Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
112 Cards in this Set
- Front
- Back
|
What is the normal range for CO?
|
4-8 L/min
|
|
|
What is the normal range for Cardiac Index?
|
2.5-4
|
|
|
What is the normal range for systemic vascular resistance? and systemic vascular resistance index?
|
800-1400, 1500-2400
|
|
|
What is the normal PCWP?
|
11 +- 4
|
|
|
What is the normal CVP?
|
7 +- 2
|
|
|
What is the normal pulmonary artery pressures?
|
20-30/6-15
|
|
|
What is the normal mixed venous oxygen saturation SvO2?
|
75+-5
|
|
|
What percentage of CO does the following organs get? kidney, brain, heart
|
25, 15, 5 respectively
|
|
|
What is the formula for MAP?
|
CO x SVR
|
|
|
What is the formula for ejection fraction?
|
stroke volume/EDV
|
|
|
Cardiac output increases with HR up to 120-150 bpm, then starts to go down, why?
|
decreased diastolic filling time
|
|
|
Atrial kick accounts for what % of LVEDV?
|
15-30%
|
|
|
Automatic increase in contractility secondary to increase in afterload. What is this effect called? What about automatic increase in contractility secondary to increased HR?
|
Anrep effect
Bowditch effect |
|
|
What is the normal O2 delivery-to-consumption ratio? What increases to keep this ratio constant?
|
5:1, CO
|
|
|
What is the normal SvO2?
|
75%
|
|
|
What measurement can be thrown off by pulmonary htn, aortic regurg, mitral stenosis, mitral regurg, high PEEP, porr LV compliance?
|
Wedge
|
|
|
What is the only way to measure pulmonary vascular resistance?
|
swan
|
|
|
Which zone of the lung do you place a swan?
|
zone III (lower lung)
|
|
|
Hemoptysis after flushing Swan. Name three interventions.
|
increase PEEP to tamponade the pulmonary artery bleed
mainstem intubate the nonaffected side, try to place a Fogarty down the affected side, may need thoracotomy and lobectomy |
|
|
Name two relative contraindications to a swan.
|
previous pneumonectomy, LBBB
|
|
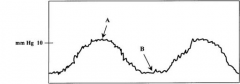
In this pulmonary artery wedge tracing, wedge pressure is measured at end expiration. Which point is for spontaneous breathing pts and which is for pts undergoing positive pressure ventilation?
|
A is for spontaneous, B is for vent
|
|
|
What are the two primary determinants of myocardial O2 consumption -> can lead to myocardial ischemia?
|
increased ventricular wall tension and HR
|
|
|
Why is LV blood 5 mmHg of PO2 lower than pulmonary capillaries?
|
unsaturated bronchial blood empties into pulmonary veins
|
|
|
What is the normal alveolar-arterial gradient in a non ventilated pt?
|
10-15 mmHg
|
|
|
Where is blood with the lowest venous saturation located?
|
coronary venous blood (30%)
|
|
|
Cardiovascular collapse; characteristically unresponsive to fluids and pressors.
|
Acute adrenal insufficiency
|
|
|
hyperpigmentation, weakness, weight loss, GI sx, increased K, decreased Na, fever, hypotension.
|
chronic adrenal insufficiency
|
|
|
Steroid potency:
1x - cortisone, hydrocortisone ___ - prednisone, prednisolone, methylprednisolone ___ - dexamethasone |
5x
30x |
|
|
Neurogenic shock - loss of sympathetic tone. Usually have decreased HR, decreased BP, warm skin. Tx?
|
give volume 1st, then phenylephrine after resuscitation; give steroids for blunt spinal trauma with deficit
|
|
|
What is the initial alteration in hemorrhagic shock?
|
increased diastolic pressure
|
|
|
What is the tx for cardiac tamponade?
|
fluid resuscitation initially; need pericardial window or pericardiocentesis
|
|
|
What is the CO and SVRI in hemorrhagic shock (increased or decreased)? and septic shock?
