![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
101 Cards in this Set
- Front
- Back
|
Micro-organisms associated with xanthogranulomatous pyelonephritis |
Proteus species and E. coli |
|
|
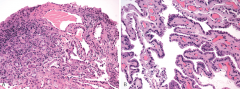
Xanthogranulomatous pyelonephritis. Collection oflipid-laden macrophages in a background of acute and chronic inflammatorycells. |
|
|
Tumors associated with Von Hippel–Lindau |
angiomatosis
hemangioblastomas pheochromocytoma renal cell carcinoma pancreatic serous cystadenoma pancreatic islet endolymphatic sac tumor bilateral papillary cystadenomas of the epididymis (men) broad ligament of the uterus (women). |
|
|
Gene of Von Hippel–Lindau
|
von Hippel–Lindau tumor (vHL) suppressor gene on chromosome 3p25 |
|
|
Causes of bilateral polycystic kidney |
Autosomal dominant polycystic kidneydisease
Acquired cystic kidney disease Tuberous sclerosis von Hippel Lindau |
|
|
EM finding in oncocytoma |
Numerous mitochondria |
|
|
Oncocytoma stains how? Hale's colloidal iron |
negative or only stains luminalcytoplasm |
|
|
Chromophobe stains how with Hale's colloidal iron |
Positive |
|
|
Angiomyolipoma assocaited with |
tuberous sclerosis multiple and bilateral when associated with tuberous sclerosis |
|
|
Renal medullary carcinoma |
Sickle cell trait or disease <40 years old |
|
|
Renal medullary carcinoma compact adenoid cysticappearance or reticular growth pattern;reminiscent of testicular yolk sac tumor mucoid, myxoid,or edematous areas are typical findings Negative INI-1 |
|
|
Tumors associated with tuberous sclerosis |
Giant cell astrocytoma (CNS)
Cortical tubers (CNS) Subependymal nodules (CNS) angiomyolipomas (Kidney) Lymphangioleiomyomatosis (Lungs) Rhabdomyomas (heart) angiofibromas (face skin) Periungual fibromas (Koenen's tumors under nails), Hypomelanic macules ("ash leaf spots"): White or lighter patches of skin Shagreen patches: thick leathery skin orange peel (Back or neck skin) astrocytic hamartomas (or "phakomas") (retina) |
|
|
Collagenous micronodules (mucinous hyperplasia) - suggests prostate cancer |
|
|
Adenomatoid tumor |
|
|
Immunophenotype of Adenomatoid tumor |
Positive: Mesothelial markers (thrombomodulin, HBME-1,CK5/6, OC125, calretinin, and cytokeratin, D2-40) positive Negative for: CEA, Leu-M1, inhibin, and factor VIII |
|
|
Adenomatoid tumor clinical features |
paratesticular tissues 20 and 40 years of age painless, unilateral, solitary, solid mass |
|
|
Most common peritesticular tumor in adults |
Liposarcoma arise from spermatic cord; |
|
|
Yolk sac tumor; pure vs when it is mixed germ cell |
Pure for pediatric group part of mixed germ cell in adults |
|
|
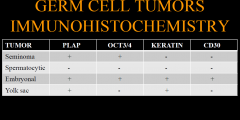
IHC in germ cell tumors |
|
|
|
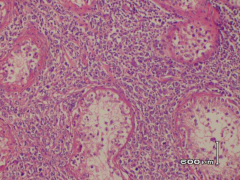
interstitial growth pattern between seminiferous tubules think lymphoma |
|
|
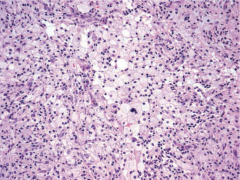
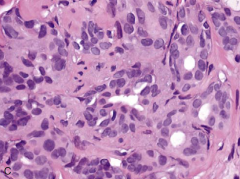
Malakoplakia. The lamina propria contains numeroushistocytes with a large amount of eosinophilic granular cytoplasm andintracytoplasmic inclusions (Michaelis-Gutmann bodies).
