Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
228 Cards in this Set
- Front
- Back
|
What does it tell you if there are casts in the urine? |
Hematuria / pyuria is of renal origin (vs bladder if there are no casts)
|
|
|
What are the types of casts that can be present in the urine?
|
- RBC casts
- WBC casts - Fatty casts ("oval fat bodies") - Granular ("muddy brown") casts - Waxy casts - Hyaline casts |
|
|
What can RBC casts in the urine indicate?
|
- Glomerulonephritis
- Ischemia - Malignant hypertension |
|
|
What can WBC casts in the urine indicate?
|
- Tubulointerstitial inflammation
- Acute pyelonephritis - Transplant rejection |
|
|
What can fatty casts ("oval fat bodies") in the urine indicate?
|
Nephrotic syndrome
|
|
|
What can granular ("muddy brown") casts in the urine indicate?
|
Acute Tubular Necrosis
|
|
|
What can waxy casts in the urine indicate?
|
Advanced renal disease / chronic renal failure
|
|
|
What can hyaline casts in the urine indicate?
|
Non-specific, can be a normal finding, often seen in concentrated urine samples
|
|
|
What can hematuria without casts in the urine indicate?
|
- Bladder cancer
- Kidney stones |
|
|
What can pyuria (pus) with no casts in the urine indicate?
|
Acute Cystitis
|
|
|
What terms can be used to describe glomerular disorders?
|
- Focal vs Diffuse
- Proliferative - Membranous - 1° Glomerular disease - 2° Glomerular disease |
|
|
What does the term "focal" mean when naming a glomerular disorder? Example?
|
<50% of glomeruli are involved
- Eg: focal segmental glomerulosclerosis |
|
|
What does the term "diffuse" mean when naming a glomerular disorder? Example?
|
>50% of glomeruli are involved
- Eg: diffuse proliferative glomerulonephritis |
|
|
What does the term "proliferative" mean when naming a glomerular disorder? Example?
|
Hypercellular glomeruli
- Eg: Mesangial Proliferative |
|
|
What does the term "membranous" mean when naming a glomerular disorder? Example?
|
Thickening of the glomerular basement membrane
- Eg: Membranous Nephropathy |
|
|
What does the term "1° Glomerular Disease" tell you about the glomerular disorder? Example?
|
Involves only glomeruli, thus a 1° disease of the kidney
- Eg: minimal change disease |
|
|
What does the term "2° Glomerular Disease" tell you about the glomerular disorder? Example?
|
Involves glomeruli and other organs, thus a disease of another organ system, or a systemic disease that has impact on the kidney
- Eg: SLE and diabetic nephropathy |
|
|
What are the types of glomerular diseases?
|
- Nephritic Syndrome
- Nephrotic Syndrome - Both |
|
|
What are the types of Nephritic Syndromes?
|
- Acute Post-Streptococcal Glomerulonephritis
- Rapidly Progressive Glomerulonephritis - Berger Disease (IgA Glomerulonephropathy) - Alport Syndrome *Note that the classic nephritic disorders can exhibit some nephrotic features |
|
|
What are the types of Nephrotic Syndromes?
|
- Focal Segmental Glomerulosclerosis
- Membranous Nephropathy - Minimal Change Disease - Amyloidosis - Diabetic Glomerulonephropathy |
|
|
What are the types of glomerular diseases that are characterized as both Nephritic and Nephrotic Syndromes?
|
- Diffuse Proliferative Glomerulonephritis
- Membranoproliferative Glomerulonephritis |
|
|
What makes a renal disease a "Nephrotic syndrome"?
|
- Massive Pr"O"teinuria (>3.5 g/day, frothy urine)
- Hyperlipidemia - Fatty casts - Edema |
|
|
What are Nephrotic Syndromes associated with? Why?
|
- Thromboembolism (hypercoagulable state d/t AT III loss in urine)
- Increased risk of infection (due to loss of immunoglobulins) |
|
|
Which type of nephrotic syndrome is associated with the following LM findings: segmental sclerosis and hyalinosis?
|
Focal Segmental Glomerulosclerosis
|
|
|
Which type of nephrotic syndrome is associated with the following LM findings: diffuse capillary and GBM thickening?
|
Membranous Nephropathy
|
|
|
Which type of nephrotic syndrome is associated with the following LM findings: normal glomeruli (lipid may be seen in PCT cells)?
|
Minimal Change Disease (Lipoid Nephrosis)
|
|
|
Which type of nephrotic syndrome is associated with the following LM findings: congo red stain shows apple-green birefringence under polarized light?
|
Amyloidosis
|
|
|
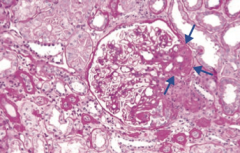
Which type of nephrotic syndrome is associated with the following LM findings: mesangial expansion, GBM thickening, and eosinophilic nodular glomerulosclerosis (Kimmelstiel-Wilson lesion)?
|
Diabetic Glomerulonephropathy
|
|
|
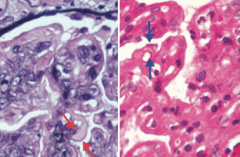
Which type of nephrotic syndrome is associated with the following LM findings: thickened "tram tracks"?
|
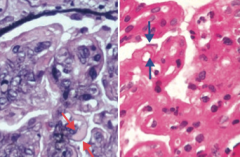
Membrano-Proliferative Glomerulonephritis (Type 1)
- Left: PAS stain - Right: H&E stain |
|
|
Which type of nephrotic syndrome is associated with the following EM findings: effacement of foot processes?
|
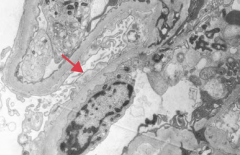
- Focal Segmental Glomerulosclerosis
- Minimal Change Disease (Lipoid Nephrosis) = picture |
|
|
Which type of nephrotic syndrome is associated with the following EM findings: "spike-and-dome" appearance with subepithelial deposits?
|
Membranous Nephropathy
|
|
|
Which type of nephrotic syndrome is associated with the following immunofluorescence findings: granular as a result of immune complex deposition?
|
Membranous Nephropathy
|
|
|
What is the most common cause of nephrotic syndrome in African Americans and Hispanics?
|
Focal Segmental Glomerulosclerosis
|
|
|
What is the most common cause of nephrotic syndrome in Caucasian adults?
