![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
149 Cards in this Set
- Front
- Back
|
Interosseous |
4 dorsal - abductors 3 palmar - adductors UN Contribute to MCP flex and IP ext. Insert prior to Lumbricals thru sagittal band. |
|
|
Lumbricals |
Originate on radial side FDP. Pass volar to Transverse MC lig. Insert onto radial aspect of Extensor hood (obl fibres). Inervated MN (radial 2), UN (ulna 2) Contribute to IP ext. |
|
|
Intrinsic tightness |
PIP flexion less with MCPJ held in extension (Intrinsics on stretch, extrinsics relaxed). Extrinsic tightness - PIP flex less with MCPJ held in flexion. |
|
|
DR post reduction bench marks (AAOS) |
Radial shortening < 3mm Dorsal articular tilt < 10 deg Intraarticular step off < 2mm. |
|
|
XR measurements DR |
Radial height 11mm Radial inclination 22 deg Volar tilt 11 deg Ulna variance. |
|
|
Blood supply to scaphoid |
Main, dorsal branch radial art. enters dorsal ridge just distal to waist, and flows in retrograde fashion towards proximal pole. |
|
|
Indications for ORIF scaphoid |
1mm displacement Humpback deformity >35deg Trans scaphoid perilunate Volar approach potentially avoids disruption to BS and is most commonly employed. Union rates 90%. |
|
|
Scaphoid non union with humpback |
FISK open wedge interposition graft to restore length and angulation. |
|
|
Osteonecrosis and non union |
Presence of intra op punctate bleeding is most reliable sign of vascular proximal pole. Vascularised BG. Harvested from dorsal aspect DR based on 1,2 intercompartment supraretinacular A. |
|
|
SNAC wrist |
Distal portion flexes, proximal pole into extension (SL lig). Stage 1 - Radioscaphoid arthritis Stage 2 - Involvement of scaphocapitate joint Stage 3 - Lunocapitate joint. Options; Radial styloidectomy, PRC, 4 corner with scaphoid excision. wrist fusion. |
|
|
Triquetrum # |
Dorsal capsular avulsion. |
|
|
Hook of Hamate # |
Often from blunt trauma to palm. Associated with sports gold, baseball hockey, tennis. Symptomatic who fail cast immobilisation treated with excision. |
|
|
Carpal instability |
Spectrum of injury from predynamic to dynamic to static. |
|
|
CID |
Carpal instability dissociative (CID). between individual carpal bones of single row. DISI / VISI. |
|
|
CIND |
Carpal instability non dissociative (CIND) between rows such as midcarpal or radiocarpal. Midcarpal - Clunking of wrist, nil Hx of truma. sudden shift of proximal row with ulna or radial deviation. Most patients have lig laxity. non op Mx. Radiocarpal - high energy. Ulna translocation of carpus signifies global ligamentous disruption. |
|
|
DISI |
SL disruption Dorsal fibres are stronger. Scaph flexs, lunate extends. Dorsal wrist pain when loading, decreased grip strength. shift test. XR SL ang > 70deg, >3mm apart. Clench fist (dynamic SL). MRI and wrist arthroscopy. Acute repair. Chronic open reduction and pinning with dorsal capsulodesis (if not a SLAC) |
|
|
SLAC |
Chronic static instability Stage 1 - OA scaphoid and RS Stage 2 - OA scaphoid and scaphoid fossa. Stage 3 - Capitate migrates proximally and get midcarpal OA Options; RSectomy, PRC, 4 corner, fusion. |
|
|
Volar extrinsic Lig |
Radioscaphocapitate Long radiolunate Short radiolunate Radioscaphoidolunate (testut) contains NV structures. |
|
|
Perilunate dislocations |
Dorsiflex, ulna dev and supination. Mayfield Dual approach. Immoblise for a long time. |
|
|
POSI |
Position of safe immoblisation (Intrinsic plus hand) Wrist 15 - 30 deg ext MCPJ 70 - 90 deg flexion IP in neutral. Immobilise 3-4 wks at most. |
|
|
MC neck fracture |
Intrinsic muscles ar emajor deforming forces and lead to apex dorsal. Check rotation and lag. 20 / 30 / 40 / 70 deg angulation is acceptable. Jahss maneuver. |
|
|
MC shaft |
associated with higher risk malrotation. 5 degs of mal rotation leads to 1.5 cm digit overlap. Acceptable angulation 10 / 10 / 30 / 30 deg. every 2mm shortening 7 deg lag. upto 5mm acceptable. |
|
|
Bennett # |
Intra articular # dislocation. APL and thumb extensors cause proximal, dorsal and radial displacement of shaft.