|
|
|
Michaelis-Gutmann bodies are formed by
|
precipitation of calcium or iron on bacteria or bacterial fragments |
|
|
Polypoid cystitis is often seen in patients with |
indwelling bladder catheters radiation treatment |
|
|
Follicular cystitis is frequently seen in patients with |
bladder carcinoma urinary tract infection radiation treatment |
|
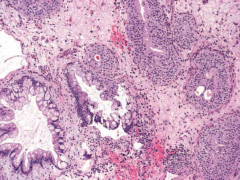
bladder |
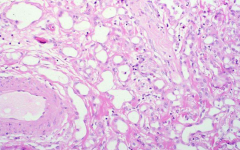
Cystitis cystica et glandularis. The lamina propriashows cystically dilated glands lined by urothelial cells sometimes has glandular metaplasia with intestinal-type goblet cells |
|
|
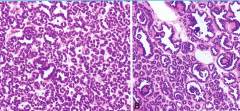
NEPHROGENIC ADENOMA clinical features
|
young adult male (2:1) after genitourinary surgery or renal transplantation associated with calculi, trauma, and cystitis polypoid exophytic mass |
|
|
nephrogenic adenoma |
|
|
Cytogenetics of urothelial carcionoma |
deletion of chromosome 9p is associatedwith superficial disease
abnormalities involvingchromosome 17p are associated with disease progression aneuploidy involving chromosomes 3, 7, and 17 |
|
|
UroVysion is designed to detect |
aneuploidy for chromosomes 3, 7, 17, and loss of the 9p21 |
|
|
IHC of adenocarcinoma of bladder |
Positive: CK7, CK20, Leu M1 (CD15), CEA, cytoplasmic Beta catenin |
|
|
Cytogenetics of inflammatory myofibroblastic tumor of bladder |
Translocation involving chromosome 2p23, site of theALK gene 70% positive for ALK IHC |
|
|
embryonal rhabdomyosarcoma can be dividedinto two basic forms with prognostic impact
|
1) polypoid, mostly intraluminal, associated with favorable prognosis(grapelike clusters, botryoid subtype),
2) deeply invasivetumors with a worse prognosis |
|
|
Genetrics of autosomal recessive polycystic kidney disease |
(PKHD1) mutation on chromosome 6p21-23: encodesfor polyductin or fibrocystin |
|
|
Genetrics of autosomal dominant polycystic kidney disease |
chromosome 16(16q13.3) in 85% of patients (involves PKD1 gene,which encodes a protein named polycystin 1) chromosome 4 (4q21-23) in approximately15% of cases (PKD2 gene, which encodesa protein named polycystin 2) |
|
|
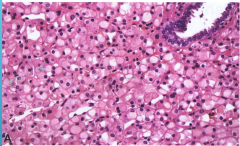
EPITHELIOID ANGIOMYOLIPOMA
|
Potentially malignant mesenchymal neoplasm withlow metastatic potential |
|
|
Associations with PAPILLARY ADENOMA |
hemodialysis acquired cystic disease chronicpyelonephritis von Hippel-Lindausyndrome trisomy 7or 17, loss of Y chromosome in male patients |
|
in kidney |
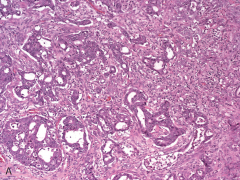
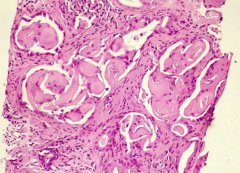
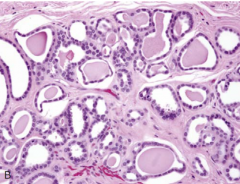
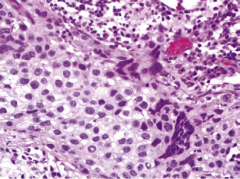
Metanephric adenoma. tightly packed tubulopapillarystructures within an acellular stroma background. Note the sharpborder with the kidney |
|
|
Metanephric adenomaclinical features |
female (2:1) 50% symptomatic (Hematuria abd pain) 15% with polycythemia 1 cm to 15 cm |
|
|
EM findings of Metanephric adenoma |
Electron microscopy: cells have basal lamina andmicrovilli |
|
|
genetics of Metanephric adenoma |
BRAF V600E mutations in 90% |
|
|
IHC of oncocytoma |
Positive: CK7, S100A1, E-cadherin, Claudin 8 Negative: Vimentin, Hale’s colloidal iron stain |
|
|
Genetics of clear cell RCC |
Chromosome 3p deletion (majority of sporadic) VHL,PBRM1, BAP1, and SETD2 Mutation of the VHL gene in 34% to 56% |
|
|
cytogenetics of oncocytoma |
loss of chromosomes Y and 1. |
|
|
oncocytoma is associated with what syndrome |
Birt-Hogg-Dube´ syndrome |
|
|
Birt–Hogg–Dubé syndrome
|
Autosomal dominant; folliculin (FLCN) gene fibrofolliculomas, trichodiscomas, acrochordons chromophobe-oncocytoma hybrid tumors |
|
|
IHC for extramammaryPaget disease (EM-PD)
|
positive: EMA, CEA, CK19, CK7, and GCDFP15 Her2/neu geneamplification can be present and might be of importancetherapeutically. |