|
Membranous Nephropathy
|
|
|
What is the most common cause of nephrotic syndrome in children?
|
Minimal Change Disease (Lipoid Nephrosis)
|
|
|
Which type of nephrotic syndrome is associated with HIV infection?
|
Focal Segmental Glomerulosclerosis
|
|
|
Which type of nephrotic syndrome is associated with sickle cell disease?
|
Focal Segmental Glomerulosclerosis
|
|
|
Which type of nephrotic syndrome is associated with heroin abuse?
|
Focal Segmental Glomerulosclerosis
|
|
|
Which type of nephrotic syndrome is associated with massive obesity?
|
Focal Segmental Glomerulosclerosis
|
|
|
Which type of nephrotic syndrome is associated with interferon treatment?
|
Focal Segmental Glomerulosclerosis
|
|
|
Which type of nephrotic syndrome is associated with chronic kidney disease due to congenital absence or surgical removal?
|
Focal Segmental Glomerulosclerosis
|
|
|
How do you treat Focal Segmental Glomerulosclerosis? Efficacy? Prognosis?
|
- Inconsistent response to steroid therapy
- May progress to chronic renal disease |
|
|
What type of disease is Focal Segmental Glomerulosclerosis? What changes occur in this disease?
|
Nephrotic Syndrome:
- Segmental sclerosis and hyalinosis - Effacement of foot processes similar to in minimal change disease |
|
|
Which type of nephrotic syndrome is associated with antibody to phospholipase A2 receptor?
|
Membranous Nephropathy
|
|
|
Which type of nephrotic syndrome is associated with drugs like NSAIDs and penicillamine?
|
Membranous Nephropathy
|
|
|
Which type of nephrotic syndrome is associated with infections like HBV and HCV?
|
Membranous Nephropathy
|
|
|
Which type of nephrotic syndrome is associated with Systemic Lupus Erythematosus?
|
Membranous Nephropathy
|
|
|
Which type of nephrotic syndrome is associated with solid tumors?
|
Membranous Nephropathy
|
|
|
How do you treat Membranous Nephropathy? Efficacy? Prognosis?
|
- Poor response to steroid therapy
- May progress to chronic renal disease |
|
|
What type of disease is Membranous Nephropathy? What changes occur in this disease?
|
Nephrotic Syndrome
- Diffuse capillary and GBM thickening - Granular immunofluorescence as a result of immune complex deposition - "Spike and dome" appearance on EM with subepithelial deposits |
|
|
Which type of nephrotic syndrome may be triggered by a recent infection, immunization, or other immune stimulus?
|
Minimal Change Disease (Lipoid Nephrosis)
|
|
|
Which type of nephrotic syndrome is associated with Hodgkin Lymphoma (eg, cytokine-mediated damage)?
|
Minimal Change Disease (Lipoid Nephrosis)
|
|
|
How do you treat Minimal Change Disease (Lipoid Nephrosis)? Efficacy? Prognosis?
|
Excellent response to corticosteroids
|
|
|
What type of disease is Minimal Change Disease (Lipoid Nephrosis)? What changes occur in this disease?
|
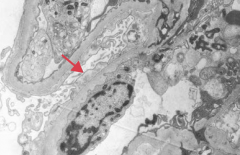
Nephrotic Syndrome:
- Normal glomeruli (lipid may be seen in PCT cells) - Effacement of foot processes |
|
|
Which type of nephrotic syndrome is associated with chronic conditions like multiple myeloma, TB, or Rheumatoid arthritis?
|
Amyloidosis
|
|
|
Amyloidosis most commonly affects what organ?
|
Kidney is the most common organ involved in systemic amyloidosis
|
|
|
What type of disease is Amyloidosis that affects the kidney? How do you make diagnosis?
|
Nephrotic Syndrome
- Congo red stain shows apple-green birefringence under polarized light |
|
|
What are the types of membrano-proliferative glomerulonephritis?
|
- Type I: subendothelial immune complex (IC) deposits with granular immunofluorescence - "tram-track" appearance
- Type II: intramembranous IC deposits - "dense deposits" |
|
|
Which type of nephrotic syndrome is associated with HBV and HCV? What type of deposits? Appearance?
|
Type I Membrano-Proliferative Glomerulonephritis
- Subendothelial immune complex (IC) deposits - Granular IF - "Tram-track" appearance due to GBM splitting caused by mesangial ingrowth |
|
|
Which type of nephrotic syndrome is associated with C3 nephritic factor? Function? What type of deposits are seen in this type of nephrotic syndrome?
|
Type II Membrano-Proliferative Glomerulonephritis
- C3 nephritic factor stabilizes C3 convertase → ↓ serum C3 levels - Intramembranous immune complex (IC) deposits - "Dense deposits" |
|
|
What type of renal disease is Membrano-Proliferative Glomerulonephritis?
|
Nephritic syndrome that can also present with nephrotic syndrome
|
|
|
What causes the renal damage in Diabetic Glomerulonephropathy?
|
- Non-enzmatic glycosylation of GBM → ↑ permeability, thickening
- Non-enzymatic glycosylation of efferent arterioles → ↑ GFR → mesangial expansion |
|
|
What type of disease is Diabetic Nephropathy? What changes occur in this disease?
|
Nephrotic Syndrome
- Mesangial expansion - GBM thickening - Eosinophilic nodular glomerulosclerosis (Kimmelstiel-Wilson lesion) |
|
|
What makes a renal disease a "Nephritic syndrome"?
|
"I"nflammatory process
- When it involves glomeruli, it leads to hematuria and RBC casts in the urine - Associated with azotemia (abnormally high levels of nitrogen-containing compounds in blood), oliguria, hypertension (d/t salt retention), and proteinuria (<3.5 g/day) |
|
|
How do Nephrotic Syndromes and Nephritic Syndromes compare in terms of the proteinuria?
|
- Nephrotic Syndrome: >3.5 g/day
- Nephritic Syndrome: <3.5 g/day |
|
|
How do Nephrotic Syndromes and Nephritic Syndromes compare in terms of the urine casts?
|
- Nephrotic Syndrome: fatty casts
- Nephritic Syndrome: RBC casts |
|
|
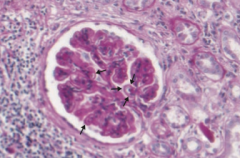
Which type of nephritic syndrome is associated with the following LM findings: glomeruli enlarged and hypercellular?
