![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
30 Cards in this Set
- Front
- Back
|
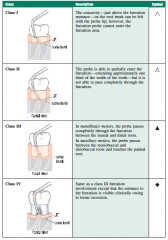
Glickman's classification |
|
|
|
Simon, Glick and Frank 1972 |

|
|
|
Lowman JV, Burke RS, Pelleu GB. Oral Surg Oral Med Oral Pathol 1973 |
Coronal and mid-root accessory canals are present in 55% of maxillary molars and 63% of mandibular molars. (dye under vacuum) |
|
|
Vertucci FJ, Williams RG. Oral Surg Oral Med Oral Pathol 1974 |
46% of the mandibular 1st molars exhibited lateral canals in the furcation region. 13% were deemed furcation canals, 23% had lateral canals, and 10% contained both lateral and furcation canals. (dye penetration) |
|
|
Sinai IH, Soltanoff W. Oral Surg Oral Med Oral Pathol 1973 |
Histologic study of rat's teeth with induced periodontal or pulpal disease. Pulpal disease affects the periodontium quickly with inflammation; perio disease affects the pulp slowly with degenerative changes. |
|
|
Jansson L, Ehnevid H,Lindskog S, Blomlof L: J Clin Periodontol 1995
|
Endodontic infections had an approximate 3-fold amplification on the rate of marginal proximal radiographic bone loss in periodontitis-prone patients (an average bone loss of 0.19 mm/year, compared to 0.06 mm/year for teeth with no or subsiding endodontic infection). |
|
|
Jansson L, Ehnevid H,Blomlof L, Weintraub A, Lindskog S. J Clin Periodontol 1995 |
intra-canal infection of endodontic pathogens stimulates epitelial downgrowth along denuded dentin surfaces with marginal communication. |
|
|
Ehnevid H, Jansson,Lindskog S, Weintraub A, Blomlof L. EndodDent Traumatol 1995
|
endodontic pathogens or their products could spread through dentinal tubules to a root surface devoid of cementum but were not able to penetrate the cementum barrier. |
|
|
Jansson LE, Ehnevid H. J Periodontol. 1998 |
endodontic infection in mandibular molars was found to be associated with additional attachment loss in the furcation area, and may thus be considered to be one of several risk factors influencing the prognosis of molars in periodontitis-prone patients. |
|
|
Miyashita H, Bergenholtz G, Grondahl K, Wennstrom JL. J Periodontol 1998 |
Endodontic therapy or pathology had no apparent influence on marginal bone levels in patients with minimal to no periodontal disease. This study failed to demonstrate a correlation between a reduced marginal bone support and prior endodontic treatment. |
|
|
Mazur B, Massler M. Oral Surg Oral Med Oral Pathol 1964 |
A histologic study of extracted teeth showed no relationship between the severity of periodontal disease and pulpal changes. The status of the periodontium doesn't exert any great influence on the pulp. |
|
|
Bergenholtz G, Lindhe J. J Clin Periodon 1978 |
The study showed that the destruction of periodontal tissues did not affect the pulp of the teeth. This was found in Monkeys with no lateral canals and the periodontal breakdown did not reach the apex. |
|
|
Czarnecki RT, Schilder H. J Endod 1979 |
No correlation between periodontal disease in itself and the presence or absence of pulpal pathology. Pulp pathosis is associated with decay or past restorative treatment. Perio treatment may contribute to pulp pathosis. |
|
|
Hattler AB, Listgarten MA. J Endod 1984 |
In rat teeth that were mechanically root planed and scaled, there was formation of reparative dentin opposite the instrumented surface without histological evidence of inflammation. |
|
|
Bergenholtz G, Nyman S. JPeriodontol 1984. |
In teeth with advanced periodontal disease, pulp necrosis developed with a significantly higher rate in abutment teeth (15%) than in non-abutment teeth(3%). The observation period varied from 4-13 years, with a mean of 8.7 years. |
|
|
Seltzer S, Bender IB, Ziontz M. Oral Surg Oral Med Oral Pathol 1963 |
periodontal disease produced a degenerative effect on the pulp. Teeth with both periodontal lesions and caries or restorations exhibited greater inflammation and pulpal necrosis than teeth with only periodontal lesions or only caries or restorations.