|
|
clear cell sarcoma of the kidney translocation |
t(10;17) |
|
|
translocationassociatedrenal cell carcinoma |
t(6;11)(p21;q12) --> MALAT1-TFEB "MiTF/TFE translocation carcinoma family" |
|
|
genetics of cellular variant mesoblastic nephroma |
t(12;15)
|
|
|
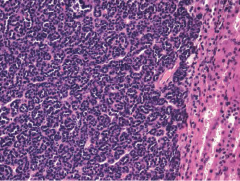
neuroblastoma has elevation of what biochemicals |
dopamine, homovanillic acid (HVA), vanillylmandelic acid (VMA) |
|
|
which PCKD has dilated collecting ducts, and have a distinctive linear radiating appearance. |
autosomal recessive has dilated collecting ducts autosomal dominant involves all parts of kidney |
|
|
IHC of seminoma |
Positive: C-kit, PLAP, cytoplasmic PAS(glycogen), HCG (syncitialtroph) Weak: keratin Negative: EMA |
|
|
IHC of paraganglioma |
Positive: NSE, chromogranin, S100(sustentacular cells only) Negative: keratins |
|
|
clinical features of choriocarcnoma of testis |
usually part of mixed germ cell tumor rarely a pure choriocarcnoma 20-30s, never before puberty fequently present with symptoms of mets hCG is high testis is normal or small "burned out" thyrotoxicosis |
|
|
Genetic abnormality of clear cell RCC |
Chromosome 3p deletion in the majority of sporadic clear cell RCC The four most commonly mutated genes are VHL, PBRM1, BAP1, and SETD2 |
|
|
genetic abnormality with papillary RCC |
trisomy 7, 17,
loss of Y chromosome |
|
|
clinical features of juxtaglomerular apparatus (JGA) tumor |
uncontolled hypertension (renin) hyperaldalsterone and hypokalemia tight pack epitheliod cells with rhomboid crystals (renin crystals) vimentin, SMA positive |
|
|
interstitial cystitis |
controversial diagnosis of exlusion ulcerated or denuded epithelium mast cells in all layers of bladder wall |
|
|
Kleinfelter syndrome at increased risk for |
seminiferous tubule sclerosis nodules of leydig breast carcinoma elevated FSH and LH |
|
|
Tumors that stain for PSA or PSAP |
Prostate breast Salivary |
|
|
tumors positive for AMACR |
prostate renal lung colon breast others |
|
|
IHC of neuroblastoma |
NSE synaptophysin chromogranin, neurofilament protein (+/-) |
|
|
poor prognostic factors of neuroblastoma
|
MYCN amplification mitosis-karyorrhexis index (MKI) >200 <2 years 1 p deletion in children younger than 1 year A serum ferritin >150 ng/mL |
|
|
features of adrenal cortical carcinoma |
>5 per 50 HPF mitoses <25% of clear cellsm(except oncocytic type) female predominance Necrosis |
|
|
Urovysion is approved for which patients |
with hematuria personal Hx of urothelial cancer |
|
|
IHC of embryonal carcinomas of the testis |
Positive: pancytokeratin, OCT3/4, andCD30 negative: EMA |
|
|
Carney syndrome
|
Large cell calcifying Sertoli cell tumor myxomas of skin, soft tissue, and heart pituitary adenomas melanocytic schwannomas fibroadenomas cutaneous blue nevi can be seen in Peutz-Jeghers syndrome |
|
|
Gonadoblastoma
|
a mix of germ cells and sex cord cells Seminoma and sertoli cells Considered an in situ neoplasm excellent prognosis All patients have a Y chromosome and are wither 46XY and X/XY mosaicism with preserved mullerian duct-derived structures |
|
|
Bacteria causing acute bacterial prostatitis |
E. coli (80%) or other gram negative |
|
in prostate? |
Postatrophic hyperplasia (benign) Hypermethylation in theupstream “CpG island” in the GSTP1 gene, shortening of CAG repeat lengths, or Chromosome 8 centromeric gain |
|
in prostate? |
HYPERPL ASIA OF MESONEPHRICREMNANTS |
|
|
IHC of prostatic stromal tumors of uncertain malignant potential(STUMPs) |
Positive: CD34, vimentin, SMA (variable), progesterone receptor |
|
|
IHC for RENAL MEDULLARY CARCINOMA |
positive: keratin, CEA, EMA, andCK19 absence of INI-1 expression aremarkers of aggressive behavior |
|
|
Congenital adrenal hyperplasia is A.K.A.