|
Acute Post-Streptococcal Glomerulonephritis
|
|
|
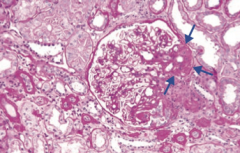
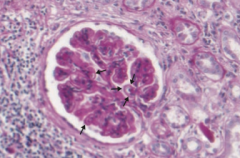
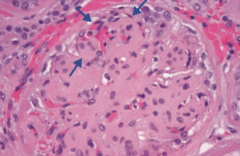
Which type of nephritic syndrome is associated with the following LM findings: crescent-moon-shape consisting of fibrin and plasma proteins (eg, C3b) with glomerular parietal cells, monocytes, and macrophages?
|
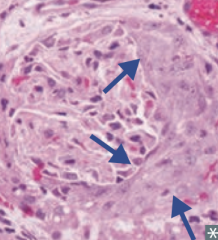
Rapidly Progressive (Crescentic) Glomerulonephritis (RPGN)
|
|
|
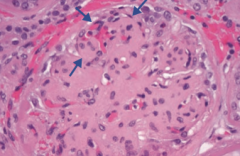
Which type of nephritic syndrome is associated with the following LM findings: wire looping of capillaries?
|
Diffuse Proliferative Glomerulonephritis (DPGN)
|
|
|
Which type of nephritic syndrome is associated with the following LM findings: mesangial proliferation?
|
IgA Nephropathy (Berger Disease)
|
|
|
Which type of nephritic syndrome is associated with the following EM findings: subepithelial immune complex (IC) humps?
|
Acute Post-Streptococcal Glomerulonephritis
|
|
|
Which type of nephritic syndrome is associated with the following EM findings: subendothelial and sometimes intramembranous IgG based immune complexes often with C3 deposition?
|
Diffuse Proliferative Glomerulonephritis (DPGN)
|
|
|
Which type of nephritic syndrome is associated with the following EM findings: mesangial immune complex deposits?
|
IgA Nephropathy (Berger Disease)
|
|
|
Which type of nephritic syndrome is associated with the following immunofluorescence findings: "starry sky" granular appearance ("lumpy-bumpy) due to IgG, IgM, and C3 deposition along GBM and mesangium?
|
Acute Post-Streptococcal Glomerulonephritis
|
|
|
Which type of nephritic syndrome is associated with the following immunofluorescence findings: crescent-moon-shape consisting of fibrin and plasma proteins (eg, C3b) with glomerular parietal cells, monocytes, and macrophages?
|
Rapidly Progressive (Crescentic) Glomerulonephritis (RPGN)
|
|
|
Which type of nephritic syndrome is associated with the following immunofluorescence findings: granular?
|
Diffuse Proliferative Glomerulonephritis (DPGN)
|
|
|
Which type of nephritic syndrome is associated with the following immunofluorescence findings: IgA based immune complex deposits in mesangium?
|
IgA Nephropathy (Berger Disease)
|
|
|
What type of renal pathology is Acute Post-Streptococcal Glomerulonephritis? Who is more likely to have this kind of damage? Cause?
|
Nephritic Syndrome
- Most frequently in children - Occurs ~2 weeks after group A streptococcal infection of pharynx or skin; type III hypersensitivity reaction - Resolves spontaneously |
|
|
What type of reaction mediates Acute Post-Streptococcal Glomerulonephritis?
|
Type III Hypersensitivity reaction (antigen-antibody complexes) to group A streptococcal infection of pharynx or skin
|
|
|
What renal pathology presents with peripheral and periorbital edema, dark urine (cola-colored), and hypertension? What lab values would you check?
|
Acute Post-Streptococcal Glomerulonephritis:
- ↑ Anti-DNase B titers - ↓ Complement levels |
|
|
What type of renal pathology is Rapidly Progressive Glomerulonephritis (RPGN)? What disease processes may result in this pattern?
|
Nephritic Syndrome:
- Goodpasture Syndrome - Granulomatosis with Polyangiitis (Wegener) - Microscopic Polyangiitis |
|
|
What type of renal pathology is caused by Goodpasture Syndrome? What findings are associated with this syndrome?
|
Rapidly Progressive Glomerulonephritis (RPGN)
- Type II hypersensitivity (antibodies produced by the immune response bind to antigens on the patient's own cells) - Abs to GBM and alveolar basement membrane → linear immunofluorescence - Presents with hematuria and hemoptysis |
|
|
What type of renal pathology is caused by Granulomatosis with Polyangiitis (Wegener)? What findings are associated with this syndrome?
|
Rapidly Progressive Glomerulonephritis (RPGN)
- PR3-ANCA / c-ANCA |
|
|
What type of renal pathology is caused by Microscopic Polyangiitis? What findings are associated with this syndrome?
|
Rapidly Progressive Glomerulonephritis (RPGN)
- MPO-ANCA / p-ANCA |
|
|
What is the prognosis for Rapidly Progressive Glomerulonephritis (RPGN)?
|
- Poor prognosis
- Rapidly deteriorating renal function (days to weeks) |
|
|
What is the most common cause of death in patient with SLE? What type of pathology is this?
|
Diffuse Proliferative Glomerulonephritis (DPGN)
- Can present as nephrotic syndrome and nephritic syndrome concurrently |
|
|
Which type of renal pathology often presents or flares with a URI or acute gastroenteritis? Signs?
|
IgA Nephropathy (Berger Disease) = Nephritic Syndrome
- Episodic hematuria with RBC casts |
|
|
Which type of renal pathology is caused by a mutation in type IV collagen? Implications?
|
Alport Syndrome = Nephritic Syndrome
- Thinning and splitting of glomerular BM - Presents with glomerulonephritis, deafness, and less commonly, eye problems |
|
|
What is the cause of Alport Syndrome?
|
- Mutation in type IV collagen → thinning and splitting of glomerular BM
- Most commonly X-linked |
|
|
Which type of renal pathology presents with glomerulonephritis, deafness, and less commonly eye problems?
|
Alport Syndrome
|
|
|
What type of disease is Acute Post-Streptococcal Glomerulonephritis? What changes occur in this disease?
