Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
61 Cards in this Set
- Front
- Back
|
1. What Fungi is superficial?
2. What Fungi are Cutaneous? 3. What Fungi is Subcutaneous? |
1. Malassezia furfur
2. Dermatophytes (Trichophyton, Microsporum, Epidermophyton) 3. Sporothrix Schenckii |
|
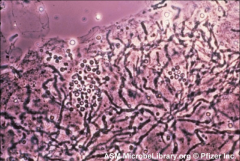
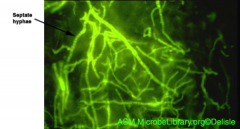
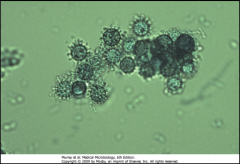
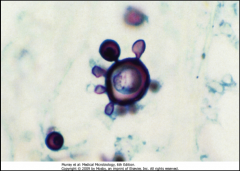
1. What is pictured here? Describe its morphology.
2. Who is vulnerable to this? 3. Where does it grow on you? 4. How is it transmitted? |
1. Malassezia furfur - Lipophilic Yeast that looks like "Spaghetti and Meatballs" (Clusters of yeast with curved, septate hyphae). A collar forms at the lips of bud initiations
2. BOTH Immunocompetent and Immunocompromised 3. Overgrowth on oily skin (Part of Normal Flora) 4. Person to Person transfer of Keratinous Material |
|
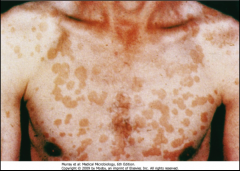
1. What disorder is pictured here and what causes it?
2. Describe the morphology of the infection. 3. Is this in yeast or hyphal form? 4. How long does this last and what are the symptoms associated with it? |
1. Pityriasis (Tinea Versicolor) caused by Malassezia furfur
2a. Fine, Dust-like scales form and interfere with Melanin Production 2b. People with dark skin --> Hypopigmented 2c. People with light skin --> Hyperpigmented 3. Both forms 4. Chronic - Asymptomatic Lesions |
|
|
1. Who is vulnerable to fungemia via Malassezia furfur?
2. How do you diagnose Malassezia Furfur? 3. How do you treat it? |
1. Infants with IV Lipid supplements b/c the fungus is Lipophilic
2a. KOH stain of skin scraping - See clusters of yearst w/ curved septate hyphae (Spaghetti and Meatballs) 2b. UV Fluorescence - Turns Coppery Orange 2c. Culture - Add olive oil b/c it is lipophilic 3. Topical Selenium Sulfide |
|
|
1. Describe the appearance of the cutaneous Dermatophyte Genera
2. What are they referred to as? 3. What is the most common symptom for Dermatophytes? |
1. Filamentous (Monomorphic) fungi
2. Ringworm - Tinea 3. Itching |
|
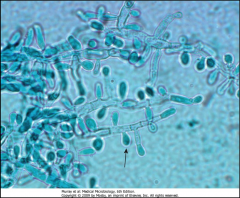
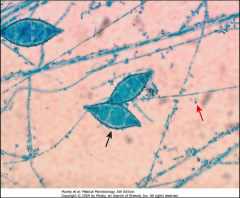
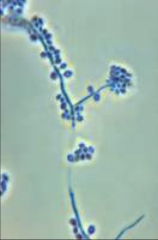
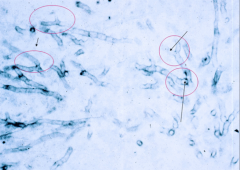
1. What is pictured here? What category of Mycosis is this?
2. Describe the morphology 3. What do macroconidia look like? |
1. Trichophyton - Cutaneous Skin Mycosis
2. Abundant Microconidia with a few macroconidia 3. Pencil-shaped with smooth walls |
|
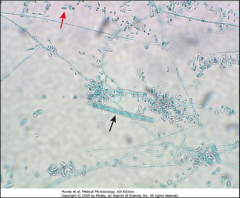
1. What is pictured here? What category of Mycosis is this?
2. Describe the morphology. Which is the micro and which is the macroconidia? |

1. Microsporum - Cutaneous skin mycosis
2. Macroconidia is large, thick walled, and multicellular. They look like shells pasta 2. Micro look small |
|

1. What is pictured here? What category of Mycosis is this?
2. Describe the morphology. |
1. Epidermophyton - Cutaneous Skin Mycosis
2a. NO Microconidia. 2b. Macroconidia are Club-shaped, thin, and have smooth walls |
|
|
What are Dermatophytes called when they are on the:
1. Scalp, brows, lashes 2. Beard 3. Smooth or Glabrous skin 4. Groin 5. Foot 6. Nails |
1. Tinea Capitis
2. Tinea Barbae 3. Tinea Corporis 4. Tinea Cruris 5. Tinea Pedis 6. Tinea Unguium |
|