Beak ligament keeps base reduced to trapezium
|
|
|
Skier's thumb |
UCL injury. 85% cases stener lesion, which adductor pollicis aponeurosis is interposed. maybe palpable on examination. |
|
|
MCPJ dislocation |
Dorsal - most common. Skin dimpling in distal palm pathognomoic. Simple P1 perched. traction and hyperext avoided. Reduce by flex wrist and direct pressure. Complex P1 and MC in bayonet position and interposition of volar plate. usually need to open. Volar approach (can go either) NV at risk. A1 pulley released to loosen noose are MC head. |
|
|
Boxers knuckle |
Most common hand injury in boxers. Extensor hood of MCP joint ruptured. Presents with swelling, reduced ROM and occasional extensor lag. Rx with primary repair. |
|
|
P1, P2 # |
P1 deform with apex volar angulation. P2 deform with apex dorsal or volar. Apex dorsal if # proximal to FDS insertion. Apex volar if # distal to FDS insertion. Majority Rx non op. if < 10deg angulation and no rotation deformity. Immobilise 3 wks then aggressive physio. Radiographic union lags by several weeks. |
|
|
PIPJ dislocations (dorsal) |
Dorsal most common. Injury to volar plate and 1 colateral. Simple - middle phalanx contact with a condyle. reduce with longitudinal traction. Complex - bayonet appearance. volar plate blocks reduction. Reduce by hyperextension then palmar force. Buddy strape is sufficient. if ongoing instability then dorsal block splint. Often ass with # P2 base If need to open then dorsal approach, and incision between central slip and lateral band. |
|
|
PIPJ dislocations (volar) |
Injury to central slip and a colateral. Splint in full extension 6 wks post reduction. (Central slip rupture) Inadequate Rx will lead to boutonniere deformity. |
|
|
PIPJ Rotatory dislocation |
One of the phalangeal condyles is buttonholed between central slip and lateral band. Often requires open reduction. |
|
|
PIPJ # dislocation |
Often un recognised. Must make sure joint stays reduced. is usually avulsion of Volar plate. <40% surface dorsal block splint allow active flexion, ext is slowly progressed over 4 wks. >40% ORIF or volar plate arthroplasty. Pilon # Rx with dynamic distraction Ext fix. |
|
|
DIPJ dislocations |
CR immoblised in slight flex with dorsal splint 2 wks. Irreducible has volar plate in it needs open . |
|
|
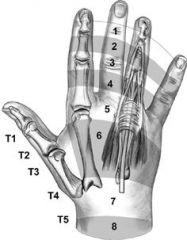
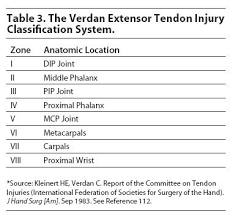
Extensor tendon zones |
|
|
|
Extensor tendon zones |
|
|
|
Extensor tendon injury |
< 50% nil need to fix, ROM to prevent adhesion. |
|
|
Zone 1 ext tendon injury |
Mallet. if < 12 wks acute splint full time 6 wks then part time 4 wks. If joint is enlocated on XR. otherwise ORIF, or K wire. if > 12 wks chronic if joint supple try splint, if contracture, dynamic splint, if swan neck (dorsal sublux of lateral bands) fowlers central slip tenotomy, if OA then arthrodesis. |
|
|
Zone 2 Ext tendon injury |
Over middle phalanx. over proximal phalanx of thumb. Direct repair if > 50%. |
|
|
Zone 3 Ext tendon injury |
over PIPJ (central slip). MCPJ thumb IF open - direct repair. Esson test. Acute boutonniere results from central slip disruption and volar sublux of lateral bands resulting in DIP hyperextension. IF closed - full time PIPJ ext splint 6 wks followed by part time 4 wks. DIP flexion maintained during Rx. Chronic central slip reconstruction or Arthrodesis. |
|
|
Zone 4 Ext tendon injury |
Over proximal phalanx or MC thumb. if > 50% direct repair. Problems with adhesions in this zone result in loss of flex. |
|
|
Zone 5 Ext tendon injury |
Over MCPJ or CMC thumb. if > 50% repair. Fight needs WO and debridement, ABx against Eikenella corrodens. |
|
|
Sagittal band rupture |
Forced extension of flexed digit. Can lead to extensor tendon sublux or dislocation. Finger held in Flex position no active ext. Passive extension if possible and patient can often hold it in that position. Acute injuries Ext slint MCPJ in ext 4-6wks. Otherwise repair or reconstruction. |
|
|
Zone 6 Ext tendon injury |
Most common. over MC. >50% repair early protected ROM. |
|
|
Zone 7,8 Ext tendon injury |
7 @ wrist. Repair retinaculum, adhesion common. Spint in POSI. |
|
|
Flexor tendon injuries |
Concomitant NVI common. Note resting posture hand, and tenodesis effect of wrist. FDP has common muscle belly and must be tested while blocking other digits. FDS individual muscle belly and can be tested together. Partial lac associated with gap formation or triggering with non op Rx. |
|
|
Basic surgical repair |
