Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
64 Cards in this Set
- Front
- Back
|
Vasculogenesis
a. what b. difference from angiogenesis c. from which tissue d. growth factors |
a. development of the blood system (via blood islands)
b. angiogenesis is development of new blood vessels (branching), while vasculogenesis is development "de novo" c. mesoderm of mesenchyme d. FGF2 & VEGF (needed for mesenchymal cells -> hemangioblasts (hematopoietic stem cells) and angioblasts (-> endothelium) |
|
|
Heart begins to beat on
|
22nd day
(Circulation does not start until days 27-29) |
|
|
Tubular heart is formed first via 3 "structures"
|
1. angioblastic cords ->
2. endocardial heart tubes -> 3. tubular heart |
|
|
Angioblastic cords
a. what b. where |
a. cordlike masses of splanchic mesenchymal cells, arrange themselves side-by-side to form the primordia of the endocardial haert tubes
b. lie ventrally to the primordial pericardial celom |
|
|
Endocardial heart tubes
|
Endothelial heart tubes in which two tubes come together an fuse in the midthoracic region to form the primordial cardiac\heart tube
|
|
|
Celom
|
A cavity in the mesoderm of an embryo that gives rise in humans to the pleural, peritoneal or pericardial cavity
|
|
|
Ventral folding of the head region cause the heart and pericardial to lie ... to the foregut, and ... to the oropharyngeal membrane
|
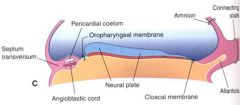
ventral to the foregut, caudal to the oropharyngeal membrane
|
|
|
Lateral folding of the embryo cause what in regards to the primordial heart
|

1. Pericardial celom expand and fuse at the midline ventrally (dorsally the primordial heart is still connected by the dorsal mesocardium)
2. Fusion of the endocardial heart tubes (inbudding of gut from yolk sac) |
|
|
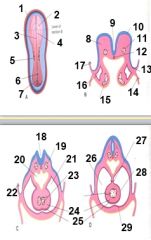
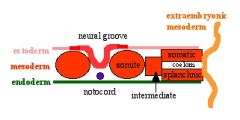
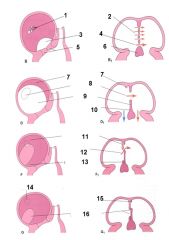
1. Cut edge of amnion
2. Pericardial coelom (ventral to brain) 3. Neural groove 4. Neural fold 5. 3rd somite 6. Primordial\primitive node (local thickening of the blastoderm at the cephalic end of the primitive streak of the embryo) 7. Primitive\primordial streak (ridge of epiblast in the midline at the caudal end of the embryonic disk from which arises the intraembryonic mesoderm and definite endoderm, day 15) 8. Mesenchyme (embryonic CT) 9. Neural groove 10. Neural fold 11. Dorsal aorta 12. Notochord (the axial fibrocellular cord about which the vertebral primordia develop, persist as nuclei pulposi in adult) 13. Lateral fold 14. Wall of yolk sac 15. Endocardial heart tube 16. Pericardial coelom (future pericardial cavity) 17. Amnion 18. Neural groove 19. Dorsal aorta 20. Foregut 21. Pericardial cavity 22. Amnion 23. Fusing endocardial tubes 24. Cardiac jelly 25. Myocardium 26. Pericardial cavity 27. Dorsal mesocardium 28. Epicardium (visceral pericardium) 29. Parietal pericardium |
|
|
Cardiac jelly
|
The gelatinous, noncellular material between the endothelial lining and the myocardial layer of the heart in very young embryos
Later in development it serves as a substrate for cardiac mesenchyme |
|
|
Dorsal mesocardium
a. what b. becomes |
a. The part of the mesocardium dorsal to the embryonic heart
b. It breaks down to form the transverse sinus of the pericardium |
|
|
Mesocardium
|
The double layer of splanchnic\visceral mesoderm supporting the embryonic haert in the pericardial cavity, it disappears before birth
|
|
|
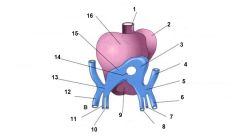
Heart tube - components
|

1. Sinus venosus (paired)
2. Primitive atrium (paired) 3. Primitive ventricle 4. Bulbus cordis (a transitory dilation where the arterial trunk joins the ventral roots of the aortic arches) 5. Truncus arteriosus (the common arterial trunk, opening out of both ventricles in early fetal life) |
|
|
The primitive heart tube
|
The earliest stage of heart development, forms primarily from splanchnic mesoderm from endocardial tubes
