Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
12 Cards in this Set
- Front
- Back
|
Clinical EHK/BCIE/BI
|
|
|
|
Clinical EHK/BCIE/BI
|

|
|
|
Inheritance
|
Autosomal dominant; 50% spontaneous mutations; keratin K1, K1 0 genes on 12q, 1 7q respectively
|
|
|
Prenatal
|
Fetal skin biopsy at 20 to 22 weeks clumped keratin filaments on electron
microscopy DNA analysis: K1 and K1 0 mutations if defect in family known, linkage analysis if kindred is large |
|
|
Incidence
|
Rare approximately 3,000 Americans afflicted; M=F
|
|
|
Age @P
|
Birth
|
|
|
Pathogenesis
|
Heterogeneous gene defects in K1, K1 0 leads to defective keratin filaments in the upper epidermis with subsequent tonofilament clumping and bullae formation; arg res 156 of K1 0 is most common site for mutation with greatest severity at terminal rod regions Extensive epidermal nevi (ichthyosis hystrix) reflect a somatic mosaicism for KI /K1 0 mutations; if gonadal mosaicism, then may have offspring with fullblown epidermolytic hyperkeratosis
|
|
|
Clinical
|
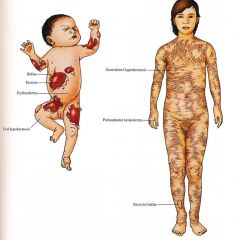
Skin
Newborn Widespread bullae, erythroderma, denuded skin; secondary sepsis, electrolyte imbalance; ± focal areas of hyperkeratosis Later Infancy to Adulthood Localized to generalized hyperkeratosis with rare, focal bullae secondary to infection (Staphyloccus aureus, gram negative bacteria); dark, warty scales with spiny ridges, increased in flexures; secondary bacterial infection with foul odor in macerated, intertriginous areas; scales shed with full thickness stratum corneum leaving tender, denuded base; prominent palmoplantar keratoderma (in some patients); secondary nail dystrophy |
|
|
D/Dx
|
Newborn
Epidermolysis bullosa (p. 200) Staphylococcal scalded skin syndrome Toxic epidermal necrolysis Other causes of blistering Later Infancy to Adult Otherichthyoses |
|
|
Lab
|
Skin biopsy for hernatoxylin and eosin (H&Q, frozen section (in newborn), and electron micro
Bacterial culture |
|
|
Manage
|
Newborn
Transfer to neonatal intensive care unit monitor fluid, electrolytes, sepsis workup; intravenous (IV) broad spectrum antibiotics until cultures negative; gentle handling, protective isolation Later Infancy to Adulthood Avoid topical keratolytics, salicylic acid, corticosteroids; systemic retinoids short course in adulthood for flares; emolliation; antistaphylococcal, gram negative antibiotic coverage; antibacterial soaps Betadine, Chlorhexicline, Clorox in bath |
|
|
Prognosis
|
Widespread blistering clears after newborn period; hyperkeratotic scale usually lifelong; generalized involvement may improve to localized disease after puberty
|