Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
37 Cards in this Set
- Front
- Back
|
Homeostasis
|
-Intracellular and extracellular fluids
-pH -Nutrients and waste -Electrolytes -Fluid volumes and pressures |
|
|
Negative Feedback
|
-Controlled by receptors, hormones, nervous system, enzymes
-The body is telling system to stop once it reaches a normal level |
|
|
Positive Feedback
|
-Tells system to keeping doing what it is doing
|
|
|
Cell Injury
|
Can be d/t:
-Infection -Hypoxia -Chemicals -Trauma -Genetics -AI: auto immune -Nutrition |
|
|
Atrophy
|
-There is a ⇓ in cellular size.
-Most commonly affects skeletal muscle, the heart, secondary sex organs, and the brain. ex. -Physiological: Normal process Aging (alzheimer's) -Pathological: abnl. Osteoporosis, muscle atrophy d/t immobilization |
|
|
Osteoporosis
|
-Osteopenia: weakening of the bone
-There is a ⇓ in bone mass Causes: -Estrogen deficiency -Post menopausal -Calcium deficiency -⇑ cortisol -Renal, Multiple Myeloma, or Vitamin D deficiency S/S: -Kyphosis, compression fx, radiolucency Testing: -Bone density scan (DEXA) T-score < -2.5 (-1 to -2.5 osteopenia) |
|
|
Alzheimer's
|
-Progressive destruction of the brain
Causes: -Genetics- can be detected early -FHX, Age, Down’s syndrome S/S: -Amyloid plaques (infl.)- like scabs on the nerves; neuritic plaques + cell death, Cortical Atrophy -Accumulation of tau protein neurofibrillary tangles + dystrophy -Decr. acetylcholine -Problems w/ memory, judgment, behavior, reasoning Testing: -R/O other possible causes |
|
|
Intracellular Accumulation
|
Pathological
-Lipids – Liver disease -Iron – Hemochromatosis -Copper – Wilson’s disease ciser flisure) -Uric Acid – Gout -Beta-Amyloids- Alzheimer's -Bilirubin- Liver, GB, Pancreas -Melanin - Addison’s -Dystrophic Calcification – Atherosclerosis -Malignant Calcification – Hyperparathyroism, Malignancy |
|
|
Hemochromatosis
|
-Increased iron absorption (30% - Normal 10%) and storage
Causes: -Primary – Genetic -Autosomal recessive – Disease -Secondary – other disorders, alcoholism S/S: Fatigue, Arthritis Deposits in liver (cirrhosis), pancreas (DM), heart (HF), anterior pituitary and other organs -Gray or bronze skin tone Testing: -Serum Fe -ferritin- storage form of Fe -transferrin saturation (>45%), TIBC- Total iron binding capacity -Glucose -FSH/LH -reproductive hormone, -EKG -Imaging -DNA testing Management: -Therapeutic Phlebotomy -Vitamin C: need to limit Vit C intake because it binds with Fe |
|
|
Hypertrophy
|
-There is an increase in size of cells and the affected organ.
ex. -Physiological: hypertrophy during pregnancy -Pathologically: BPH, CHF, left ventricular hypertrophy, HTN |
|
|
Hyperplasia
|
-Increase in the number of cells d/t ⇑ rate of cell division
-Physiological: -Compensatory hyperplasia (1) *kidney or liver (ectomy) or failure *callous -Hormonal hyperplasia (2) *pregnancy -Pathological: -can occur as a response to excessive hormonal stimulation ex. endometrial hyperplasia, BPH, fatty liver (NASH) |
|
|
Dysplasia
|
-There are abnl. changes w/in mature cells to include size, shape, and organization.
-Referred to as atypical hyperplasia -There is only pathological dysplasia -usually occurs in epithelial tissue and associated with neoplastic growths r/t Cancer -can be reversible if caught and corrected early -commonly seen in cervix and resp. tract |
|
|
Metaplasia
|
-Reversible replacement of one mature cell by another less differentiated cell.
-Always pathological -Ex. smoker lungs. the cells that are replaced do not secrete mucous or have cilia. Replaced d/t damage from smoke inhalation -If smoking stopped cells can be corrected if not risk for dsyplasia (cancer cells) - Squamous to glandular epithelium - Barrett’s esophagus can turn into a cancer |
|
|
Cell Adaptation
|

|
|
|
Coagulative Necrosis
|

-occurs in kidney, heart, and adrenal glands as a result of hypoxia
-The necrotic tissue appears firm and slightly swollen |
|
|
Liquefactive Necrosis
|