|
Nephritic Syndrome
- Glomeruli enlarge and become hypercellular - IgG, IgM, and C3 deposition along GBM and mesangium leads to "Starry sky" granular appearance ("lumpy-bumpy) on immunofluorescence - Subepithelial immune complex (IC) humps |
|
|
What type of disease is Rapidly Progressive Glomerulonephritis? What changes occur in this disease?
|
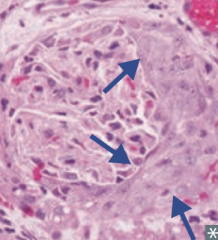
Nephritic Syndrome
- Crescent-moon shape consists of fibrin and plasma proteins (eg, C3b) with glomerular parietal cells, monocytes, and macrophages |
|
|
What type of disease is Diffuse Proliferative Glomerulonephritis (DPGN)? What changes occur in this disease?
|
Nephritic Syndrome
- "Wire looping" of capillaries - Subendothelial and sometimes intramembranous IgG-based immune complexes, often with C3 deposition - Granular appearance on immunofluorescence |
|
|
What type of disease is IgA Nephropathy? What changes occur in this disease?
|
Nephritic Syndrome
- Mesangial proliferation - Mesangial immune complex deposits - IgA based immune complex deposits in mesangium - Seen with Henoch-Schönlein purpura |
|
|
What type of disease is Alport syndrome? What changes occur in this disease?
|
Nephritic Syndrome
- Glomerulonephritis - thinning and splitting of glomerular BM - Deafness - Eye problems (less commonly) |
|
|
What diagnosis should you consider in a patient presenting with unilateral flank tenderness, colicky pain radiating to groin, and hematuria? Treatment/Prevention?
|
Kidney Stones
- Treat and prevent by encouraging fluid intake |
|
|
What are the potential complications of kidney stones?
|
- Hydronephrosis
- Pyelonephritis |
|
|
What are the types of kidney stones based on content? How common?
|
- Calcium (80%)
- Ammonium magnesium phosphate (15%) - Uric acid (5%) - Cystine (1%) |
|
|
What kind of kidney stones precipitate with ↑ pH?
|
- Calcium phosphate
- Ammonium magnesium phosphate |
|
|
What kind of kidney stones precipitate with ↓ pH?
|
- Calcium oxalate
- Uric acid - Cystine |
|
|
What kind of kidney stones appear radiopaque on x-ray?
|
- Calcium phosphate and calcium oxalate
- Ammonium magnesium phosphate - Cystine |
|
|
What kind of kidney stones appear radiolucent on x-ray?
|
Uric Acid (think radiol"U"cent for "U"ric acid)
|
|

If your patient presents with unilateral flank tenderness, colicky pain radiating to groin, and hematuria, and the following urine crystals are identified, what should you diagnose?
|

Calcium kidney stones
- This is the "envelope" type of calcium urine crystal - There is also a dumbbell shaped urine crystal |
|

If your patient presents with unilateral flank tenderness, colicky pain radiating to groin, and hematuria, and the following urine crystals are identified, what should you diagnose?
|

Ammonium magnesium phosphate kidney stones
- This is the "coffin lid" type of urine crystal |
|

If your patient presents with unilateral flank tenderness, colicky pain radiating to groin, and hematuria, and the following urine crystals are identified, what should you diagnose?
|

Uric Acid kidney stones
- Rhomboid or rosettes appearing urine crystals |
|
If your patient presents with unilateral flank tenderness, colicky pain radiating to groin, and hematuria, and the following urine crystals are identified, what should you diagnose?
|
Cystine kidney stones
- Hexagonal appearing urine crystals |
|
|
What is the most common kidney stone presentation?
|
Calcium oxalate stone in a patient with hypercalciuria and normalcalcemia
|
|
|
Calcium kidney stones can be composed of what? What promotes their formation?
|
- Content: calcium oxalate, calcium phosphate, or both
- Promoted by hypercalciuria: idiopathic or 2° to conditions that cause hypercalcemia such as cancer or ↑ PTH) |
|
|
What can cause calcium oxalate crystals to form?
|
- Ethylene glycol (anti-freeze)
- Vitamin C abuse - Crohn disease |
|
|
How do you treat patients with recurrent calcium kidney stones?
|
- Thiazide diuretics
- Citrate |
|
|
What type of renal pathology is also known as "struvite"?
|
Ammonium Magnesium Phosphate kidney stones
|
|
|
What causes Ammonium Magnesium Phosphate kidney stones / Struvite?
|
Infection with urease (+) bugs:
- Proteus mirabilis - Staphylococcus - Klebsiella These bugs hydrolyze urea to ammonia → urine alkalinization |
|
|
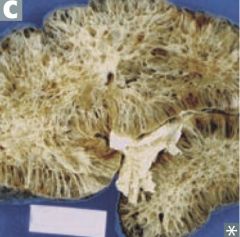
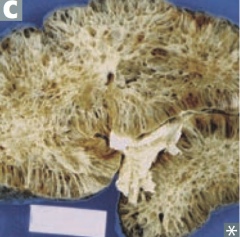
What are potential complications of Ammonium Magnesium Phosphate kidney stones / Struvite?
|

Staghorn calculi (picture) → can be a nidus for UTIs
|
|
|
How do you treat Ammonium Magnesium Phosphate kidney stones / Struvite?
|
- Eradicate underlying infection (Proteus mirabilis, Staphylococcus, or Klebsiella)
- Surgical removal of stone |
|
|
What type of kidney stone is likely to form in a patient with ↓ urine volume, acidic pH, and arid climate?
|
Uric Acid
|
|
|
How can you identify a Uric Acid kidney stone?
|
- Visible on CT and Ultrasound, but not on x-ray (radiolucent)
- Strongly associated with hyperuricemia (eg, gout) |
|
|
What are Uric Acid kidney stones associated with?
|
- Hyperuricemia (eg, Gout)
- Diseaes with ↑ cell turnover, such as leukemia |
|
|
How do you treat patients with Uric Acid kidney stones?
|
Alkalinization of urine
|
|
|
Who is more likely to get Cystine kidney stones? What is the most common cause?
|
- Mostly seen in children
- Secondary to cystinuria |
|
|
How can you diagnose a patient with having Cystine kidney stones?
|
- Sodium nitroprusside test is positive
- Look at crystals (hexagonal) |
|
|
What are the potential complications of Cystine kidney stones?
|

Can form staghorn calculi
|
|
|
How do you treat a patient with Cystine kidney stones?