(Components: sinus venosus, primitive atrium, primitive ventricle, bulbus cordis, truncus arteriosus) |
|
|
The primitive ventricle, give rise to
|
Give rise to the trabeculated parts of the left and right ventricles
|
|
|
Bulbus cordis - give rise to
|
The smooth part of the the left and right ventricles
(lies ventral to the primitive ventricle after the developing heart assumes its S-shaped form) |
|
|
Sinus venosus
a. what b. give rise to |
a. A cavity at the caudal end of the embryonic cardiac tube in which the veins from the intra- and extraembryonic circulatory arcs unite
b. form the adult derivative sinus of the vena cava (the portion of the right atrium that receives blood from the venae cavae and is separated from the rest of the atrium by the crista terminalis) |
|
|
Sinus of the vena cava
|
The portion of the cavity of the right atrium that receives the blood from the venae cavae, separated from the rest of the atrium by the crista terminalis
|
|
|
Truncus arteriosus
a. what b. gives rise to |
a. The common arterial trunk opening out of both ventricles in early fetal life
b. aorta and pulmonary trunk by development of the spiral septum |
|
|
Transverse septum
a. what b. covered with what c. becomes |
a. The mesodermal mass separating the pericardial and peritoneal cavities
b. It is covered with mesothelium except where it is intimately associated with the liver (which develops within in it, this part becomes the bare area of the liver) c. The central tendon of the diaphragm |
|
|
|
|
|
Blood islands
a. what b. when & where |
a. An aggregation of splanchnic mesoderma cells on the embryonic yolk sac, has the potential to form vascular endothelium and primitive blood cells
b. day 17: forms in extra-embryonic mesoderm, day 18 in intra-embryonic mesoderm, day 19 forms cardiogenic mesoderm (pair that later coalesce) |
|
|
Extraembryonic mesoderm\primary mesoderm
|
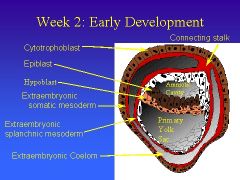
a. Cells derived from the epiblast fill the space between the trophoblast and the two cavities (amnion, yolk sac) and forms their own celom - the extraembryonic celom\chorionic cavity)
|
|
|
Intraembryonic mesoderm\Secondary mesoderm
|
Mesoderm derived from the primitive streak and lying between ectoderm and endoderm
|
|
|
The endocardial heart tube induces the cardiogenic mesoderm to differentiate into four layers
|
Inner->Outer
1. Cardiac jelly 2. Myocardium 3. Epicardium 4. Pericardial cavity |
|
|
The heart tube folds
|

Ventrally, caudally and to the right --> S-shaped tube
|
|
|
The heart tube fold at 2 sites
|

1. The bulboventricular sulcus (-> ventricular septum)
2. The atrioventricular groove |
|
|
The 3 partitionings of the heart
|
1. Partitoning of the AV canal
2. Partitoning of the primordial atrium 3. Partitoning of the primordial ventricle (From mid 4th week-->end of 5th week) |
|
|
Partitioning of AV canal
|
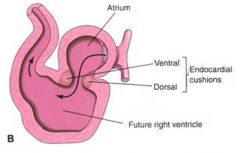
By fusion of ventral and dorsal endocardial\AV canal cushions
(AV canal cushions: a pair of mounds of embryonic CT covered by endothelium. Bulges into the embryonic AV canal, located one dorsally and one ventrally. Grow together and fuse with each other and with the lover edge of the septum primump, thus dividing the originally single canal into right and left atrioventricular orifices |
|
|
AV canal\Endocardial cushions
a. what b. which c. do what |
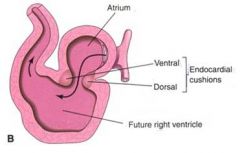
a. A pair of mounds of embryonic CT covered by endothelium
b. Located one dorsally and one ventrally c. They bulge into the embryonic AV canal, they grow together and fuse with each other and with the lower edge of the septum primum, dividing the originally single canal into right and left AV orifices |
|
|
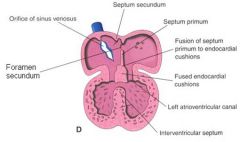
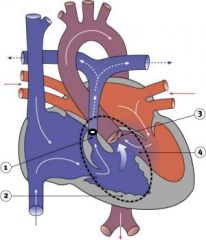
Development of partitoning of atrium
|

1. Septum primum grows inferiorly, the increasingly smaller inferior gap is know as ostium primum