Strength of repair proportional to number of suture strands that cross site. Larger diameter suture decrease gap formation. Locking loop decreases gap formation. Epitendinous repair decreases gap and increase overall strength by 10-50%. Purchase should be 1 cm of lac. Repair of flexor tendon sheath has no effect. Risk of re rupture is @ 3wks and occurs at knots use of early active flexion protocol post op needs at least 4 strand. |
|
|
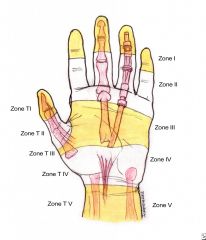
Flexor tendon zones |
|
|
|
Zone 1 flexor injury |
Rugger jersey Avulsion of FDS insertion. Mechanism of forced Ext of DIP during grasping. Leddy and Packer. 1 - FDP retracted to palm repair 7-10 days. 2 - intact vincula prevent retraction past PIPJ 6wk 3 - boney avulsion 6 wks. |
|
|
Quadrigia |
If FDP tendon advanced (middle, ring ,small) occurs because of common muscle belly. will compromise flexion of the adjacent digits. also results in forearm pain. |
|
|
Zone 2 flexor injury |
In sheath, between FDS insertion and distal crease. FDP and FDP involved. tendon injury maybe different level to skin injury. Direct repair. early ROM to prevent adhesions. 50% patients need tenolysis. |
|
|
Zone 3 flexor injury |
Between palmar crease and CT. Better outcome with repair. Lumbricals originate from FDP. |
|
|
Post op rehab Flexor tendons. |
Duran protocol (if patient can be trusted) uses other hand to perform passive digit flexion exercises. Active extension allowed. Restrict AROM 6 wks. |
|
|
Stenosing tenosynovitis |
women over 50yo, DM inflam arthritis Repetitive grasping. Inflam of flexor tendon sheath. 60% respond to CSI into flexor tendon sheath. DM have a poorer response to injection. If fail surgical release. |
|
|
De Quervain tenosynovitis |
1st compartment APL/EPB middle aged women, new mothers, golfers. Finkelstien test. Non Op - brace, activity mod, CSI (80% success). If fail surgical release. Dorsal retinaculum to prevent volar subluxation. Anatomic variation, APL may have multiple slips (2-4). EPB can be in own compartment. |
|
|
Intersection syndrome |
Junction bw 1st and 2nd compartment. Affects rowers, weight lifters. tender/swelling 4-5cm distal to radiocarpal joint. Non op rest,ice, NSAID, CSI into second compartment. If fails surgical release of second compartment and debridement of bursa. |
|
|
Acute calcific tendonitis |
FCU most common Over use syndrome with resisted wrist flexion. Acute wrist pain and swelling. Fluffy calcium on xR. Oral steroids, NSIAD, ice, immobilisation. |
|
|
ECU tendonitis |
tetherd by fibroosseous sheath. Overuse tendonitis racquet sports. MRI thickening, tears. Non Op. |
|
|
ECU subluxation Traumatic |
Forced hypersupination and ulnar deviation. May hear snap, maybe reproducible. Early diagnosis, long arm cast with wrist held in in pronation and slight radial dev. Chronic requires repair or reconstruction of extensor retinaculum +/- deepening of groove. Associated with TFCC tears in 50% cases. |
|
|
Components of TFCC |
Dorsal and volar radioulnar ligaments Articular disc Meniscus homologue ECU subsheath Origins of ulnolunate and ulnotriquetral ligaments. Deep fibres insert into ulna fovea termed ligamentum subcruentum. |
|
|
TFCC tears |
type 1 traumatic type 2 degenerative (from abutment) acute traumatic initially Rx with immobilization. if fail arthroscopy or open repair / debridement. degenerative = ulna shortening osteotomy. |
|
|
DRUJ |
Instability - fracture etc. ECU can block reduction. May need K wires. OA - Sauve-Kapandji procedure. |
|
|
Nail structure |
nail plate composed of keratin. Originates from germinal matrix. Sterile matrix under nail. Lunula is junction of the above 2. Hyponychium skin at tip of finger Eponychium (cuticle) proximal nail fold skin Paronychium forms the lateral margins skin |
|
|
Hook Nail |
May result from tight nail bed repair. Distal advancement of matrix Loss of underlying bony support |
|
|
Post nail bed repair |
High incidence of finger tip hypersensitivity and or cold intolerance for up to 1 year. Nail takes 3-6 months to grow back. |
|
|
Lumbrical plus finger |
When FDP insertion is violated. As patient goes to flex finger, FDP tendon retacts and creates tension on extensor mechanism through its lumbrical, causing paradoxical IP joint extension. Treat with release of radial lateral band. |
|
|
Options for finger tip loss |
Without out bone exposed. Allowed to heal by secondary intention if less than 1 cm. Bone exposed. Cross finger flap, thenar flap, V-Y advancement. Moberg advancement for thumb. Otherwise shortening of bone and closing. Do not violate FDP insertion as get a lumbrical plus finger. |
|
|
Flap classification by tissue type |
Single.