|
- Alkalinization of urine
- Hydration |
|
|
What is the term for the distention / dilation of the renal pelvis and calyces?
|
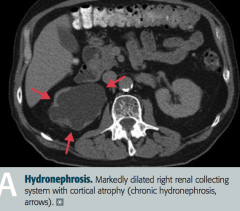
Hydronephrosis
|
|
|
What are the most common causes of Hydronephrosis?
|
- Urinary tract obstruction: eg, renal stones, BPH, cervical cancer, injury to ureter
- Retroperitoneal fibrosis - Vesicoureteral reflux |
|
|
What findings occur in Hydronephrosis? Complications?
|
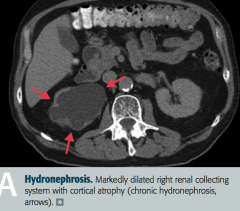
- Distention / dilation of renal pelvis and calyces proximal to site of pathology
- Only impairs renal function if bilateral or patient only has one kidney - Leads to compression atrophy of renal cortex and medulla |
|
|
What is the most common primary renal malignancy? Origin?
|
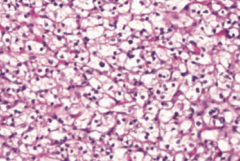
Renal Cell Carcinoma
- Originates from proximal tubule cells → polygonal clear cells (picture) filled with lipids and carbohydrates |
|
|
In whom is Renal Cell Carcinoma most common?
|
- Most common in men 50-70 years old
- ↑ incidence in patients who smoke and are obese |
|
|
What diagnosis should you consider in a patient with hematuria, a palpable mass, 2° polycythemia, flank pain, fever, and weight loss?
|

Renal Cell Carcinoma
|
|
|
What are the most common locations for Renal Cell Carcinoma to spread to? Significance?
|
- Invades renal vein then IVC to spread hematogenously
- Metastasizes to lung and bone - "Silent" cancer because it commonly presents as a metastatic neoplasm |
|
|
What genetic change is associated with Renal Cell Carcinoma?
|
Gene deletion on chromosome 3 (sporadic or inherited as von Hippel-Lindau syndrome)
RCC = 3 letters = chromosome 3 |
|
|
What is Renal Cell Carcinoma associated with?
|
Paraneoplastic syndromes:
- Ectopic EPO - Ectopic ACTH - Ectopic PTHrP |
|
|
How do you treat Renal Cell Carcinoma?
|
- Resection if localized disease
- Immunotherapy or targeted therapy for advanced / metastatic disease - Resistant to chemotherapy and radiation therapy |
|
|
What is the typical presentation of Renal Cell Carcinoma?
|
- Commonly silent because it often only presents once it has metastasized
- Hematuria - Palpable mass - 2° polycythemia - Flank pain - Fever - Weight loss |
|
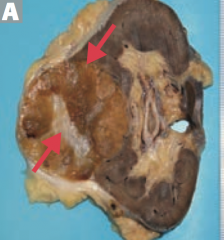
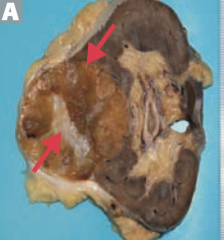
Which type of renal tumor presents as a well-circumscribed mass with a central scar? Benign or malignant? Source?
|
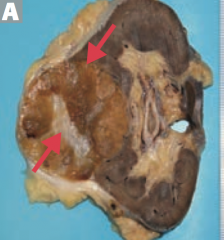
Renal oncocytoma
- Benign epithelial cell tumor |
|
|
What is the histologic appearance of a Renal Oncocytoma?
|
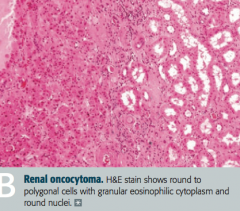
Large eosinophilic cells with abundant mitochondria without perinuclear clearing
|
|
|
What diagnosois should you consider in a patient who presents with painless hematuria, flank pain, and an abdominal mass? How should you treat?
|
Renal Oncocytoma
- Treat with nephrectomy |
|
|
What is the most common renal malignancy of early childhood (ages 2-4)?
|
Wilms Tumor (Nephroblastoma)
|
|
|
What kind of structures are in a Wilms Tumor (Nephroblastoma)?
|
Embryonic glomerular structures
|
|
|
What is the typical presentation of a Wilms Tumor (Nephroblastoma)?
|
- Child aged 2-4
- Huge, palpable flank mass - Hematuria |
|
|
What genetic change is associated with Wilms Tumor (Nephroblastoma)?
|
Loss of function mutations of tumor suppressor genes WT1 and WT2 on chromosome 11
|
|
|
If your patient with a Wilms tumor also has Aniridia (absence or iris), a genitourinary malformation, and mental retardation / intellectual disability, what diagnosis should you consider?
|
Beckwith-Wiedemann Syndrome or WAGR complex:
- Wilms tumor - Aniridia - Genitourinary malformation - mental Retardation (intellectual disability) |
|
|
What are the findings in the Beckwith-Wiedemann Syndrome?
|
WAGR complex:
- Wilms tumor - Aniridia - Genitourinary malformation - mental Retardation (intellectual disability) |
|
|
What is the most common tumor of the urinary tract system? Where can it occur specifically?
|
Transitional Cell Carcinoma
- Renal calyces - Renal pelvis - Ureters - Bladder |
|
|
A patient presents with painless hematuria without casts, what is the most likely diagnosis?
|
Bladder cancer (Transitional Cell Carcinoma)
|
|
|
What are the associated exposures in patients with Transitional Cell Carcinoma?
|
Problems in your Pee SAC:
- Phenacetin (pain-relieving and fever-reducing drug, banned in 80s) - Smoking - Aniline dyes - Cyclophosphamide |
|
|
What is the histologic appearance of Transitional Cell Carcinoma?
|
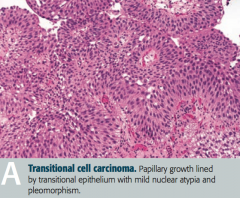
Papillary growth lined by transitional epithelium with mild nuclear atypica and pleomorphism
|
|
|
What types of cancer can occur in the bladder?
|
- Transitional cell carcinoma
- Squamous cell carcinoma of the bladder |
|
|
What causes squamous cell carcinoma of the bladder?