1. What causes Tinea Capitis?
2. What is the scope of the infection? 3. What is the most serious form of this infection? What does it look like? 4. What is the vector for this? |
1. Microsporum and Trichophyton on the Scalp
2a. Skin and Hair Surface 2b. Hair Shaft (Ectothrix - Shaft) (Endothrix - inside Shaft) 3. Tineas Favosa - Permanent Hair loss, Inflammatory, Itchy 4. Cats and Dogs |
|

1. What causes Tinea Barbae?
2. What is the scope of the infection? 3. What happens if you shave with this? |
1. Trichophyton on the Beard
2.Mild and Superficial OR Severe, Inflammatory, Pustular (Folliculitis) 3. Could open up lesions and lead to secondary bacterial infection |
|

1. What causes Tinea Corporis?
2. What is the scope of the infection? 3. How is this spread? |
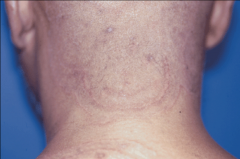
1. Any Dermatophyte on smooth skin other than the beard and scalp (can also be on the face)
2. Can be on the whole body. (See picture) 3. P2P contact |
|

1. What causes Tinea Cruris?
2. What is the scope of the infection? 3. What is the main symptom aside from appearance? 4. Why does it grow here? 5. How do you treat it? |
1. Trichophyton or Epidermophyton on the Groin, Perianal, Perineal, or Upper Thigh Area
2. Scope: Erythmatous to brown lesions covered with thin, dry scales 3. Itchy 4. It likes sweaty, moist areas 5. Powder (gold bond) |
|

1. What causes Tinea Pedis?
2. What is another name for TInea Pedis? |
1. Trichophyton or Epidermophyton on the Soles and Toe Webs
2. Athlete's Foot |
|

1. What causes Tinea Unguium?
2. How do you treat this? |
1. Trichophyton on the Nail Plate
2. Oral Antifungal |
|
|
1. How do you diagnose Dermatophites (Tinea - Ringworm)?
2. How do you treat them? |
1a. KOH stain on the skin/nail scrapings for Hyphae and Arthroconidia
1b. Calcifluor White Test 1c. Wood Lamp - Microsporum Glows Fluorescent Green 2a. Topical Imidazoles (all EXCEPT Unguium) 2b. Oral Imidazoled (Unguium - Nail) 2c. Keep Areas Dry |
|
1. What is pictured here?
|
1. Microsporum under a Wood Lamp
|
|
1. What is pictured above? What category of mycosis is this?
2. What is special about this compared to the other skin mycoses? 3. Which form is pictured above? 4. Describe the Morphology. 5. What does the Tissue form look like? |
1. Sporothrix Schenckii - Subcutaneous Mycosis
2. This is the ONLY Dimorphic one 3. Mold Form 4. Hyphae with Rosettes, sleeves of conidia with Conidiospores at a 90 DEGREE ANGLE from septate hyphae - Usually solitary 5. Cigar-shaped yeast |
|

1. What is this and where can you get this from?
2. Who is most at risk for this? 3. What is the pathogenesis? 4. What is it called if this gets into the blood? |

1. Sporothrix Schenckii - Cutaneous Inoculi where a Rose Thorn stabs you (also Tree Bark, Shrubs, plants)
2. Rose Gardeners 3a. Inoculation with Sporothrix Schenckii 3b. Conversion of Mold to Yeast 3c. 1-10 Week Incubation 3d. Open lesion at the Injury Site and a Chain of Nodular, ulcerating lesions up the lymphatic tract (Pictured) 4. Extracutaneous |
|
|
1. Who is at risk for the inhaled form of Sporothrix Schenckii?
2. How is Sporothrix Schenckii (all types) diagnosed? 3. How is it treated? |
1. Alcoholics - Pulmonary Spororichosis
2. Diagnosis - Culture Pus or Tissue Tissue Biopsy - Shows Yeasts (easy to do) Serology 3. Treatment Lymphocutaneous - Itraconazole Pulmonary - Amphotericin B |
|
|
1. Which form of Mycoses are ALL dimorphic?
2. What is meant by Primary Pathogens? 3. What is meant by Endemic Pathogens? 4. What is the difference in infections b/w the two immune statuses? |
1. Systemic
2. It can infect BOTH immune statuses AND it is INHALED FIRST and THEN MOVES TO THE DEEP VISCERA 3. Located in specific geographical areas --> The spores are inhaled from THAT SPECIFIC ENVIRONMENT 4. Immunocompromised people get MUCH MORE SEVERE infection |
|
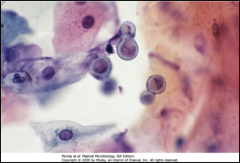
1. What mycosis is pictured and in what form?
2. Describe the morphology. 3. Where is it found geographically? 4. What is the source of it? 5. Who is at risk for contracting this? |
1. Blastomyces Dermatitidis - yeast form
2. BROAD BASED BUDS 3. Ohio-Upper Great Lakes, Africa, Europe, Middle East 4. Dogs and ROTTING WOOD 5. People new to the area and never exposed before |
|
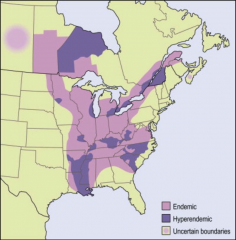
1. What mycosis is found in this geography?
2. What is the pathogenesis of this mycosis? 3. What do people new to the area get? What do people who live in the area get? What to immunocompromised people get? 4. Describe the progression of symptoms in Immunocompromised people. |

