion, alertness decrease, upgaze paralysis, somnolence, eventually coma - Can be given an external drainage if worsened (EVD), or a ventriculoperitoneal shunt for long term if necessary - Can be protected against with monitoring and frequent imaging Vasospasm (vessel spasm leading to vasoconstriction) - Leads to secondary ischemic injury and strokes (as high as 40%) - Peaks between days 3-13 after rupture; Pts monitored with serial neuro exams and transcranial doppler (ultrasound of cranial vessels that can identify vasopasm before it even becomes a problem) evaluation of blood flow velocity through major intracerebral vessels (surrogate marker for vessel diameter). If velocities increase, they are then sent to get a traditional angiogram. - Occurs more often if thick clots seen on CT. - Can be treated by hemodynamic augmentation -- Classically HHH therapy (hypertension, hypervolemia, hemodilution) -> elevate BP, increase volume, and thin the blood to allow for perfusion -- Now more typically hypertension and euvolemia (normal volume) --- Can also be treated with Intra-arterial therapies ---- Vasodilators (commonly calcium channel blockers) ---- Angioplasty |