|
Chronic irritation of urinary bladder → squamous metaplasia → dysplasia and squamous cell carcinoma
|
|
|
What are the risk factors for squamous cell carcinoma of the bladder?
|
- Schistosoma haematobium infection (Middle East)
- Chronic cystitis - Smoking - Chronic nephrolithiasis |
|
|
If your patient from the Middle East presents with painless hematuria what diagnosis / cause should you consider?
|
Schistosoma haemotobium infection → chronic irritation of urinary bladder → squamous metaplasia → dysplasia and Squamous Cell Carcinoma of bladder
|
|
|
What diagnosis should you consider in a patient presenting with suprapubic pain, dysuria, urinary frequency, and urgency?
|
Acute infectious cystitis (bladder infection)
|
|
|
What are the risk factors for acute infectious cystitis?
|
- Female gender (short urethra)
- Sexual intercourse ("honeymoon cystitis") - Indwelling catheters |
|
|
What are the most common causes of acute infectious cystitis?
|
- E. coli (most common)
- Staphylococcus saprophyticus (sexually active young women - although E. coli still more common) - Klebsiella - Proteus mirabilis (urine has ammonia scent) - Adenovirus (hemorrhagic cystitis) |
|
|
What are the most common causes of acute infectious cystitis in young sexually active women?
|
- E. coli (most common)
- Staphylococcus saprophyticus |
|
|
Which cause of acute infectious cystitis is associated with an ammonia scent to the urine?
|
Proteus mirabilis
|
|
|
What infection causes hemorrhagic cystitis?
|
Adenovirus
|
|
|
What are the typical lab findings in acute infectious cystitis?
|
- Leukocyte esterase (+)
- Nitrites appear for G- organisms (especially E. coli) - Sterile pyruia with (-) urine cultures suggests urethritis (N. gonorrhoeae or Chlamydia trachomatis) |
|
|
What diagnosis should you consider in a patient with sterile pyuria and negative urine cultures?
|
Urethritis by Neisseria gonorrhoeae or Chlamydia trachomatis
|
|
|
What diagnosis should you consider in a patient presenting with dysuria, fever, costovertebral angle tenderness, nausea, and vomiting?
|
Acute Pyelonephritis
|
|
|
What are the most common causes of Acute Pyelonephritis?
|
- Ascending UTI (E. coli most common)
- Vesicoureteral reflux - Hematogenous spread of infection to kidney |
|
|
What lab / imaging findings are associated with Acute Pyelonephritis?
|
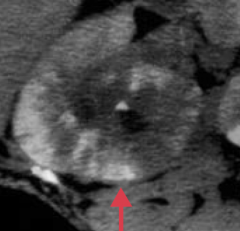
- White cell casts in urine
- CT: striated parenchymal enhancement |
|
|
What are the risk factors for Acute Pyelonephritis?
|
- Indwelling urinary catheter
- Urinary tract obstruction - Diabetes mellitus (sugar in urine = food for infection) - Pregnancy |
|
|
What are the possible complications of Acute Pyelonephritis?
|
- Chronic pyelonephritis
- Renal papillary necrosis - Perinephric abscess |
|
|
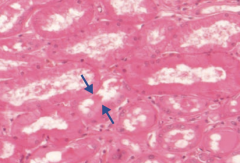
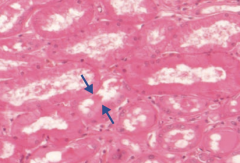
What is the histologic appearance of Acute Pyelonephritis?
|
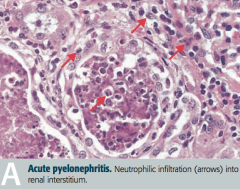
Neutrophilic infiltration (arrows) into renal interstitium
|
|
|
How do you treat Acute Pyelonephritis?
|
Antibiotics appropriate for cause
|
|
|
What is the cause of Chronic Pyelonephritis?
|
- Recurrent episodes of acute pyelonephritis
- Typically requires predisposition to infection such as vesicoureteral reflux or chronically obstructing kidney stones |
|
|
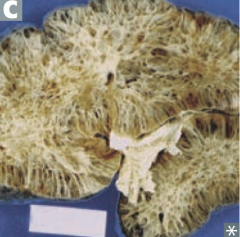
What is the histologic appearance of Chronic Pyelonephritis?
|
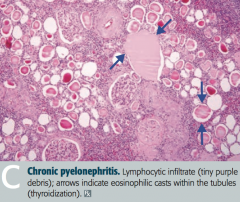
- Coarse, asymmetric corticomedullary scarring
- Blunted calyx - Tubules can contain eosinophilic casts that resemble thyroid tissue (thyroidization of kidney) = picture |
|
|
In what renal pathology is there "thyroidization of the kidney"?
|
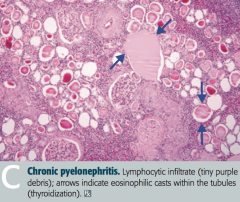
Chronic Pyelonephritis
- Tubules can contain eosinophilic casts that resemble thyroid tissue |
|
|
What diagnosis should you consider in a patient with fever, rash, hematuria, and costovertebral angle tenderness in a patient who has been taking a new drug for 1-2 weeks? What drugs are most likely to cause this?
|
Drug-Induced Interstitial Nephritis (Tubulointerstitial Nephritis)
- Diuretics - Penicillin derivatives - Sulfonamides - Rifampin - Can occur months after taking NSAIDs |
|
|
What changes occur in Drug-Induced Interstitial Nephritis (Tubulointerstitial Nephritis)?
|
- Acute interstitial renal inflammation
- Pyuria (classically eosinophils) - Azotemia (abnormally high levels of nitrogen-containing compounds in blood) |
|
|
How do drugs cause Drug-Induced Interstitial Nephritis (Tubulointerstitial Nephritis)?
|
Drugs act as "haptens" (elicit an immune response only when attached to a large carrier such as a protein), inducing hypersensitivity
|
|
|
What renal pathology is associated with obstetric catastrophes (eg, abruptio placentae)? Cause?
|
Diffuse Cortical Necrosis
- Acute generalized cortical infarction of both kidneys - Likely due to a combination of vasospasm and DIC |
|
|
What renal pathology is associated with septic shock? Cause?
|
Diffuse Cortical Necrosis
- Acute generalized cortical infarction of both kidneys - Likely due to a combination of vasospasm and DIC |
|
|
What causes Diffuse Cortical Necrosis?