Fascia, Muscle (Lat, gastroc), Bone. Composite Cutaneous - skin and subcutaneoue tissue. Fasciocutaneous - fascia with overlying skin. Musculocutanous - with muscle, and over lying skin. |
|
|
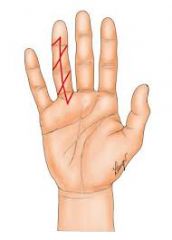
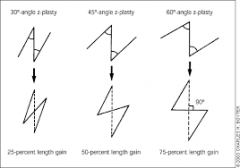
Z plasty along finger |
|
|
|
Z plasty basics |
|
|
|
Traumatic amputation |
Indications for replant. thumb, multiple digits, wrist, in kid. Contraindications to replant. Single digit (esp index) Crush or mangled Prolonged ischemia (6hrs warm, 12hrs cold). Level of amputation in zone 2 of flexor Patient is idiot. |
|
|
Sequence of replant |
Bone stabilisation (usually with shortening) Extensor tendon repair Flexor tendon repair Arterial reanastomosis Venous reanastomosis Nerve Skin. |
|
|
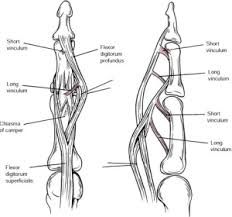
FDP avulsions. Rugger Jersey finger.
|
Leddy and Packer classificationI Vinculae are ruptured, tendon retracts to palm (must be treated <10days otherwise 2 stage revision)
II Vinculae intact, tendon remains at PIPJ (Operate within 6wks) III Large bony fragment, ensnared beyond A4 pulley (Operate within 6wks) |
|
|
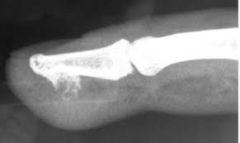
Acro–Osteolysis
|
Absorption of distal tuft of phalanx
DDx Psoriasis, Scleroderma / Raynauds, Frost Bite, Hyperparathyroidism, Diabetes, Vasculitis, Leprosy,RA, rarelyGout |
|
|
SLE
|
ANA, dsDNA. Auto immune disorder.
Get distension of joint from synovitis rather than destruction. Pannus not as aggressive. Migratory polyarthraliga, Flexor tenosynovitis, MCP PIPJ OA, AVN carpus. Butterfly rash, pericarditis, glomerulonephritis. XR effusions, subluxation, juxtacortical osteopenia. Ortho soft tissue balancing |
|
|
CREST Syndrome |
1. Calcinosis 2. Raynaud's 3. Esophageal Strictures 4. Sclerodactyly 5. Telangiectasia |
|
|
Scleroderma
|
Small vessel disease with fibrosis of many organs. HandsStiff shiny digits Loss of creases Acral tapering of digits Autoamputation (acro–osteolysis) Telangiectasia Calcium nodules Extraskeletal Lung fibrosis CRF |
|
|
Psoriasis |
Psoriasis. Autoimmune disease. Seronegative arthritis. DDx from RA. asymmetrical distribution, seronegative, psoriatic rash, nail changes. pitting. Less aggressive. Typically more DIP involved.