1. Blastomyces Dermatitidis
2a. Inhalation of conidia 2b. Transform at 37C into yeast 2c. Neutrophilic and Granulomatous Reaction 2d. IF IMMUNOCOMPROMISED: Disseminated via Macrophages to Skin, Bone, Urinary Tract 3a. New to Area - Pulmonary - Flu-like symptoms, Chronic IF LARGE INOCULATION (ARDS, Pneumonia, diffuse infiltrates, SOB, Tachypnea, Hypoxemia) 3b. Locals - Asymptomatic 3c. Immunocompromised - Disseminated (Skin involvement w/o pulmonary or systemic) and CNS problems 4a. Face, neck, extremities - Starts as a DEMARCATED PAPULE 4b. Forms ULCERATED LESIONS w/ PUSTULES 4c. Chronic |
|
|
1. How is Blastomyces Dermatitidis diagnosed?
2. How is it treated? |

1a. Morphology - Broad Based Buds
1b. Smear or culture of affected area 1c. Culture 2. Treatment - Amphotericin B |
|
|
What are the 4 Systemic Mycoses and what are their buzzwords?
|
1. Blastomyces Dermatitidis - Broad Based Buds (BBB) and Rotting Wood, Granuloma
2. Histoplasma Capsulatum - Pigeons, Excavation/Demolition, Calcification like TB 3. Coccidiodes Immitis - Arizona, Dry, Desert, Desert Mumps 4. Paracoccidiodes Brasiliensis - Pilot's Wheel, Brazil |
|
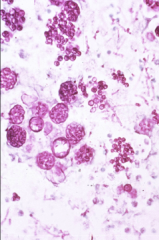
1. What is pictured here?
2. Describe the morphology of this form. 3. What does the other mold form of this look like? |

1. Macroconidia of Hystoplasma Capsulatum
2. Round and fuzzy 3. Microconidia on short stalks |
|
|
1. Where, geographically, can we find Histoplasma Capsulatum?
2. Where can you find Histoplasma Capsulatum normally? 3. How is it transmitted and what is the pathogenesis? |
1. Central USA - Eastern Great Lakes and Mississippi and Missouri River Beds, Mexico, and South America
2. Pigeon Poop (Nitrogen Rich Soil) and Excavation/Demolition Sites (b/c there is pigeon poop in the cracks) 3a. Inhalation of microconidia (from pigeon poop) 3b. Phagocytosis by Macrophages and Neutrophils 3c. Germination inside the phagocytes - FACULTATIVE INTRACELLULAR) 3d. Remain localized or Spread in Blood and Lymph |
|
1. What mycosis is this and how can we tell?
2. How much of this do you have to inhale to get any symptoms? 3. What 2 antigens does this carry? |
1. Histoplasma Capsulatum - It is OBLIGATE INTRACELLULAR, so it is growing inside of a phagocyte in this picture
2. A LOT - with a low inoculum , 90% are asymptomatic 3. M and H antigens |
|