|
- Acute generalized cortical infarction of both kidneys
- Likely due to a combination of vasospasm and DIC - Associated with obstetric catastrophes (eg, abruptio placentae) and septic shock |
|
|
What is the most common cause of intrinsic renal failure?
|
Acute Tubular Necrosis
|
|
|
What is the prognosis for Acute Tubular Necrosis?
|
- Self-reversible in some cases
- Can be fatal if left untreated - Death most often occurs during the initial "oliguric" phase |
|
|
What is the key identifying feature of Acute Tubular Necrosis?
|
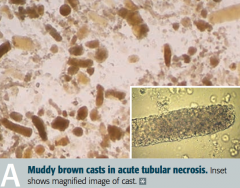
Granular "muddy brown" casts
|
|
|
What are the three stages of Acute Tubular Necrosis?
|
1. Inciting event
2. Maintenance phase - oliguric (small production of urine) 3. Recovery phase - polyuric (increased production of dilute urine) |
|
|
What is the first stage of Acute Tubular Necrosis?
|
Inciting event
- Ischemic injury - Nephrotoxic injury |
|
|
What is the second stage of Acute Tubular Necrosis, after the inciting event? Length? Characteristics?
|
Maintenance phase
- Oliguria (production of a small amount of urine) - Lasts 1-3 weeks - Risk of hyperkalemia and metabolic acidosis |
|
|
What is the third stage of Acute Tubular Necrosis, after the maintenance phase / oliguria? Characteristics?
|
Recovery phase
- Polyuria (production of large amounts of dilute urine) - BUN and serum creatinine fall - Risk of hypokalemia |
|
|
What can cause Acute Tubular Necrosis?
|
- Ischemic injury
- Nephrotoxic injury |
|
|
What can be responsible for an ischemic injury leading to Acute Tubular Necrosis? What does this lead to?
|
- 2° to ↓ renal blood flow (eg, hypotension, shock, sepsis, hemorrhage, CHF)
- Results in death of tubular cells that may slough into tubular lumen (proximal tubule and thick ascending limb are highly susceptible to injury) |
|
|
Which parts of the kidney are particularly susceptible to injury by ischemia?
|
- Proximal tubule
- Thick ascending limb of loop of Henle |
|
|
What can be responsible for a nephrotoxic injury leading to Acute Tubular Necrosis? What does this lead to?
|
- 2° to injury resulting from toxic substances (eg, aminoglycosides, radiocontrast agents, lead, cisplatin)
- Or 2° to crush injury (myoglobinuria) or hemoglobinuria - Proximal tubule is particularly susceptible to injury |
|
|
Which toxic substances can cause a nephrotoxic injury leading to Acute Tubular Necrosis?
|
- Aminoglycosides
- Radiocontrast agents - Lead - Cisplatin |
|
|
Which part of the kidney is particularly susceptible to nephrotoxic injury?
|
Proximal Tubule
|
|
|
What can cause gross hematuria and proteinuria?
|
Renal Papillary Necrosis
- Sloughing of renal papillae - May be triggered by a recent infection or immune stimulus |
|
|
What is Renal Papillary Necrosis associated with?
|
- Diabetes Mellitus
- Acute pyelonephritis - Chronic phenacetin use (acetaminophen is a phenacetin derivative) - Sickle cell anemia and trait |
|
|
What is the definition of Acute Kidney Injury (acute renal failure)?
|
- Abrupt decline in renal function
- ↑ Creatinine and ↑ BUN - Occurs over a period of several days |
|
|
What happens to BUN and creatinine in a normal nephron? Why?
|
- BUN is reabsorbed for countercurrent multiplication
- Creatinine is not reabsorbed |
|
|
What are the forms of acute kidney injury / acute renal failure?
|
- Pre-renal Azotemia
- Intrinsic Renal Failure - Post-renal Azotemia |
|
|
What happens to the kidney in Pre-Renal Azotemia? Why?
|
- ↓ GFR due to ↓ RBF (eg, hypotension)
- Na+, H2O, and urea are retained by the kidney in an attempt to conserve volume - ↑ BUN/creatinine ratio |
|
|
What happens to the kidney in Intrinsic Renal Failure? Why?
|
- Generally due to acute tubular necrosis or ischemia / toxins
- Less commonly due to acute glomerulonephritis (eg, RPGN) - Patchy necrosis leads to debris obstructing tubule and fluid backflow across necrotic tubule → ↓ GFR - Urine has epithelial / granular casts - BUN reabsorption is impaired → ↓ BUN/creatinine ratio |
|
|
What happens to the kidney in Post-Renal Azotemia? Why?
|
- Due to outflow obstruction (eg, stones, BPH, neoplasia, congenital anomalies)
- Develops only with bilateral obstruction |
|
|
Which type of acute kidney injury causes:
- Urine osmolality: >500 mOsm/kg - Urine Na+: <20 mEq/L - FENa: <1% (fractional Na+ excretion) - Serum BUN/Cr ratio: >20 Causes? |
Pre-Renal Azotemia
- As a result of ↓ RBF, eg, hypotension |
|
|
Which type of acute kidney injury causes:
- Urine osmolality: <350 mOsm/kg - Urine Na+: >40 mEq/L - FENa: >2% (fractional Na+ excretion) - Serum BUN/Cr ratio: <15 Causes? |
Intrinsic Renal Failure
- Generally due to acute tubular necrosis or ischemia/toxins - Less commonly due to glomerulonephritis (eg, RPGN) |
|
|
Which type of acute kidney injury causes:
- Urine osmolality: <350 mOsm/kg - Urine Na+: >40 mEq/L - FENa: >1% if mild, >2% if severe (fractional Na+ excretion) - Serum BUN/Cr ratio: >15 Causes? |
Post-Renal Azotemia
- Due to outflow obstruction (eg, stones, BPH, neoplasia, congenital anomalies |
|
|
What is the urine osmolality in Pre-Renal Azotemia vs Intrinsic Renal Failure vs Post-Renal Azotemia?
|
- Pre-Renal Azotemia: >500
- Intrinsic Renal Failure: <350 - Post-Renal Azotemia: <350 (in mOsm/kg) |
|
|
What is the urine Na+ in Pre-Renal Azotemia vs Intrinsic Renal Failure vs Post-Renal Azotemia?
