Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
54 Cards in this Set
- Front
- Back
|
What is blood pressure?
How is it generated? What does it ensure? |
Measurement of force applied to artery walls.
Generated by the cardiac contraction against vascular resistance --> driving force that moves blood through vascular system. Ensures optimal delivery of metabolic substrates at the tissue level. |
|
|
Diastolic or systolic.
Heart contracts Heart at rest |
Contract = systolic
Relax = diastolic |
|
|
What organ systems does blood pressure regulation involve?
|
Central and autonomic nervous system
CV Kidney Adrenal gland |
|
|
For god's sake regurgitate the normal, pre-hypertension, etc. again.
|
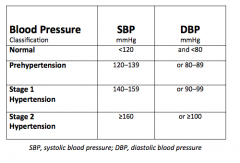
|
|
|
Two types of hypertension: which one is most common? Causes of each.
|
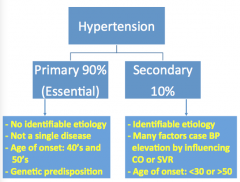
Primary: age = 40s and 50s, genetic
Secondary: age = young or old, changes in CO or SVR |
|
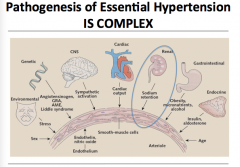
Overview of all the things that contribute to essential hypertension.
|
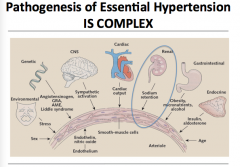
Look it over.
|
|
|
Do genetics play a role in HTN?
|
Oh yes!
70-80% have a family history |
|
|
What are some candidate genes for HTN?
What leads to intermediate phenotypes? |
M235T variant in angiotensinogen gene, angiotensin-converting enzyme gene, B2-adrenergic receptor gene
Hypertensinogenic factors (environment and behavior) |
|
|
What monogenic diseases have been identified that lead to HTN?
|
Liddle's disease = activating ENaC mutation
Glucocorticoid remediable aldosteronism: gene mutation that leads to aldosterone synthetase responsive ACTH Mineralcorticoid excess: inactivating mutations in 11B-HSD-2 gene |
|
|
What is the equation for MAP?
What can increase in BP be? Another equation for MAP? |
MAP = CO x SVR
Increase CO and/or SVR MAP = (SBP-DBP)/3 + DBP |
|
|
What is the equation for CO?
How can you increase SV? |
CO = SV * HR
Increase pre-load or cardiac contractility --> increased SV |
|
|
What can increased pre-load be due to?
Does increased CO in essential HTN persist? What is NOT a cardiac feature of essential HTN? |
Increased venous tone, increased volume--> must mean increase in total sodium (Na)
No! Peripheral edema |
|
|
What is the role of kidney in BP regulation?
|
Alter extracellular volume by altering NA and water excretion/reabsorption --> maintains healthy BP range
|
|
|
What does the development of sustained HTN depend on?
What lowers BP in the majority of patients? |
Impairment in kidney ability to excrete excess sodium and therefore water.
Decrease Na intake, increase Na excretion (diuretics) |
|
|
True or false.
Hypertension follow the kidney. |
TRUE!
Kidney from hypertensive donor given to normotensive recipient will result in hypertensive patient. |
|
|
What is Guyton's theory of long-term BP control?
What does this imply? |
Essential HTN = ability of kidney to excrete sodium load
Homeostasis from pressure natriuresis = increase pressure, renal sodium output increases, EC fluid responds appropriately Impairment in pressure-natriuresis = persistant elevated BP. |
|
|
Principal site of changes in Na excretion?
Does this affect GFR? What is a mediator? |
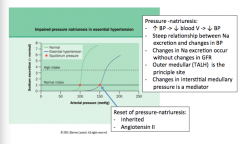
No change in GFR
Principal site = TALH Mediator = changes in interstitial medullary pressure |
|
|
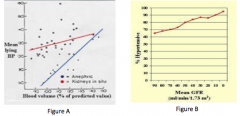
How will the renal curve change in salt-sensitive hypertension?
|
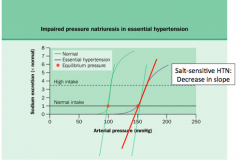
Decrease in slope?
|
|
|
What are the pros of Guyton's theory?
|
Allows for a normal blood volume despite an elevated pressure, in keeping with most volume measurements in hypertensive patients
|
|
|
Cons of Guyton's theory?
|
Ignores role of ANS in the development of HTN
Fails to explain BP↑ in prehypertension, where ↑ CO mainly driven by activation of SNS |
|
|
Draw the pathway of "long term autoregulation."