-results from ischemic injury (Cerebral ischemia) or Bacterial infection
The tissue becomes soft, liquefies, forms cyst |
|
|
Caseous Necrosis
|

- Commonly results from TB lung infection and Histoplasmosis
-It's a combination of coagulative and liquefactive necrosis -Tissues resemble cottage cheese. -(lipids+macrophages) -Develop granulomas |
|
|
Fat Necrosis
|

-High Fat content
-Can occur in breast, pancreas, and other abd structures. Necrotic tissue appears opaque and chalky white |
|
|
Gangrenous Necrosis
|

-Death of tissue r/t severe hypoxic injury
-Dry (Ischemic) usually d/t coagulative necrosis (skin dry and shrinks) -Wet (Bacterial) looks cold, swollen, and black. There is a foul odor and pus |
|
|
Cells Involved with Inflammation
|
-Neutrophils- First responders and initiate the inflammatory process
-Eosinophils- Involved with allergic rxns and parasites Basophils- Releases histamine Macrophages- Do the cleaning up and usually appear towards the end of the inflammation process. -Lymphocytes- B cell antibodies --Immunoglobulins -IGM-(The initial or primary response) starts early in neonatal life -IGD- Not alot of info on it, unknown fx. -IGG- Long term immunity -IGA- found in mucosal membranes -IGE- works against allergic rxns and parasite infections T cells -Tell immune system to turn on and off. -Platelets- Coagulation |
|
|
Genetics
|
- DNA- Housed in the nucleus and is the "body cook book"
- Chromosomes- Packages of DNA (23 pairs) -Males XY -Females XX Traits -Physical – ex. Hair, eye and skin color -Behavioral – ex. Herding dog -Familiar predispositions – Sickle cell, CVD, CA, Mental illness |
|
|
Genetics
|
-Dominant: the disease was given to child by one parent. The person who passed it on usually has that disease also
-Recessive: both the parents passed on the disease but do not have the disease. Just carriers -Sex-linked: effects the X and Y -Autosomal: out side of sexlinked -Multifactorial: ex. pre disposition of DM. Environmental and Lifestyle related |
|
|
Chromosomal
|
Disease related to Abnl. Chromosomes
|
|
|
Down's Syndrome
|
-Trisomy 21 with physical and mental disorders
Causes: -Chromosomal disorder -Maternal age --35 – 1/385 --40 – 1/106 --45 – 1/30 S/S: -Small head with flat facial features -Slanted eyes, Single crease in palm of hand -Heart defects, leukemia, dementia, decr. IS -May have decreased IQ and speech difficulties -Risk for Early Alzheimer’s Testing: -Prenatal care – US or amniocentesis |
|
|
Down's Syndrome
|

|
|
|
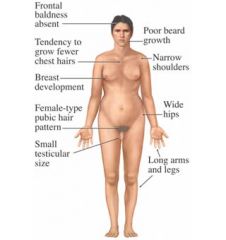
Klinefelter's Syndome
|
Causes:
Chromosomal disorder XXY 1/500 -1000 S/S: -Generally male with both male and female sexual characteristics - ⇓ testosterone less body and facial hair, gynecomastia (risk breast CA), weak muscles and bones (osteoporosis), shy -Infertility Testing: -Clinical Exam -Chromosomal testing -Hormones |
|
|
Klinefelter's Syndrome
|
|
|
|
Turner's Syndrome
|
Causes:
- Chromosomal disorder w/ women - contain X only also called XO S/S: - Short stature - No or irregular menstrual periods; ovarian failure, risk for ovarian Ca. - No breast development - Infertility - Aortic stenosis or coarctation; pulses stronger on upper extremities compared to lower - Web neck - Nipples are wider apart Testing: - Clinical - Chromosomal testing - Echo - Reproductive Hormones |
|
|
Turner Syndrome
|