|
CO is decreased, SVRI is increased in hemorrhagic shock
CO is increased, SVRI is decreased in septic shock |
|
|
What is the triad of hyperventilation, confusion and respiratory alkalosis?
|
early sepsis triad
|
|
|
What is the insulin and glucose in early vs late gram-negative sepsis?
|
Early is decreased insulin and increased glucose due to impaired utilization
Late is increased insulin and increased glucose due to insulin resistance |
|
|
When does hyperglycemia occur in sepsis?
|
just before pt becomes clinically septic
|
|
|
What is activated protein C (Xigris) used for and what is the mechanism?
|
used for sepsis; mechanism is fibrinolysis
|
|
|
What stain can be used to find fat in sputum in urine to help dx fat emboli?
|
sudan red
|
|
|
PA systolic pressures >40, decreased PO2 and PCO2, respiratory alkalosis, chest pain, cough, dyspnea, increased HR
|
PE
|
|
|
What is the tx for air emboli?
|
place pt head down and roll to left to keep air in RV and RA then aspirate air out with central line or PA catheter to RA/RV
|
|
|
When is IABP used? what is the contraindication? what does it improve?
|
cardiogenic shock, aortic regurgitation, improves coronary perfusion
|
|
|
Name the receptor:
vascular smooth muscle constriction; gluconeogenesis, glycogenolysis |
Alpha 1
|
|
|
Name the receptor:
venous smooth muscle constriction |
Alpha 2
|
|
|
Name the receptor:
mycocardial contraction and rate |
Beta 1
|
|
|
Name the receptor:
relaxes bronchial smooth muscle, relaxes vascular smooth muscle; increases insulin, glucagon, rennin |
Beta 2
|
|
|
Name the receptor:
relax renal and splanchnic smooth muscle |
dopamine
|
|
|
Name the three receptors and associated effects for dopamine at low (0-5 ug/kg/min), medium (6-10), and high (>10) doses.
|
low - dopamine receptors (renal)
medium - beta-adrenergic (heart contractility) high - alpha-adrenergic (vasoconstriction and increased BP) |
|
|
What receptors and affects does dobutamine affect at low (5-15 ug/kg/min) and high (>15) doses.
|
low - beta-1 (increased contractility)
high - beta 2 (vasodilation, increased HR) |
|
|
Name the drug that is a phosphodiesterase inhibitor (Increases cAMP). Results in increased Ca flux and increased myocardial contractility. Also causes vascular smooth muscle relaxation and vasodilation.
|
Milrinone
|
|
|
What receptor does Phenylephrine affect?
|
alpha-1, vasoconstriction
|
|
|
What receptors does Norepinepherine affect at low and high doses?
|
Low - beta-1 (increased contractility)
High - alpha-1 and alpha-2 |
|
|
What receptors does Epinephrine affect at low and high doses?
|
Low - beta 1 and beta 2 (increased contractility and vasodilation). Can decrease BP at low doses.
High - alpha-1 and alpha-2 (vasoconstriction). Increased cardiac ectopic pacer activity and myocardial O2 demand. |
|
|
Name the drug that hits Beta-1 and beta-2 receptors, increasing HR and contractility, vasodilates. Side effects: extremely arrhythmogenic; increased heart metabolic demand (rarely used); may actually decrease BP.
|
Isoproterenol
|
|
|
Name the Vasopressin receptor:
vasoconstriction of vascular smooth muscle |
V-1
|
|
|
Name the vasopressin receptor:
water reabsorption at collecting ducts |
V-2 (intrarenal)
|
|
|
Name the vasopressin receptor:
mediate release of factor VIII and vWF |
V-2 (extrarenal)
|
|
|
What is the concern with Nipride (arterial and venous dilator)?
|
Cyanide toxicity at doses ?3 ug/kg/min for 72 hrs; check thiocyanate levels and signs of metabolic acidosis
|
|
|
How does nitroglycerin decrease myocardial wall tension?
|
decreasing preload
|
|
|
What is the MOA of hydralazine?