|
- Pre-Renal Azotemia: <20
- Intrinsic Renal Failure: >40 - Post-Renal Azotemia: >40 (in mEq/L) |
|
|
What is the FENa (fractional sodium excretion) in Pre-Renal Azotemia vs Intrinsic Renal Failure vs Post-Renal Azotemia?
|
- Pre-Renal Azotemia: <1%
- Intrinsic Renal Failure: >2% - Post-Renal Azotemia: >1% (mild), >2% (severe) |
|
|
What is the serum BUN/creatinine ratio in Pre-Renal Azotemia vs Intrinsic Renal Failure vs Post-Renal Azotemia?
|
- Pre-Renal Azotemia: >20
- Intrinsic Renal Failure: <15 - Post-Renal Azotemia: >15 |
|
|
What are the consequences of renal failure?
|
MAD HUNGER:
- Metabolic Acidosis - Dyslipidemia (esp. ↑ TGs) - Hyperkalemia - Uremia - Na+/H2O retention - Growth retardation and developmental delay - Erythropoietin failure (anemia) - Renal osteodystrophy |
|
|
What are the two forms of renal failure? Causes?
|
- Acute: pre-renal azotemia, acute tubular necrosis, post-renal azotemia
- Chronic: hypertension, diabetes, congenital anomalies |
|
|
What is there an inability to do in renal failure?
|
Inability to:
- Make urine - Excrete nitrogenous wastes |
|
|
What acid/base disturbance is associated with renal failure?
|
Metabolic Acidosis
MAd hunger |
|
|
What lipid disturbance is associated with renal failure?
|
Dyslipidemia: especially ↑ TGs
maD hunger |
|
|
What electrolyte disturbance is associated with renal failure?
|
- Hyperkalemia
- Uremia - Na+/H2O retention mad HUNger |
|
|
What disturbances are there in children with with renal failure?
|
Growth retardation and developmental delay
mad hunGer |
|
|
What blood disturbance is associated with renal failure?
|
anemia due to Erythropoietin failure
(and platelet dysfunction due to uremia) mad hungEr |
|
|
What bone disturbance is associated with renal failure?
|
Renal osteodystrophy - causes subperiosteal thinning of bones
mad hungeR |
|
|
What are the characteristics of Uremia in renal failure?
|
↑ BUN and ↑ Creatinine, leads to:
- Nausea and anorexia - Pericarditis - Asterixis - Encephalopathy - Platelet dysfunction |
|
|
What causes renal osteodystrophy?
|
- Failure of vitamin D hydroxylation → ↓ 1,25-(OH)2-Vitamin D → ↓ intestinal Ca2+ absorption
- Hypocalcemia - Hyperphosphatemia also independently ↓ serum Ca2+ by causing tissue calcifications |
|
|
What happens in renal osteodystrophy due to the failure of vitamin D hydroxylation, hypocalcemia, and hyperphosphatemia?
|
- Subperiosteal thinning of bones
- 2° Hyperparathyroidism |
|
|
What are the types of renal cyst disorders?
|
- Autosomal Dominant Polycystic Kidney Disease (ADPKD)
- Autosomal Recessive Polycystic Kidney Disease (ARPKD) - Medullary Cystic Disease - Simple vs Complex Renal Cysts |
|
|
Which type of renal cyst disorder occurs more often in adults? Appearance of kidneys?
|
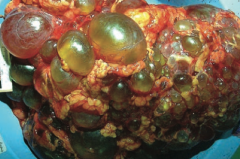
Autosomal Dominant Polycystic Kidney Disease (ADPKD)
- Innumerable cysts - Bilateral enlarged kidneys - Destroys kidney parenchyma |
|
|
What are the symptoms of a patient with Autosomal Dominant Polycystic Kidney Disease (ADPKD)?
|
- Flank pain
- Hematuria - Hypertension - Urinary infection - Progressive renal failure |
|
|
What is the cause of Autosomal Dominant Polycystic Kidney Disease (ADPKD)?
|
- 85% of cases: mutation in PKD1 on chromosome 16
- 15% of cases: mutation in PKD2 on chromosome 4 Autosomal dominant inheritance |
|
|
What are the complications and prognosis in patients with Autosomal Dominant Polycystic Kidney Disease (ADPKD)?
|
- Death from complications of chronic kidney disease or hypertension (caused by ↑ renin production)
- Associated with Berry aneurysms, mitral valve prolapse, and benign hepatic cysts |
|
|
Which type of renal cyst disorder occurs more often in infants? Appearance of kidneys?
|
Autosomal Recessive Polycystic Kidney Disease (ARPKD)
- Cysts in parenchyma |
|
|
What is Autosomal Recessive Polycystic Kidney Disease (ARPKD) associated with?
|
- Congenital hepatic fibrosis
- Potter sequence (if significant renal failure in utero) - Beyond neonatal period: hypertension, portal hypertension, progressive renal insufficiency |
|
|
What is the appearance of the kidneys in Medullary Cystic Disease?
|
- Medullary cysts usually not visualized
- Kidneys appear shrunken on ultrasound |
|
|
What damage occurs in Medullary Cystic Disease? Prognosis?
|
- Tubulointerstitial fibrosis
- Progressive renal insufficiency - Inability to concentrate urine - Poor prognosis |
|
|
What diagnosis should you consider in a patient with difficulty concentrating urine and shrunken kidneys on ultrasound?
|
Medullary Cystic Disease
|
|
|
What is responsible for the majority of all renal masses? Location?
|
Simple Renal Cysts - found in outer cortex
|
|
|
What are the findings of simple renal cysts?
|
- Found in outer cortex
- Filled with ultrafiltrate - Found incidentally and typically asymptomatic |
|
|
What kind of renal cyst increases the risk of renal cell carcinoma?
|
Complex Renal Cysts
|
|
|
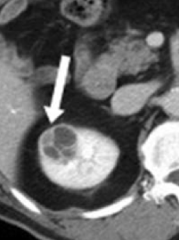
What is the appearance of Complex Renal Cysts? How should they be treated?
|
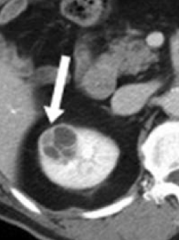
- Can be septated, enhanced, or have solid components, as seen on CT
- Require follow-up or removal due to risk of renal cell carcinoma |