Hand XR. Asymm, no periarticular osteopenia, periosteal bone all MC shafts. DIPJ. Pencil in cup, P3 tuff resorption. |
|
|
Tooth Knuckle Injuries. Organisms
|
50% rates infection. SA, OM, teno
Polymicrobial – streptococci – Staphylococci – Eikenella (quater, GNB, synergistically with strep. can be resistantto diclox). – anaerobes. Need wash out in theatre. Take deep samples direct Abx. Start with IV penicillin. |
|
|
Rolando #
|
Rolando Fracture.
2 small intra articular fragments, Poor prognosis. Op Mx for significant displacement. Dorsal approach, Plate. |
|
|
Rheumatoid Arthritis Diagnostic criteria.
|
1987 American College of Rheumatology Need 4/7 (MAX RANS)
1. Morning Stiffness 2. Arthritis of 3 areas > 6/52 3. Xray changes 4. Rh factor 5. Arthritis of Hand > 6/52 6. Nodules 7. Symmetric Arthritis > 6/52 |
|
|
Types of surgery for RA
|
1. Synovectomy / Capsulorrhaphy
2. Tenosynovectomy 3. Tendon surgery & soft tissue balancing 4. Arthroplasty 5. Arthrodesis |
|
|
Nalebuff Classification MCPJ
RA |
MCPJ RA
Stage I – Synovitis– medical Rx and splinting– synovectomy Stage II – Synovitis + Ulna deviation– medical treatment and splinting– synovectomy + soft tissue reconstruction Stage III – Moderate joint destruction– volar subluxation and ulnar drift– soft tissue reconstruction possible– arthroplasty gives more reliable results Stage IV – Advanced joint destruction– fixed joint deformities– arthroplasty with soft tissue releases |
|
|
Swan Neck
|
DIPJ – terminal extensor tendon rupture or attenuated.
PIPJ – volar capsule stretching / FDS rupture– contracted central extenor slip MCPJ – intrinsic tightness – extrinsic weakness / MCPJ subluxation and subluxation extensor apparat |
|
|
Boutonniere Finger
|
Problem
– rupture of central slip. LAteral bands displace volar Solution – flexible – Matev's central slips reconstruction– radial lateral band to central slip– ulna lateral band to radial lateral band insertion |
|
|
Bunnell test
|
Assess interossei Tightness.
– hand dorsum up – correct ulna deviation – extend MCPJ & comment on active PIPJ range – flex MCPJ & comment on active PIPJ range Positive – PIPJ flexion less in MCPJ extension than with MCPJ flexion – interossei are tighter in extension |
|
|
RA Thumb
|
NaleBuff.
Type 1 – Boutonniere. Most common (MP flex, IP Hext) Type 2 – doesnt exist any more Type 3 – Swan neck. Second most common. Primary deformity is OA of CMC, then hyperExt MPJ and IPJ flexion. Type 4 – game keepers (synovitis) Fusion. Type 5 – stretched volar plate MCPJ. Differes from SN due to no CMC OA. Type 6 – Arthritis Mutilans, distruction and instability. |
|
|
Sagittal bands V Lateral bands
|
Sagittal bands
– stabilise EDC – extend MCPJ Lateral bands – lumbricals extended PIPJ |
|
|
Dorsal Blocking wire for Mallet |
Antigrade wire into Distal Phalanx. Flexion of DIPJ. Blocking wire inserted thru fragment or just proximal to it then into p2. DIPJ Extended 1st wire driven across joint. |
|
|
Zone 2 Extensor tendon injuries
|
If have some active DIPJ extension at least one Lateral band intact.
Rx in splint (3 wks) If nil active extension both lateral bands gone Rx surgical repair. |
|
|
Zone 3 Extensor tendon injuries.
|
Central slip ruptured at PIPJ. (Elsons test)
Deformity not present at time of injury usually develops 2–3wks later. Develop Boutonniere deformity. If lateral bands sublux volar this creates DIPJ hyperextension. Closed injury with full ROM of IPJs Rx in extension splint (PIPJ) 4 wks. If FFD PIPJ the progressive splint (Capener Splint) Open or large Avulsion with bone Rx surgical. |
|
|
Extensor Tendon Repairs Zone 5 – 9
|
Excellent results of repair 5 proximal zones
Only 50% excellent results 4 distal zones. Lacerations >50% zones V–VIII should be repaired. Important to maintain length as will decrease flexion. Dynamic splint. Improves results, prevent adhesions of flexors. Outrigger with passive extension. |
|
|
Flexor Pulleys |
A1, A5 expendable A2, A4 +/– A3 loss = Bowstring A2, A4 fibro osseous, srise from periosteum, maintain short moment arm. A1,3,5. arise from volar plates. Single pulley ruptures Rx non op. Multiple pulley rupture repiars do poor therefore reconsturction |
|
|
Define Endo, Epi, paratenon Synovial sheaths.