|
|
|
Dominant
|
Disease given by ONE parent and usually has the disease also
|
|
|
Hunington's Chorea
|
-Progressive degeneration of nerve cells
Causes: -Genetic- Autosomal dominant -FHX -Middle age onset S/S: -Chorea ⇒ jerky movements -Problems ⇒ Speech, Balance, Swallowing Cognitive Impairment, Behavioral/Personality Changes Testing: -CT/MRI -Genetic testing |
|
|
Dwarfism
|
Adult height of less than 4 feet 10 inches or less”
Causes: - ⇓ GH - Achondroplasia (autosomal dominant) ⇒ Most Common ⇒ no cartilageproduction ⇒ no bone production - problem is below the hips; shorter than nl. and leads to hip problems Primordial dwarfism ⇒ autosomal recessive S/S: - Hip deformities - Clubfoot - Scoliosis and lordosis Testing: - Clinical exam ⇒ height percentiles - Hormones - X-Ray/CT - Genetic testing |
|
|
Recessive
|
Both parents passed the disease but do not have the disease (Carriers)
|
|
|
Cystic Fibrosis
|
Causes:
Autosomal recessive ⇒ ⇓ Cl metabolism ⇒ ⇑ Na and H2O reabsorption ⇒ sticky mucus S/S: - Respiratory- cough, wheezing, freq. infection (Pseudomonas), clubbing, bronchiectasis - GI –meconium ileus, abnormal fat metabolism⇒ steatorrhea, fecal impaction, fat absorption is not absorbed well which causes decrease in vitamin absorption, brain tissue, cholestrol (Makes our steroid hormones) - Pancreas – decr. exocrine function ⇒ digestive enzymes -Liver – thick bile -Growth- failure to thrive -Reproductive – infertile males and some females Testing: - Sweat test ⇒ NaCl - Genetic Testing |
|
|
Muscular Dystrophy
|
- Skeletal Muscle degeneration
Dystrophin deficiency (protein responsible for intracellular structure and support) - Wheelchair by age 12 - Excessive fat tissue and effects lower legs (calves) Cause: -Duchenne MD -- MC, severe, early onset (1) -- X-linked recessive – male children -- Weakness in proximal muscles – necrosis of muscle fibers – replacement with fatty tissue – pseudohypertrophy -- Pneumonia -- Decr. IQ, cardiomyopathy, incr. intestinal transit time - Becker MD -- Less severe than Duchenne’s Testing: -Incr. CK -EMG (electromyogram) -Genetic -Biopsy |
|
|
Sickle Cell Anemia
|
Causes:
- Sickle cell disease ⇒ Autosomal recessive - Sickle cell trait⇒ one defective gene ⇒ have both Hb A and S - African American - Hb S instead of Hb A ⇒ live only ~ 16 days - Hb F S/S: - Sickling of cells ⇒ Hypoxia, dehydration, acidosis, cold temps, infection abdominal and bone pain, ulcerations, thrombi, infarcts - Acute Chest Syndrome ⇒ damage to lung tissue, cardiomyopathy - Hemolytic crisis ⇒ Jaundice and hematuria - NO def. due to incr. lysed cells - Splenic sequestration crisis ⇒ HSM - Aplastic crisis - Higher risk osteomyelitis and aseptic necrosis - Retinal hemorrhage/ detachment, Priapism |
|
|
Sickle Cell Anemia
|
Testing (high, low, normal)
- Bilirubin (high) - Potassium (high) - WBC’s (high) - Hemoglobin (low) - Reticulocytes: immature blood cells (high) - Newborn screening CBC – diff., reticulocytes, Hb Electrophoresis |