|
alpha blocker
|
|
|
What is the formula for compliance? What does high compliance lungs mean?
|
change in volume/change in pressure.
easy to ventilate |
|
|
Pts with ARDS, fibrotic lung disease, reperfusion injury, pulmonary edema all have reduce what?
|
pulmonary compliance
|
|
|
Which part of the lungs has the highest V/Q ratio? the lowest?
|
highest in upper, lowest in lower
|
|
|
On a ventilator what can be increased to improve oxygenation (alveoli recruitment) -> improves FRC
|
increased PEEP
|
|
|
On a ventilator what 2 things can be increased to decrease CO2?
|
increased rate or volume
|
|
|
Normal weaning parameters:
negative inspiratory force (NIF) > ___, FiO2 < ___% PEEP ___ (physiologic) pressure support 5, RR < ___ HR < ___ Po2 > ___ PCO2 < ___ pH 7.35-7.45 sats > 93% off pressors, follows commands, can protect airway |
negative inspiratory force (NIF) > 20,
FiO2 < 35% PEEP 5 (physiologic) pressure support 5, RR < 24 HR < 120 Po2 > 60 PCO2 < 50 pH 7.35-7.45 sats > 93% off pressors, follows commands, can protect airway |
|
|
Barotrauma on vent - high risk if plateus >___ and peaks >___ -> consider prophylactic ___
|
30,50, chest tubes
|
|
|
What does pressure support on a vent do?
|
decreases the work of breathing (inspiratory pressure is held constant until minimum volume is achieved)
|
|
|
Excessive PEEP complications include decreased RA filling, decreased CO, decreased renal blood flow and decreased urine output and increased ___
|
pulmonary vascular resistance
|
|
|
What 3 types of pts where high frequency ventilation is used?
|
kids, tacheoesophageal fistula, bronchopleural fistula
|
|
|
Why is inverse ratio ventilation used? (normal 1:2 I:E phase; go to 2:1)
|
helps reduce barotrauma
|
|
|
What is the formula for minute ventilation?
|
TV x RR
|
|
|
What class of lung disease is represented by decreased TLC, decreased RV, decreased FVC, FEV1 can be normal or increased?
|
restrictive lung disease
|
|
|
What class of lung disease is represented by increased total lung capacity, increased residual volume and decreased FEV1?
|
obstructive lung disease
|
|
|
What is the most common cause of ARDS?
|
sepsis
|
|
|
Acute Lung Injury is defined by acute onset, bilateral pulmonary infiltrates, PaO2/FiO2 < 300, PAOP < 18 mmHg or no clinical evidence of LAH. What one additional criteria defines acute respiratory distress syndrome?
|
PaO2/FiO2 < 200
|
|
|
What two cytokines mediate SIRS?
|
TNF-alpha and IL-1
|
|
|
What are the 4 SIRS criteria?
|
Temp >38 or <36
RR >20 or Pco2 < 32 WBC >12,000 or <4000 HR >90 |
|
|
SIRS -> Sepsis -> Septic Shock -> ___
|
MOD (Progressive but reversible dysfunction of 2 or more organs arising from an acute disruption of normal homeostasis)
|
|
|
What is the name of the syndrome of chemical pneumonitis from aspiration of gastric secretions.
|
Mendelson's
|
|
|
Most common cause of fever in the first 48 hours after operation?
|
atelectasis
|
|
|
What effect does the following have on the lungs?
bradykinin, PGEi, prostacyclin (PGI2), nitric oxide |
pulmonary vasodilation
|
|
|
What effect does the following have on the lungs?
histamine, serotonin, TXA2, epinephrine, norepinephrine, hypoxia, acidosis |
pulmonary vasoconstriction
|
|
|
What effect does alkalosis have on pulmonary vasculature? and acidosis?
|
alkalosis - pulmonary vasodilator
acidosis - pulmonary vasoconstrictor |
|
|
What does nitroprusside, nitroglycerine, and nifedipine do to the pulmonary vasculature?