|
Endotenon – surrounds the individual collagen bundles
Epitenon – fine fibrous outer layer, highly cellular. contains most of the blood vessels & capillaries Paratenon – thin visceral layer of adventitia. Provides nutrition & allows gliding Synovial Sheaths – in distal palm & fingers, visceral synovial layer enclosing FDS/FDP– parietal layer continuous with the pulleys |
|
|
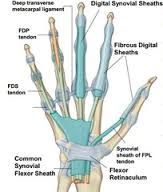
Synovial sheaths in Hand
|
|
|
|
Quadriga
|
Issue FDP of MF / RF / LF linked
– will only extend as much as of shortest tendon – if limited excursion of one FDP due to repair. – present with limitation of all finger flexion and forearm pain Solution Release adhesions of the shortened tendon |
|
|
Flexor tendon repair complications.
|
1. Flexor Tendon Rupture (5%) 1 or 2 stage repair
2. Adhesions (20%). Therapy 3–6mths. 3. PIPJ contractures. Splints then operative 4. Triggering 5. Pulley failure 6. Quadrigia |
|
|
Flexor tendon zones. |
1 – distal to FDS (FDP only) 2 – between A1 pulley and FDS insertion (2 tendons in sheath) 3 – palm, lumbrical origin
4 – in carpal tunnel 5 – proximal to carpal tunnel |
|
|
Flexor tendon repair. Concepts.
|
1. Core suture
Strength of repair proportional to Number of strands crossing the gap (not suture type) Suture size (usually non absorbable braided suture 3/0 or 4/0) 2. Repair strength increases more rapidly with early motion stress 3. Dorsal sutures are stronger but may interfere with blood supply 4. Repairs usually rupture at knots 5. Locking loops decrease pull out and increase strength 7. Peripheral Circumferential Suture – increases repair strength by 10–50% – reduces gapping and bulk of repair – closure of epitenon with 6/0 suture |
|
|
Early ROM for tendon repairs
|
At 3 wks load to failure is 3 x strength compared with immobilised tendon.
Early ROM decreases adhesions. |
|
|
Early Active ROM Protocol
|
Splint in Wrist, MCPJ flex and PIP and DIP Ext.
Stage 1. P flexion 5 x hour. Active Ext in splint. Splint never removed. Stage 2. Once full ROM gained. 5 x above plus 5 x A flex and Ext. Splint never removed. 6 wks. splint removed active wrist ext. no resistance. 8 wks. resistant work started. 12 wks normal activity. |
|
|
FDS and FDP
|
|
|

|
Epidermal inclusion cyst.
distal phalanx. Male, 3rd decade. Traumatic implantation of keratinising epithelium that continues to grow. In bone or soft tissue. Painless and firm. Mx, excision of lump curettage and BG if boney. |
|
|
Ganglion.
|
Synovial herniation.
lined epithelium, Viscous mucin, hyaluronic acid. |
|

|
Glomus tumour
Hypertrophied glomus. Coiled structure involved in temp regulation. 50% time under nail. Triad. Pain, exquisite tenderness, cold intolerance. Rx – Remove nail excise tumour, repair bed, replace nail. |
|
|
Nora's lesion.
