![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
22 Cards in this Set
- Front
- Back
|
Digoxin effect |
- Downsloping ST depression with characteristicslurred appearance - Flattened, inverted, or biphasic T waves - Shortened QT interval |
|
|
With inferior ST elevation myocardial infarction (STEMI) and the use of ____________ is relatively contraindicated in management. |
If patient presents with an inferior ST elevation myocardial infarction (STEMI) and the use of nitroglycerin is relatively contraindicated in management. In patients with myocardial ischemia or infarction, nitrates are used to decreased myocardial oxygen demand. They increase venous capacitance leading to decreased preload and are direct coronary artery vasodilators. Patients with an inferior STEMI may also have right ventricular infarct and be preload dependent. In a patient with an inferior STEMI, right ventricular infarct is suggested by the presence of ST elevation in lead III larger than that in lead II. A right ventricular infarct can be discovered by performing a right-sided ECG and looking for ST elevation in lead “RV4.” In these patients, a preload reducing medication like nitroglycerin can lead to a precipitous drop in blood pressure! |
|
|
Patients with an inferior STEMI may also have right ventricular infarct and be preload dependent. In a patient with an inferior STEMI, right ventricular infarct is suggested by the presence of [WHAT EKG FINDINGS]. A right ventricular infarct can be discovered by performing a right-sided ECG and looking for ST elevation in lead “RV4.” In these patients, a preload reducing medication like nitroglycerin can lead to a precipitous drop in blood pressure. |
ST elevation in lead III larger than that in lead II A right ventricular infarct can be discovered by performing a right-sided ECG and looking for ST elevation in lead “RV4.” In these patients, a preload reducing medication like nitroglycerin can lead to a precipitous drop in blood pressure. |
|
|
What are RBBB findings? |
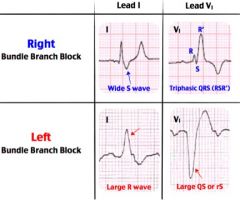
A right bundle branch block (RBBB) is a unifascibular block in which ventricular activation is by way of the left bundle branch. The impulse travels down the left bundle, thus activating the septum from the left side (as it normally does in the absence of RBBB). This is followed by activation of the free wall of the left ventricle and finally the free wall of the right ventricle. Because of the two changes in direction, there is a tendency toward triphasic complexes in a RBBB (RSR’). The ECG in a RBBB will show a wide S wave in lead I and a RSR’ pattern in lead V1. |
|
|
What are LBBB findings? |
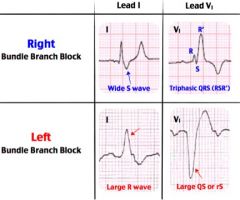
In left bundle branch block (A), lead I has a large R wave and in lead V1 there is a negative QS or rS complex. |
|
|
What is electrical alternans and what does it indicate? |

The electrocardiogram demonstrates electrical alternans, with alternating height and sometimes axis of the QRS complex due to the shifting heart inside the pericardial effusion. More commonly, the ECG demonstrates low voltage due to impaired conduction of the electrical current through the effusion to the surface of the chest wall. The quickest and most reliable test to evaluate a pericardial effusion is bedside cardiac ultrasound. Ultrasound visualizes the fluid and also identifies cardiac function and the presence or absence of tamponade. There are multiple causes of pericardial effusions including: pericarditis, malignancy, uremia, trauma, radiation and autoimmune diseases like lupus. |
|
|
True or False: Horizontal or downsloping ST-segment depression is generally more specific for ischemia than upsloping ST-segment depression. |
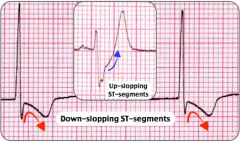
TRUE! 2 mm downslopping ST-segment depression is the most specific finding for myocardial ischemia during an exercise stress test. Subendocardial ischemia during exercise produces ST-segment depression or elevation or both. ST-segment depression that occurs during exercise testing is one of the most identifiable ECG signs of myocardial ischemia. The ECG portion of the exercise test is generally considered abnormal, or positive for ischemia, when there is ≥ 1 mm horizontal or downsloping ST-segment depression in one or more leads. Horizontal or downsloping ST-segment depression is generally more specific for ischemia than upsloping ST-segment depression. |
|
|
0.2 seconds on an ECG is one small or one large block? |
Large. Each small block is 0.04 seconds. Therefore, 5 small blocks to every 1 large block (5 x 0.04 = 0.2). |
|

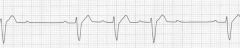
A 53-year-old man presents with dyspnea on exertion and near-syncope. His ECG is shown above. What treatment should emergently be initiated? |
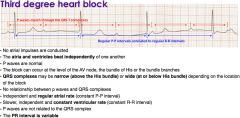