-no healthy controls |
|
|
Rubach WC, Mitchell DF. J Periodontol 1965 |
A histological study of extracted teeth with varying degrees of periodontitis. 15% of the teeth had pulpal pathosis secondary to accessory canal communication with the periodontium. -no healthy controls |
|
|
Bender IB, Seltzer S. Oral Surg OralMed Oral Pathol 1972 |
Presented the"pulpodontic-periodontic" syndrome. Periodontal disease can cause pulpal disease and vice-versa. There is a greater tendency for the pulp to undergo degenerative/inflammatory changes or necrosis if the tooth is subjected to more than one irritant, i.e. periodontal disease with caries and/or restorations. |
|
|
Wong R, Hirsch RS, Clarke NG. Endod Dent Traumatol 1989 |
Root planing opens dentinal tubules to bacterial invasion and potential localized pulpitis. |
|
|
Kipioti A, Nakou M, Legakis N, Mitsis F. Oral Surg Oral Med Oral Pathol 1984 |
Microorganisms present in the root canals of caries-free teeth with advanced periodontitis generally resembled those found in the adjacent periodontal pockets (P. gingivalis, P. melaninogenicus and P. intermedius most commonly detected). Streptococci were a prominent genus cultured from both sites. |
|
|
Kobayashi T, Hayashi A, Yoshikawa R, Okuda K, Hara K. Int Endod J 1990 |
The presence of micro-organisms common to both deep periodontal pockets and non-vital root canals indicates that the periodontal pocket may be a possible source of root canal infections in caries free teeth. |
|
|
Rupf S, Kannengieber S, Merte K, Pfister W, Sigusch B, Eschrich K. DentTraumatol 2000 |
Periodontalpathogens (AA, B. forsythus, E.corrodens, F. nucleatum, P. gingivalis, P. intermedia) could be demonstrated in the endodontium when present in the periodontium. |
|
|
Harrington GW. Dent Clin North Am 1979 |
Periodontal probing is the primary diagnostic method used to discern between primary periodontal and primary endodontic lesions. -blowout type lesion -conical lesion (perio) -narrow sinus tract lesion -wide sinus tract lesion -sinus tract lesion at the base of a conical lesion (true combined communicating) -no probing |
|
|
Paul BF, Hutter JW. J Am Dent Assoc 1997. |
This review article recommends providing endodontic therapy 1-2 months prior to periodontal therapy to avoid removal ofhealthy periodontal tissue. |
|
|
Lima LA, Anderson GB, Wang MM, Nasjleti CE, Morrison EC, Kon S, Caffesse RG. J Periodontol 1997 |
Root canal therapy performed simultaneously or 3 weeks after surgery modified the healing of intrabony defects, impairing new bone formation, cementum formation and attachment. SRP, MWF, RCT/MWF, MWF+RCT. dog study |
|
|
Britain SK, von Arx T, Schenk RK, Buser D, Nummikoski P, Cochran DL. J Periodontol 2005 |
Treatment of combined induced perio-endo lesions (PA+buccal cortical plate) using bioabsorbable collagen membranes alone or in combination with anorganic bovine bone matrix resulted in increased amounts of bone, periodontal ligament, and new cementum when compared to open flap debridement in a canine model. |
|
|
Kim E, Song JS, Jung IY, Lee SJ, Kim S. J Endod. 2008 |
The successful (complete and incomplete healing) outcome for isolated endodontic lesions treated with S-RCT was 95.2%. In endodontic-periodontal combined lesions, successful outcome was 77.5%, suggesting that lesion type had a strong effect on tissue and bone healing. -Kim and Kratchman classification JOE 2006. -prospective study (263 teeth). |
|
|
Schmidt JC, Walter C, Amato M, Weiger R. J Clin Periodontol. 2014 |
A sequential treatment with root canal treatment as a first treatment step appears to be reasonable. An adequate time for tissue healing is suggested prior to re-evaluation. Sys Rev. 23 studies included (1 RCT, 4 case series, and 18 case reports) |
|
|
Raheja J, Tewari S, Tewari S, Duhan J. J Periodontol. 2014 |
CHX may be used as an effective intracanal medicament for promoting periodontal healing in concomitant endodontic-periodontal lesions. -clinical study, 31 pts, CHX placed in post space + OFD. |
|
|
Gupta S, Tewari S, Tewari S, Mittal S. J Endod. 2015 |
Nonsurgical periodontal treatment may be performed simultaneously with endodontic treatment in the management of concurrent endodontic-periodontal lesions without communication, and an observation period after endodontic treatment may not be required. -RCT, 31 pts. |