Bizarre parosteal osteochondromatous proliferation (BPOP). Benign lesion. 50% recurrence after excision. |
|
|
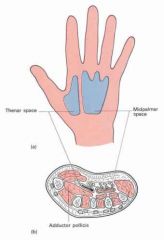
Thenar Space |
Dorsal to the flexor tendons. Volar to the interosseous fascia. Seperate from the midpalmer space by the midpalmar septum. |
|
|
Midpalmar space |
Dorsal to the flexor tendons.Volar to the interosseous fascia. Seperate from the thenar space by the midpalmar septum |
|
|
Deep palmar spaces |
|
|
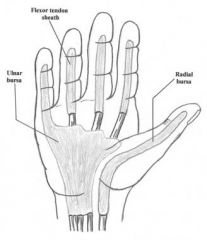
Radial bursa |
Begins at MCPJ extends 2cm prox to transverse carpal lig. Communicates with FPL sheath. |
|
|
Ulna bursa |
Begins at proximal aspect little finger sheath extends 2 cm proximal to TCL. Communicates with Synovial sheet of little finger. |
|
|
Radial and Ulna Bursa |
|
|
Parona space |
Potential space between FDP tendons adn the pronator quadratus fascia. When present the space facilitates communication between radial and ulna bursa. |
|
|
Extensor tendon |
Trifurcates at base p1. central portion insertion into base p2 (central slip). Lateral slips joined by contributions from interossei and lumbricals and form conjoined lateral band. |
|
|
Sagittal bands |
from MCPJ volar plate and the base of P1. Stabilise the Ext tendon at MCPJ. |
|
|
Transverse retinacular lig |
Level of PIPJ. Fibres are dorsal volar. stabilise the lateral conjoined bands to prevent dorsal subluxation. |
|
|
Triangular ligaments |
Stabilise the conjoined lateral bands over base P2 (almost DIPJ) to stop them volar subluxing. |
|
|
Lumbricals |
From FDP pass volar to deep transverse intermetacarpal lig on Radial side of each lig. Insert into lateral band of extensor hood. Action is to Extend PIP and DIPJ through oblique fibres. It is only muscle that can relax its antagonist. |
|
|
Action of interossei |
Flex MCPJ. Dorsal, 4, bipennate, 2 insertions (deep into tendon flex MCP, superifical into lateral tubercle abduct) Volar, 3, unipennate, from same digit MC into hoodflex MCPJ and adduct. |
|
|
Rh Wrist |
Treat wrist at same time as finger as will reoccur. Synovitis, DRUJ stretch, Volar sublux and supernation of carpus. Caput ulna. ECU sublux volar to axis which loses its mechanical advantage so radial wrist extinsors cause, radial deviation and ulna drift. Carpal collapse loss of mechanical advantage of long F/E = intrinsic overpower and intrinsic plus deformity. |
|
|
Rh wrist surgery. |
Synovectomy - does prevent tendon rupture. ECRL to ECU prevents ulna subluxation. CTD Tendon transfers. DRUJ - Darrachs / Suave Kapandji. Partial / total wrist fusion. |
|
|
Rh Tendon Ext ruptures |
Ext. starts as EDM goes radial. EDM - Vaughan-Jackson Syndrome. LF = RF side to side LF/RF = MF side to side. LF / RF / MF = LF / RF to EI + s2s MF - IF. All = RF and MF FDS. |
|
|
Rh Tendon Flex ruptures |
Go from radial to ulna. Mannerfelt. Rupture FPL over scap and trapezium. May wish to fure to prevent further rupture. May need to debride bone prom. FPL rupture fuse IP or t/f FDS IF. IF FDP = fuse DIP IF FDS and FDP = fuse DIP t/s FDS MF. |
|
|
Rh MCPJ |
Ulna drift. capsule stretch, CL stretch, Ulna volar Flex tendons die to pulley stretch. Ulna dislocation extensor tendons. Radial deviation wrist. Rx Synovectomy ST release - Divide transverse, obl, sag bands ulna side. Release ulna side interossi and t/f to next digit thru radial lateral band. realign ext tendon by ulna sag band release. If joint detroyed then add swansons arthroplasty to the above. |
|
|
Management of Swan neck |
Aim for FFD of PIPJ. Use slips of FDS, detach prox pass thru a2 pulley and attach to bone or itself. Producing 20deg FFD. +DIP fusion. May need to release intrinsics if tight. Arthroplasty or arthrodesis. |
|
|
Management of Boutonnieres |
early - reduce lateral bands and suture them together. late - Matev central slip reconstruction. Arthrodesis. |
|
|
Rh Thumb |
Boutonniere commonest. MCJP flex, IP hyper ext. Usually EPB rupture with EPL sublux. Flexable. Synovectomy MCPJ, EI to EPB and EPL centralisation. or EPL t/f and fuse IPJ. Fixed any joint fuse (even both). |