|
adrenogenital syndrome |
|
|
Congenital adrenal hyperplasia: genetics and effects |
rare autosomal recessive condition 21-hydroxylase deficiency No cortisol sometimes no aldosterone (salt wasting --> death) and excess androgen Females: virilization Males: hypogonadism, testicular tumors |
|
|
ANDROGEN INSENSITIVITY SYNDROME effects
|
organs resistant to androgen stimulation (androgen receptor mutation) testicular feminization (severe) or normal male with infertility (mild) Male: pseudohermaphroditism, B/L cryptorchidism, Female: primary amenorrhea |
|
|
KLINEFELTER SYNDROME biomarkers |
High GSH Variable LH |
|
|
IHC for SEMINOMA
|
Positive: PLAP, CD 117, OCT3/4 (nuclear staining),SALL4, and vimentin Negative: cytokeratins, epithelialmembrane antigen (EMA), CD30, AFP, and hCG |
|
|
genetics of SEMINOMA |
Isochromosome (12p) 20% C-kit gene amplification 12% activating mutations of C-kit |
|
|
IHC for SPERMATOCYTIC SEMINOMA |
50% c-kit positive negative: for germ cell markers such asOCT3/4, AE1/3, and CD30 |
|
|
genetics of SPERMATOCYTIC SEMINOMA |
gain of chromosome 9 gain of X chromosome |
|
|
IHC for EMBRYONAL CARCINOMA |
Positive: CD30, OCT3/4 (nuclear), SALL4 (nuclear), PLAP (weaker), cytokeratins, AFP (focal) Negative: CD117, EMA, CEA, vimentin, and hCG |
|
|
genetics of EMBRYONAL CARCINOMA |
Isochromosome (12p) more copy numbers of i12p is bad |
|
|
YOLK SAC TUMOR biochemical marker |
usually AFP high |
|
|
IHC of YOLK SAC TUMOR |
Positive: AFP (patchy), SALL4, α-1-antitrypsin, glypican-3,PLAP (patchy/weak), cytokeratins Negative: CD117, OCT3/4, and hCG |
|
|
genetics of YOLK SAC TUMOR |
Loss of chromosomes 1p and 6q Gain of chromosomes 1q, 12q, 20q, 22 |
|
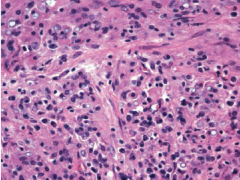
? in testis |
CHORIOCARCINOMA syncytiotrophoblast cells (large, multinucleatedcells with large irregular nuclei), cytotrophoblastcells (pale cytoplasm with single largenucleus and prominent nucleolus), and intermediatetrophoblast cells (clear cytoplasm, larger than cytotrophoblastswith single nuclei) extensive hemorrhage and necrosis |
|
|
cytoplasm inclusions that are only seen in Leydigcells, |
Reinke crystals |
|
|
Leydig cell tumor features
|
Leydig cells, Reinke crystals, Lipofuscin deposition, fibrous bands separating tumor nodules (some cases) architectural: solid (mostcommon), cordlike, pseudoglandular, adipose-like, andmicrocystic. |
|
|
IHC for Leydig cell tumor |
positive: vimentin, calretenin, inhibin A, Melin-A (maybe), p53 (maybe), BCL2 (maybe) Negative: keratins |
|
|
IHC for SERTOLI CELL TUMOR |
Positive: vimentin, keratins, EMA, inhibin Negative: PLAP, OCT 3/4, CD30 |
|
|
IHC of EXTRAMAMMARY PAGET DISEASEOF PENIS AND SCROTUM |
Positive for CEA, LMWK, CK7, EMA Negative: HMWK, PSA,S100 protein, HMB45 |
|
|
AFP elevations are seen in |
yolk-sac tumors and embryonal carcinoma also:Pregnancy, hepatocellular carcinoma, cirrhosis, and hepatitis |
|
|
bhCG elevations are seen in |
Choriocarcinoma, embryonal carcinoma, yolk sac, mixed germ cell, and a minority of seminomas (< 10%) also:prostate, bladder, ureteral, and renal cancers |
|
|
Lactate dehydrogenase (LDH) level correlates well with |
the tumor burden and with the number of i(12p) copies |
|
|
i(12p) |
NONSEMINOMATOUS GERM CELL TUMORS (NSGCTs): 1) EMBRYONAL CARCINOMA2) YOLK SAC TUMOR (ENDODERMAL SINUS TUMOR)3) CHORIOCARCINOMA4) MIXED GERM CELL TUMOR |
|
|
syndrome associated with NONSEMINOMATOUS GERM CELL TUMORS |
30 to 40 times > in Klinefelter syndrome |
|
|
HCG above 500 IU indicates which germ-cell |
a choriocarcinoma component |
|
|
Helpful in differentiating renal medullary carcinoma from collecting duct carcinoma |
Medullary has loss of INI-1 |
|
|
Succinate Dehydrogenase Deficiency RCC Loss of SDHB protein IHC Double-hit inactivation ofone of SDH gene family – most commonly SDHB |
|
IHC? |
Metanephric adenoma +WT-1 +CK7 +EMA |