Transvenous pacemaker. This patient presents with symptomatic third degree heart block and should have a transvenous pacemaker placed. Third degree AV block (or complete heart block) is defined as an absence of conduction of atrial impulses accompanied by an escape rhythm. |
|
What does this show? |
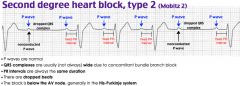
Second-degree heart block is defined by one or more impulses not reaching the ventricles and is classified as type I and type II. Type II second-degree heart block, also known as Mobitz II, is caused by an infranodal conduction abnormality, most commonly in the bundle of His or the purkinje fibers. ECG findings demonstrate random dropped QRS complexes without any changes in the PR interval. Type II second-degree heart block carries a worse prognosis than type I second-degree heart block and necessitates treatment. Unlike type I, atropine has no effect on the His-Purkinje system and may worsen conduction. Pacemaker placement is critical because this rhythm can devolve to complete heart block. In the ED, transcutaenous or transvenous pacing should be instituted if the patient is symptomatic and there should be immediate consultation with a cardiologist. |
|
|
The axis is said to be normal if it is [up/down] in which leads? |
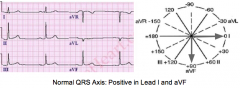
If the QRS complex is upright (positive) in both lead I and lead aVF, then the axis is normal. |
|
|
The axis is said to be Left Axis Deviation if it is [up/down] in which leads? |
QRS upright in lead I (positive) and downward in lead aVF (negative), and lead II is downward (negative), then left axis deviation is present. Causes of left axis deviation are: Normal variant, L anterior fascicular block, L ventricular hypertrophy, LBBB, inferior MI, Wolff-Parkinson White syndrome |
|
|
The axis is said to be Right Axis Deviation if it is [up/down] in which leads? |
If the QRS is predominantly negative in lead I and positive in lead aVF, then the axis is rightward (right axis deviation). Causes of right axis deviation include: normal variation, RBBB, R Ventricular hypertrophy, L posterior fascicular block, dextrocardia, lateral wall MI, Wolff-Parkinson White Syndrome, S1Q3T3 sign that occurs with PEs |
|
|
The P wave should be upright in lead _____ if the action potential is originating from the SA node. |
The P wave should be upright in lead II if the action potential is originating from the SA node. |
|
|
Remember that segments (ex. PR segment vs PR interval) are different than intervals. The important factor to analyze in segments on the ECG is [duration / their change from the isoelectric line (elevation or depression)] while the important thing to analyze for intervals is their [duration / their change from the isoelectric line (elevation or depression)] . |
Remember that segments are different than intervals. The important factor to analyze in segments on the ECG is their change from the isoelectric line (elevation or depression) while the important thing to analyze for intervals is their duration. |
|
|
What is the Q wave defined as? |
The Q wave is the first downward deflection after the P wave and is the first element in the QRS complex. When the first deflection of the QRS complex is upright, then no Q wave is present. The normal individual will have a small Q wave in many, but not all ECG leads. |
|
|
What is the R wave defined as? |
The R wave is the first upward deflection after the P wave and is part of the QRS complex. The R wave morphology itself is not of great clinical importance, however at times it can vary. In lead V1, the R wave should be small. The R wave becomes larger throughout the precordial leads (V1 to V6) to the point where the R wave is larger than the S wave in lead V4. The S wave then becomes quite small in lead V6. This is called normal "R wave progression". |
|
|
What is the S wave defined as? |
The S wave is the first downward deflection of the QRS complex that occurs after the R wave. |
|
|
What is the QT interval defined as? |
The QT interval is the time from the beginning of the QRS complex (ventricular depolarization) to the end of the T wave (ventricular repolarization). In general, the normal QT interval is less than 400-440 ms (0.4 to 0.44 seconds). A quick way to see if the QT interval is prolonged is to examine if the T wave ends past the half-way point between the R-R interval. If the T wave ends past the half-way point of the R-R interval, then it is prolonged. |
|
|
What is a delta wave and what condition is it associated with? |
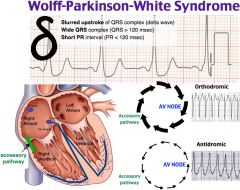
delta wave (a slurred upstroke to the QRS complex) is seen with Wolff-Parkinson-White. |
|
|
What do you see with Wolff-Parkinson-White (WPW) on EKG? |
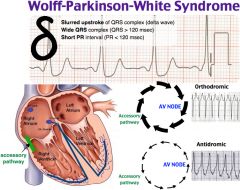
Might not see all 3 on EKG for WPW. |
|
|
What are some causes of sinus bradycardia? |
- Increased vagal tone in a well trained athlete - Sick sinus syndrome - Hypothyroidism - Hypothermia - Hypoglycemia - OSA |