2. The septum primum fuse with the endocardial cushion closing the ostium primum, meanwhile perforations in the superior part appear and develop into ostium secundum (->->fossal ovalis) 3. Septum secundum develops to the right of septum primum. It grows by upper limb (anteroinferior) and lower limb (anterosuperior) 4. Foramen ovale appears as canal through upper & lower limb of septum secundum and foramen secundum 4. Superior limb of septum secundum grow further anteroinferior and create a valve between it and the inferior part of foramen secundum 5. Decreased pressure in pulmonary circulation switch the blood flow and functionally occluding the foramen ovale after 1st breath |
|
|

|
|
|
Ductus arteriosus\Botallo duct
a. Closes how b. When |
a. The duct is kept open during fetal life by a continuous production of PGE2 by the ductus. higher pO2 -> lower PGE2 -> smooth muscle constriction. Following the constriction fibrosis occurs. (patent DA can be treated with indomethacin or ibuprofen (NSAIDs)
b. It is substantially closed after 12-24h and completely sealed after 3 weeks |
|
|
Ductus venosus
a. Closes how b. When |
a. Uncertain, appear to be a decrease in pressure in the portal sinus (resulting in retraction and narrowing of its origin which thus assumes a slit-like appearance), also probably reinforced by muscular elements in the wall of the portal sinus near the origin of the duct
b. functional: 1st minute parturition, organic closure: within 15-20th day |
|
|
Partitioning of the primordial ventricle
|
1. Primordial interventricular septum (becomes muscular part of the IV septum)(from ventricular wall)
2. Membranous part of IVS (from fused bulbar ridges and fused endocardial cushions)(last to fuse) |
|
|
The bulbar\conotruncal ridge
a. what b. gives rise to c. derived from |
a. one of two spiral subendocardial thickenings in the embryonic bulbus cordis
b. when they fuse, they divide the bulbus into the aorta and pulmonary artery, contribute to formation of semilunar valves, and contribute to formation of membranous IVS c. derived from ectomesenchyme from cranial neural crest |
|
|
The endocardial\AV canal cushions
a. what b. give rise to |
a. a pair of mounds of embryonic CT covered by endothelium
b. part of membranous part of IVS, divide the AV canal, contribute to formation of the AV valves, contribute to septum primum in atrium |
|
|
Partitoning of bulbus cordis and truncus arteriosus
a. By what b. How |
a. By bulbar and truncal ridges which form aortico-pulmonary septum\spiral septum
b. perform a 180 degree spiraling and fusing |
|
|
The aorticopulmonary\Spiral septum
a. formed by, induced by b. Function |
a. Arise within the truncus arteriosus from downward helical growth and fusion of conotruncal ridges (one on each side), which is induced by invasion of neural crest cells
b. Divide the ventricular outflow between the pulmonary artery and the ascending aorta |
|
|
Eisenmenger's syndrome
|
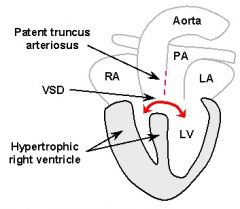
Occurs as a result of equal division of the truncus arteriosus with an incomplete fusion of bulbar ridges proximally involving the membranous part of the IVS. This results in
1. Persistent truncus arteriosus 2. IVSD 3. Left-to-right shunt -> pulmonary hypertension (capillaries are destroyed and replaced by scar tissue (decrease diffusion surface & cause sclerosis -> increased afterload) -> shunt reversal |
|
|
Which syndrome occurs when the division of the AP septum occurs asymmetrically
|
Tetralogy of Fallot
|
|
|
Dorsal folding of heart
a. effect on direction of heart tube b. mediated by c. fold at d. forms what e. does what to the fibrous skeleton of the heart |
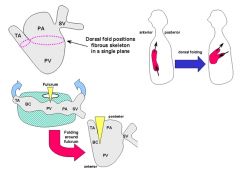
a. Inflow and outflow trunks are positioned posteriorly
b. Mediated by apoptosis in the dorsal mesocardium c. The bulboventricular sulcus d. Forms the two pericardial sinuses e. Places the fibrous skeleton in a single plane |
