Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
37 Cards in this Set
- Front
- Back
|
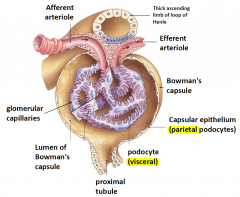
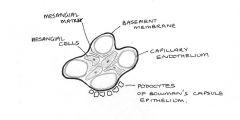
Structure of the glomerulus
|
|
|
|
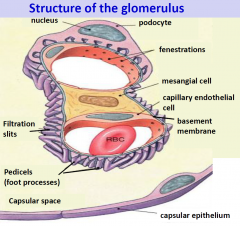
Structure of the glomerulus: EM
|
|
|
|
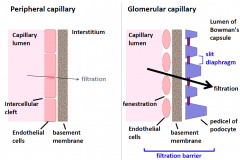
Comparison of filtration across peripheral and glomerular capillaries
|
|
|
|
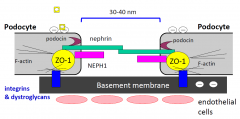
Composition of slit diaphragm
|
|
|
|
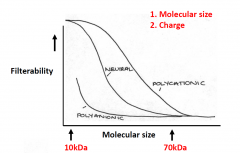
Semipermeable nature of the filtration barrier
|
|
|
|
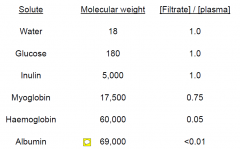
Examples of solute filtration
|
|
|
|
Glomerular mesangial cells
|
1. Contractile
contraction - AngII, ADH, growth factors, endothelin relaxation - ANP, NO, PGE2 2. Secrete mesangial matrix 3. Behave like macrophages 4. Hormones, cytokines, growth factors -> contraction & proliferation 5. Secrete growth factors & cytokines -> autocrine / paracrine actions |
|
|
Glomerular filtration rate Depends on
|

|
|
|
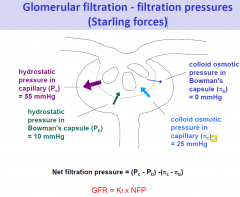
Glomerular filtration - filtration pressures (Starling forces)
|
|
|
|
Filtration pressure along the glomerular capillary
|
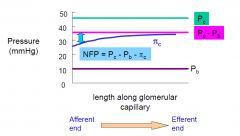
•net filtration pressure 's along length of glomerular capillary because c 's
|
|
|
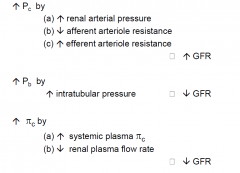
Changes in filtration pressures affect GFR
|
|
|
|
Glomerular capillary blood pressure and GFR
|