|
pulmonary shunting
|
|
|
What is the most common cause of postoperative renal failure?
|
hypotension
|
|
|
What percentage of nephrons need to be damaged before renal dysfunction occurs?
|
70%
|
|
|
What is the best test for azotemia?
|
FeNa
|
|
|
What are the three steps to treating Oliguria?
|
1st make sure pt is volume loaded (CVP 11-15 mmHg), 2nd try diuretic trial (Lasix or butanamide)
3rd dialysis if needed |
|
|
Renin is released in response to decreased pressure sensed by ___ in kidney. Also in response to increased Na concentrations sensed by ___
|
juxtaglomerular apparatus, macula densa
|
|
|
What does renin do?
|
converts angiotensinogen to angiotensin I
|
|
|
What converts angiotensin I to angiotensin II?
|
angiotensin converting enzyme in the lung
|
|
|
What structure releases aldosterone in response to angiotensin II?
|
adrenal cortex
|
|
|
What specifically does aldosterone do to the kidney?
|
Acts on distal convoluted tubule ATPase to increase resorption of water and sodium and secretion of potassium.
|
|
|
What does atrial natriuretic peptide do to the kidney? to the blood vessels?
|
inhibits Na and water resorption at the collecting ducts
vasodilator |
|
|
What specifically does ADH do to the kidney? the blood vessels?
|
Acts on the collecting ducts for water resorption
vasoconstrictor |
|
|
How do NSAIDs cause renal damage?
|
Inhibit prostaglandin synthesis, resulting in renal arteriole vasoconstriction
|
|
|
How do aminoglycosides cause renal damage?
|
direct tubular injury and later renal vasoconstriction
|
|
|
Myoglobin causes direct renal tubular injury. What is the tx?
|
alkalinize urine
|
|
|
Contrast dyes cause direct tubular injury. What is the tx?
|
premedicate with N-acetylcysteine and volume
|
|
|
The following things preclude what diagnosis?
uremia, temp <30, BP <70/40, desaturation with apnea test, drugs, metabolic derangements |
brain death
|
|
|
How long must the following exist to declare brain death:
unresponsive to pain, absent caloric oculovestibular reflexes, absent oculocephalic reflex, positive apnea test, no corneal reflex, no gag reflex, fixed and dilated pupils. |
6-12 hours
|
|
|
What two testing modalities can be used to prove absence of brain activity?
|
EEG - electrical silence
MRA - will show no blood flow to brain |
|
|
Apnea test – disconnected from ventilation; CO2 >___ mm Hg or increase in CO2 by ___ is a positive test for apnea. If arterial pressure drops to <60 or patient desaturates, the test is terminated
|
60, 20
|
|
|
Can you still have deep tendon reflexes with brain death?
|
yes
|
|
|
What does carbon monoxide do to a pulse oximeter?
|
Can falsely increase reading
|
|
|
What does carbon monoxide do to hemoglobin?
|
binds hemoglobin directly creating carboxyhemoglobin
|
|
|
What is an abnormal carboxyhemoglobin level? and in smokers?
|
>10%, >20%
|
|
|
What is tx for carbon monoxide poisoning?
|
100% O2 on a ventilator; may need hyperbaric O2 if really high
|
|
|
Methemoglobinemia can occur from nitrites such as Hurricaine spray; nitrites bind Hgb. What is the O2 saturation? What is the tx?
|
85%, methylene blue
|
|
|
Critical illness polyneuropathy – motor > sensory neuropathy; occurs with ____; can lead to failure to wean from ventilation
|
sepsis
|
|
|
In endothelial cells, forms toxic oxygen radicals with reperfusion, involved in reperfusion injury. Also involved in the metabolism of purines and breakdown to uric acid
|
Xanthine oxidase
|
|
|
When do seizures occur with ETOH withdrawal?
|
48 hrs
|
|
|
ICU (or hospital) psychosis generally occurs after which postoperative day? What do you need to rule out?
|
3rd, metabolic and organic causes
|