|
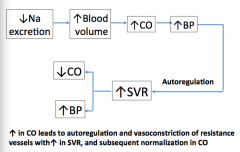
What does an increase in CO lead to?
|
|
|
What is the role of Ouabain in the transition from increased CO to increased SVR?
|
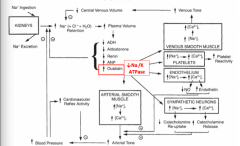
Seems to decrease Na/K ATPase which would lead to increased Na+ in endothelium --> increased calcium --> decreased NO and increased endothelin --> vasoconstriction
Secreted by adrenal gland => also leads to increased sympathetic neurons => increased calcium => increased catecholamine release = > increased arterial tone => increased BP |
|
|
What is Brenner's hyppothesis of essential HTN?
|
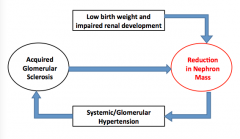
Reduction in nephron mass => makes kidneys unable to excrete normal sodium loads.
|
|
What is the role of reduced nephron mass?
|
Normal kidney = infusion of sodium --> small BP change
No kidney = infusion of sodium --> rapid BP rise Progression of chronic kidney disease (decline in GFR) --> prevalence of HTN rises |
|
|
What is the role of salt in the development of HTN?
|
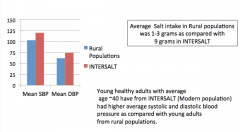
Increased salt intake seems to correspond to higher BP.
|
|
|
If there is no salt intake, even with aging, does HTN appear?
|
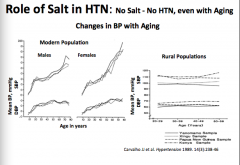
No!
|
|
|
What is the role of salt in HTN? Equation.
Not everyone is salt sensitive though. Which populations are more salt sensitive? Does salt sensitivity increase with age? |
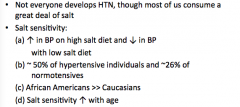
Salt --> increased BV --> CO --> HTN
|
|
|
What is the mechanism behind decreased kidney Na excretion that leads to HTN?
|
Decrease kidney Na excretion --> increase activity of SNS --> activation of kidney Na/H+ exchanger --> increase in intracellular Ca in vascular smooth muscle cells --> decrease in NO
|
|
|
What does MAP equal?
What are some factors that effect SVR? Vasoconstrictors and dilators? What are some local factors (auto regulation)? |
MAP = CO x SVR
Vasoconstrictors = ATII, NE, endothelin, ADMA Vasodilators = NO, prostacyclin, PGE2, PGD2, adenosine Local = mediated by NO |
|
|
What is the pathway behind the renin-angiotensins-aldosterone system?
|
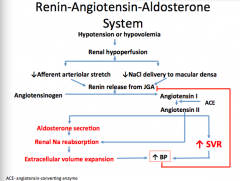
Draw this out again.
|
|
|
In the juxtraglomerular apparatus, what does the activation of each receptor do?
B1-Rc Adenosine2-Rc Prostaglandin Rc |
B1-Rc = increase renin secretion
Adenosine2-Rc = decease renin secretion Prostaglandin Rc = increase renin |
|
|
In the macula dense, what is the effect of each?
Increase NaCl delivery Decrease NaCl delivery |
Increase = increase adenosine production
Decrease = increase NO and prostaglandins |
|
|
What are extraglomerular mesangial cells?
|
"Supporting cells"
|
|
|
Is renin elevated in everyone with HTN?
|
No!
20% high PRA (plasma renin acCvity): “Dry HTN” - 30% low PRA : “Wet HTN” 50% normal PRA |
|
|
What is Laragh's hypothesis of nephron heterogenesity?
|
Some nephrons ischemic --> high PRA
Others not ischemic --> have imparied natriuresis from ATII Total PRA is diluted and may be normal |
|
|
What is the role of RAAS in renal artery stenosis (secondary hypertension)? Use the Goldblatt model I.
What could be used to reduce BP? |
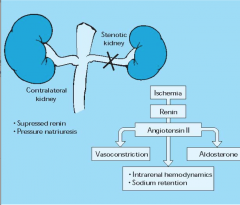
HTN associated with unilateral RAS is associated with increased SVR and right shift in pressure natriuresis in normal kidney --> excretes excess Na, volume does not play additional role in BP
ACE-inhibitors reduce BP |
|
|
What is the Goldblatt model II in the role of RAAS in BILATERAL renal artery stenosis?
Do ACE inhibitors work? |

Total kidney mass hypoperfusion
No off-setting pressure natriuresis (flash pulmonary edema) Intolerance to ACE-inhibitors |
|
|
Is RAS more common in whites or black?