|
|
|
Regulation of GFR
|
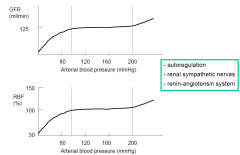
- autoregulation
- renal sympathetic nerves - renin-angiotensin system |
|
|
Renal autoregulation of GFR
INTRINSIC METHODS |
1.Myogenic mechanism
2.Tubuloglomerular feedback mechanism |
|
|
Myogenic mechanism
|
smooth muscle in afferent arteriole
- contracts when stretched - relaxes when released from stretch afferent BP contraction of arterioles blood flow |
|
|
Tubuloglomerular feedback
|
|
|
|
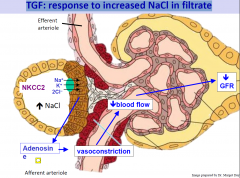
TGF: response to increased NaCl in filtrate
|
|
|
|
TGF: response to decreased NaCl in filtrate
|
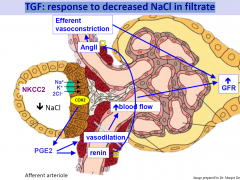
also NO can be releases by the macula densa cells
|
|
|
Perturbations of tubuloglomerular feedback
|
Bartter’s syndrome – NKCC2 mutation -> increased renin -> vasodilation of afferent -> increase GFR
Loop diuretics – block TGF by blocking NKCC2 -> increase GFR -> increases efficacy of these diuretics |
|
|
Extrinsic regulation of GFR
|
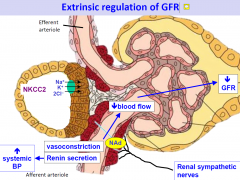
can over-ride the intrinsic mechanisms
|
|
|
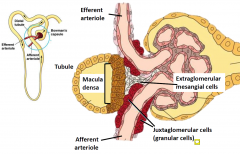
Juxtaglomerular apparatus
|
Juxtaglomerular apparatus serves two functions in fluid homeostasis:
1. Vascular feedback control of GFR = tubuloglomerular feedback fast response - minute to minute controller 2. NaCl - dependent control of renin secretion and synthesis slow response to prolonged changes |
|
|
Pathophysiological changes affecting the filtration barrier
|
Two categories of glomerular disorders
1. Nephrotic syndrome (nephrosis) -affects integrity of glomerular filtration barrier -metabolic disorders (eg diabetes) -autoimmune disorders (eg Lupus) 2. Nephritic Syndrome (nephritis) –involves inflammatory response within glomerulus –can affect any layer –causes injury due to (a)Circulating antibody-antigen complexes trapped in filtration membrane (b)Antibodies reacting with glomerular antigens |
|
|
Symptoms characterised by proteinuria
|
•Resorptive capacity of proximal tubule exceeded –> low MW proteins in urine
•Glomerular filtration problem –> proteins >69 kDa in urine (mainly albumin) due to:- (a)impairment of charge selectivity (eg minimal change nephropathy, microalbuminergic stage of diabetic nephropathy) (b) impairment of size filter - podocytes / mesangial cells |
|
|
Pathophysiological changes relating to podocytes
|
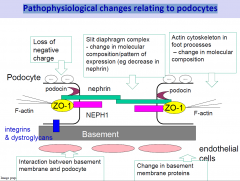
occurs in many forms of glomerular disease
(eg. membranous glomerulopathy, diabetes mellitus) Early events characterised by changes in molecular composition -> affects slit diaphragm, foot process structure -> fusion of filtration slits -> can be reversed eg AngII inhibitors, ACE inhibitors If early structural changes not reversed -> severe and progressive glomerular damage Podocytes can’t undergo regenerative proliferation |
|
|
Mesangial cell changes
|
Injury to mesangial cells in diseases such as diabetes mellitus and glomerular nephritis due to:
(a) metabolic injury (eg high plasma glucose inhibits contraction) (b) immunological injury Early stages/ acute damage –> damage mesangial cells & filtration barrier –> local inflammatory response - release of NO -> relaxation of mesangial cells –> hyperfiltration and proteinuria Later stages / chronic damage –> mesangial cell proliferation, production of mesangial matrix –> filtration impaired |
|
|
Why does filtration occur?
|
Filtration occurs because of the high pressure in the glomerular capillaries (PGC). The glomerular capillaries are unique in that they lie between two arterioles, the afferent arteriole and the efferent arteriole. Because of the added resistance of the efferent arteriole, PGC is higher than pressure in a typical capillary.
|
|
|
Measuring GFR?
Ideal Substance |
Ideal substance:
•Exclusively filtered, not reabsorbed or secreted •Production is constant and unaffected by medications, age, patient size |
|
|
Inulin Clearance
|
•Inulin is a plant carbohydrate that is neither reabsorbed nor secreted
•The clearance of inulin is completely due to filtration. •Inulin is not an endogenous substance, therefore it must be infused. •Impractical in clinical practice |
|
|
Creatinine
|
•An endogenous substance derived from the metabolic breakdown of creatine, a component of skeletal muscle
•Creatinine is almost exclusively filtered with only a small amount of secretion •Muscle mass influences creatinine level •A significant rise in creatinine only starts to occur when almost 50% of renal function is lost |
|
|
eGFR
|
•In CKD, Creatinine is used to estimate GFR (via CKD-epi equation)
•eGFR assumes a steady state situation so it is not appropriate to use an eGFR in acute kidney injury |
|
|
Kidney Autoregulation
|
One would think that changes in the systemic blood pressure would cause changes in PGC and thus, changes in the GFR. In healthy individuals, this does not occur because of renal autoregulation. Renal autoregulation involves feedback mechanisms intrinsic to the kidney that cause either dilation or constriction in the afferent arteriole so as to counteract blood pressure changes and keep a steady GFR
|
|
|
Regulation of glomerular filtration rate
|

|
|
|
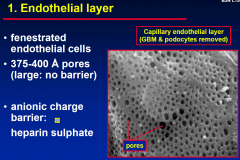
1. Endothelial Layer
|
|
|
|
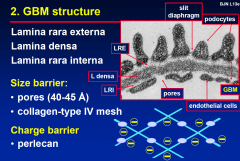
2. GBM Structure
|
|
|
|
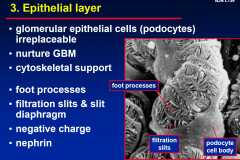
3. Epithelial Layer
|
|
|
|
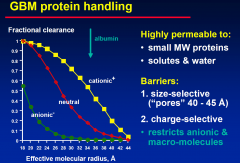
GBM Portein Handling
|
|
|
|
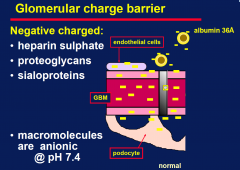
Glomerular charge barrier
|
|