|
|
Superior vena cava develops from
|
Right anterior cardinal vein and the right common cardinal vein
|
|
|
Critical period for development of the heart and the great vessels
|
3rd-6th week
|
|
|
Frequency of anomalies of heart and great vessels
|
6-8\1000 births
|
|
|
Aortic arch derivatives - 1st pair
|
1. Maxillary aa
2. External carotid aa |
|
|
Aortic arch derivatives - 2nd pair
|
Stapedial & hyoid aa
|
|
|
Aortic arch derivatives - 3rd pair
|
Proximal -> Common carotid aa
Distal -> Internal carotid aa |
|
|
Aortic arch derivatives - 4th pair
|
Left -> part of arch of aorta
Right -> right subclavian artery (distal part forms from the right dorsal aorta Left subclavian artery is not derived from an aortic arch, its derived from the 7th intersegmental artery |
|
|
Origin of subclavian arteries
|
Right <- right 4th pair of aortic arch, distal part from right dorsal aorta
Left <- 7th intersegmental artery |
|
|
Aortic arches
a. what b. how many |
a. A series of arterial channels encircling the embryonic pharynx in the mesenchyme of the branchial arches
b. potentially 6 pairs, but in mammals the 5th is poorly developed or absent |
|
|
Aortic arch derivatives - 6th pair
|
Left
a. proximal -> left pulmonary artery b. distal -> Ductus arteriosus (Botali) Right -> right pulmonary artery |
|
|
|
|
|
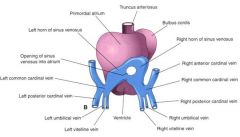
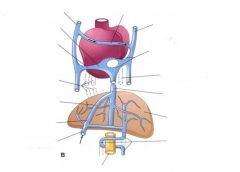
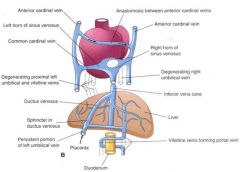
The vitelline veins give rise to the aduldt derivatives
|
1. Hepatic veins (from the remains of the right vitelline vein
2. Portal vein (from an anastomotic network around the duodenum) |
|
|
Umbilical veins - fetal development
|
Right and part of the left vein degenerate, the persistent part of the left become the umbilical vein
(the ductus venosus shunt ca 50% the blood it returns through the liver) |
|
|
Changes in the sinus venosus - fate of right horn
|
It enlarges, receives all the blood from the head and neck (SVC) and caudal regions (IVC)
It becomes incorporated into the wall of the right atrium |
|
|
Changes in the sinus venosus - fate of left horn
|
Decrease in size and importance - to become coronary sinus
|
|
|
Types of atrial septal defects
|
1. Patent foramen ovale (in 25% of people a probe patent foramen ovale exists)
2. Ostium secundum defects 3. Endocardial cushion defect involving ostium primum (often associated with AV valve defects) 4. Common atrium |
|
|
Patent ductus arteriosus
a. Most common in b. Who is at risk |
a. Most common in preterm infants (60% close spontaneously wi 3 days)
b. Preterm, Down's, Maternal Rubella infection during pregnancy, 2x as common in girls |
|
|
Tetralogy of Fallot - 4 components
|
1. Pulmonary stenosis (valvular or infundibular\conus arteriosus(from supraventricular crest to pulmonary trunk, smooth-walled)
2. Right ventricular hypertrophy 3. Dextroposition of aorta (Overriding aorta) 4. Ventricular septal defect |
|
|
Dextrocardia
|
Initial malrotation of the heart tube bending left instead of right.
(Results in heart and greater vessels reversed, can also occur with situs inversus) (Not symptomatic. Defibrillate on the right side) |
|
|
Coarctation of the aorta
a. types |
a. preductal (5% of turner syndrome), ductal, postductal (most common)
(Associated with bicuspid aortic valve, defect in which only one ventricle is present, VSD) |
|
|
Long QT syndrome
a. what, effect b. cause |
a. Group of rare genetic disorders with prolonged ventricular repolarization and a risk of ventricular tachyarrhythmias.
b. Cause is mutation in genes encoding either cardiac ion channels or channel interacting proteins. |
|
|
Groups of congenital heart diseases
|
Group 1: left->right shunts (acyanotic heart disease, frequent infections, include VSD, ASD, PDA, AV canal)
Group 2: right->left shunts (tetraology of Fallot, overriding aorta, pulmonary stenosis, right ventricular hypertrophy) Group 3: Obstructive lesions |