|
|
Eaton Classification 1st CMC OA |
1- synovitis 2- Jt narrow < 1/3 sublux 3 - Jt obliterated sublux BOT proximal anchored by adductor pollics, base radially. 4 - Multiple joints. |
|
|
Beak lig |
Volar, palmar oblique lig. Volar tubercle trapezium Ulna base MC Resis dorsal subluxation |
|
|
DRUJ instability |
Dorsal dislocation locked in pronation. CR and hold in supination. Volar dislocation locked in supination CR into pronation and hold. |
|
|
Keinbocks |
Vascular V mechanical theory. 1 - No radoilogy 2 - Sclerosis 3 - collapse / fragmentation 3a- normal carpal height 3b - LOH / capitate migrates. 4 - Pan carpal arthritis. Poor grip strength. TTP lunate. |
|
|
Keinbocks Rx |
1 - splint 3mths. (doesnt work) 2 - neg ulna variance = radial shortening. 2 - pos ulna variance = Capitate shortening or vascularised bone graft. 3a as above 3b limit fusion STT or 4 corner 4 PRC, arthrodesis. |
|
|
ECU calcific tendonitis |
Sudden onset pain with out trauma. Hx ulna deviation. Selling and crepitation. |
|
|
ECU subluxation |
6th compartment. has its own fibro-osseous tunnel distal 15mm ulna. The extensor ret passes over this. Forced supination, palmar flex and ulna dev. Common in tennis. Acute immoblise in long arm plasterin pronation. Chronic reconstruction using Extensor ret. |
|
|
Webspace anatomy |
From web skin 40mm proximal to just past MCPJ. Superficial transverse lig is superifical and passes over the flexor sheaths onto phalanges. Deep transverse MCL joins palmar surfaces of MCPJ. Contains; Digital N and V. Lumbrical tendons. Interossei is dorsal to deep palmar lig. |
|
|
Mid palmar space |
roof = fascia deep to long flexor tendon. floor = interossei and metacarpals. proximally = limited by parietal attachment of long flexor sheaths to walls and dorsum of carpal tunnel. distally – continuous with lubrical canals – ie easy communication with web space |
|
|
Thenar Space |
lies under tendon sheaths of FPL and IF long flexor sheath. roof = adductor pollicis communicates distally around distal border of add pol in web space of thumb, with the space btw add pol and 1st DI. |
|
|
Dupuytrens |
AD with variable penetration. Alcohol, DM, Epilepsy, Smoking, Chronic lung disease. M7:f1 Caucasians 50-70. 3 stages, Proliferative, Involutional, Residual. Type 3 collagen, myofibroblast, intercellular fibronectin. |
|
|
Dupuytrens bands |
Pre tendinous Spiral Natatory LAteral digital sheet Graysons lig. |
|
|
Dupuytrens Cords |
Pretendinous (MCPJ) Central (PIPJ) Spiral (NVB connects to p2) Lateral (close to skin DIPJ) Natatory (web space) Retrovascular (dorsal to NVB, DIP ext) Abduct DM 1st web space. |
|
|
Dupuytrens Diathesis |
Aggrressive early onset, multiple areas, usually FHx, Recurs rapidly. Feet (ledderhose) Penis (Peronie) Garrods pads (PIPJ) |
|
|
Lucks three stages |
1st - proliferative, incr cellularity, large number myofibroblasts. 2nd - involutional, dense myofibroblast network align to long axis of collagen bundles. 3rd residual, myofibroblasts disappear, fibrocytes and dense collagen remain. |
|
|
PIPJ contracture |
Central, spiral, lateral, retrovascular. Resect cords, capsulotomy, release check rein lig, Accessory collateral lig, volar plate. |
|
|
Superficial Palmar arch |

Ulna Artery. Runs volar to Long finger flexers. |
|
|
Deep palmar arch |
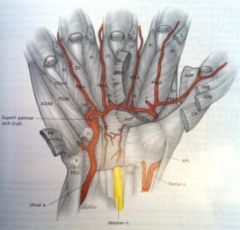
From deep branch ulna artery. Runs deep to flexor tendons on Palmar interossi. ? supplies dorsal surface of finger. |
|
|
Radial artery |

? runs on dorsal interossi |
|
|
Superifical nerves from Ulna |
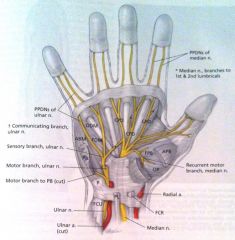
Runs volar to flexor tendons with superifical art. |
|
|
Vessels and arteries in hand / fingers. which is volar. |

Vessels run volar in palm and dorsal in finger |
|
|
Zones of guyons canal |
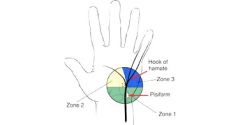
Zone 1 S&M (# ganglion) Zone 2 M (# ganglion) Zone 3 S (thrombosis) |
|
|
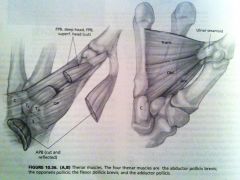
Muscles of thumb |
|
|
|
Order of innervation for the PIN |
ECU, EDC, EDM, APL, EPL, EPB, EIP. |