What does RAS get higher with? Most common causes of RAS? |
32% whites with DBP > 125mmHg, only 4% black
increasing age, diabetics, PVD, DBP > 125mmHg Atherosclerosis (85%) Fibromuscular dysplasia |
|
|
What is the role of SNS in HTN?
|
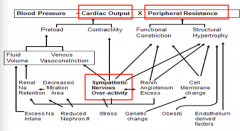
Cardiac output
Peripheral resistance SNS |
|
|
What are some causes of secondary hypertension?
|
Aldosterone excess
Glucocorticoid excess Pseudohyperaldosteronism Type 1 (Liddle and 11B-hydroxysteroid dehydrogenase inhibition) Pseudohyperalsoderonism type 2 (Gordon) |
|
|
What are all causes of secondary characterized by?
|
Salt-sensitive hypertension
All (except aldosterone excess) => low renin and low aldosterone All (except Gordon) => hypokalemia and metabolic alkalosis |
|
|
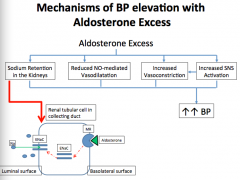
What are the mechanisms that lead to elevated BP with aldosterone excess?
|
|
|
|
what are the mechanisms that lead to volume expansion in glucocorticoid excess (Cushing's syndrome)?
|
|
|
|
What are the clinical features of pseudoHYPERaldosteronsm?
Two causes of 11B-hydroxysteroid dehyrdogenase deficiency or inhibition: |
HTN, hypokalemia, metabolic alkalosis, low renin, low aldosterone
Genetic = 11B-hydroxysteroid dehydrogenase deficiency Acquired = chronic licorice ingestion inhibits 11B-HSD2 |
|
|
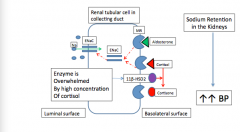
What is the pathophysiology behind 11B-hydroxysteroid dehydogenase deficiency?
What is the treatment? |
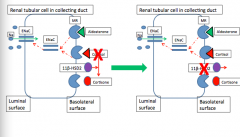
Cortisol in presence of inhibition/deficiency --> epithelial sodium channel activation in CD --> increase Na reabsorption
Treatment = stop using substance if acquired, if genetic = use triamterene or amiloride |
|
|
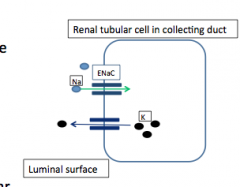
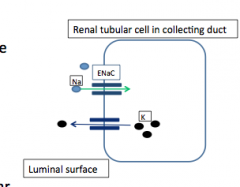
How does Liddle's syndrome cause pseudohyperaldosteronism?
What is the therapy? |
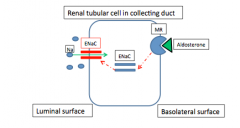
Genetic defect = autosomal dominant mutation --> constitutive activation of Na+ channel in distal tubule due to mutation in B or gamma subunits
Triamterene or amiloride |
|
|
What is the mechanism behind hypokalemia?
|
Increased Na reabsorption in CD --> increased K+ secretion by creating favorable gradient. --> intracellular shift of H+ into tubular cells --> secretion into lumen
|
|
|
What is the mechanism of metabolic alkalosis?
|
Increased H+ secretion by H-pump in response to activation of mineralcorticoid receptor
Hypokalemia --> intracellular shift of H+ into tubular cells --> secretion into lumen |
|
|
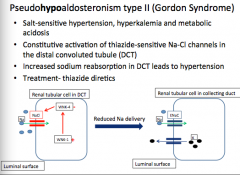
What is seen clinically with pseudoHYPOaldosteronism type II?
(Gordon syndrome) |
Salt-sensitive hypertension, hyperkalemia, and metabolic acidosis
|
|
|
What is the mechanism behind Gordon syndrome?
How do you treat it? |

Constitutive activation of thiazide-sensitive Na-Cl channels in DCT --> increased Na+ reabsorption in DCT --> hypertension
Treat = thiazide diuretics |
|
|
BP = 185/102
HR = 78 Bicarb = 19 Creat = 1 k = 5.4 Increased function of which transporter or channel may explain hypertension? |
Sounds like metabolic alkalosis
Hyperkalemia Gordon's syndrome (Pseudohypoaldosteronism type II) Na-Cl co transporter in distal tubule. |
|
|
True or false:
The ability to maintain blood pressure in normal range with sodium loads is reduced in chronic kidney disease. |
True
|
|
|
True or false:
If you eat a low sodium diet, you are less likely to develop hypertension even with aging. |
True
|
|
|
When would RAS-blockers not be effective for blood pressure reduction?
|
55 year old with low plasma renin level
Will work to LOWER BP in person with bilateral stenosis, but the patient will probably not be able to tolerate it. |