1. What is this and what causes it?
2. What does this organism cause in immunocompetent people? 3. What does it cause in immunocompromised people? |
1. Disseminated Histoplasmosis in Immunocompromised - Histoplasma Capsulatum
2. Acute Pulmonary Histoplasmosis - Flu-like symptoms, Mediastinal Node Enlargement, Hepatosplenomegaly and RDS IF IT DOESN'T RESOLVE ITSELF 3. Lesions that calcify and look like TB on CXR AND IF DISSEMINATED --> Musculocutaneous lesions (Pictured) |
|
|
1. What are the complications of Histoplasma Capsulatum?
2. How is it diagnosed? 3. How is it treated? |
1a. Lymphadenopathy with Bronchial Obstruction
1b. Arthritis/Arthralgias 1c. Pericarditis 1d. Mediastinal Fibrosis 1e. Calcification of pulmonary lesions 2. Microscopy, Culture for Temp-Regulated Dimorphism, Serology, Antigen-Detection for antibodies to M and H antigens 3. Amphotericin B |
|
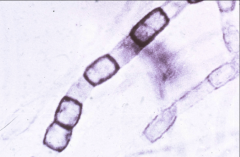
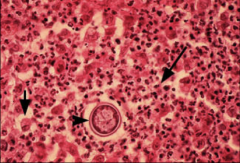
1. What form of Coccidiodes Immitis is pictured?
2. What is the other form and what does it look like? 3. Where and when can this be found? |
1. Mold Form - Arthroconidia
2. Yeast Form - Endosporulating Spherules 3. Arizona, Dry, Desert area, California, New Mexico in the Late Summer/Early Fall |
|
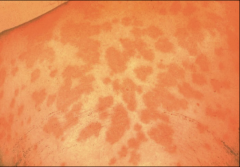
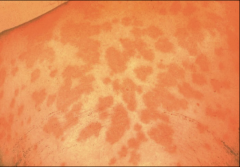
1. What is pictured here and what causes it?
2. What causes this symptom? 3. Who is at risk for this? 4. How is it transmitted and what is the pathogenesis? |
1. Erythema Nodosum (Blotchy Rash) - Coccidiodes Immitis
2. Allergic Reaction from Immune complex formation 3. Outdoor occupations, Infants and Elderly, Late Pregnancy/Early Post-partum, HIV 4a. Vegetative HYPHAE convert to ARTHROCONIDIA 4b. Inhalation and conversion to SPHERULES 4c. Progressive Internal Septation --> MATURE SPHERULES RUPTURE 4d. ENDOSPORES are released and can convert to SPHERULES in the body |
|
|
1. What does Coccidiodes Immitis cause?
2. What are the symptoms of Primary Disease? 3. What are the symptoms of Secondary Disease? 4. When in pregnancy is Coccidiodes Immitis dangerous? |
1. Valley Fever (DESERT MUMPS)
2. Asymptomatic, Self-limiting Flu-like illness, Allergic Reaction (ERYTHEMA NODOSUM 3a. Progressive Pulmonary Disease - Nodules, Cavitary with Calcifying lesions as they heal 3b. Dissemination to skin. bones, joints, soft tissues, meninges - IMMUNOCOMPROMISED and 3rd Trimester of pregnancy 4. 3rd Trimester |
|
|
1. How is Coccidiodes Immitis Diagnosed?
2. How is it treated? |
1. Dagnosis:
Microscopic Exam of Sputum, Exudates, or Tissue for SPORULES (Pictured) Nucleic Acid Hybridization Culture - Requires Infection Control 2. Amphotericin B |
|
1. What is this? Describe the morphology
2. Where, geographically, is this found? 3. Who is at risk for contracting this? 4. Describe the transmission and pathogenesis |
1. Paracoccidiodes Brasiliensis - PILOT'S WHEEL - Round with single or multiple buds
2. Brazil - Latin America 3. Children, Immunocompromised, Those exposed to soil 4a. Inhalation or Traumatic Inoculation 4b. Self-limiting Primary Infection in the Lungs 4c. Gets to other organs via Venous System or Lymphatics |
|

1. What does this picture have to do with Paracoccidiodes Brasiliensis?
2. What are the Clinical implications for adults? 3. What are the clinical implications for Immunocompromised people? |
1. In children, they can get Lymphadenopathy, Bone Marrow Involvement, and Osteoarticular Manifestations --> Dislocations, Improper Bone Growth
2. Adults - Respiratory and possible reactivation of primary respiratory infection years later 3. Immunocompromised - Disseminated to Mucous Membranes, Skin, and Lymph Nodes |
|

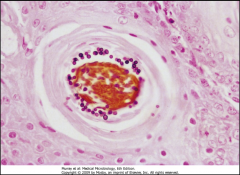
1. What is pictured here? What causes it?
2. How is this diagnosed? |

1. Mucous Membrane/Skin Lesions - Paracoccidiodes Braziliensis
2a.. Microscopy for the Pilot's Wheel yeast morphology 2b. Culture - Demonstrating temp-regulated dimorphism |
|
|
1. What are the 4 Opportunistic Mycoses and what are their buzzwords?
|
1. Cryptococcus Neoformans - Encapsulated Yeast, Pigeon Breeders, AIDS
2. Aspergillus Fumigatus - 45 degree angle mold, AIDS 3. Candida Albicans - Germ Tubes at 37C, Phenotypic Switching 4. Oneumocystis Jiroveci - P. Carini - Silver Staining Cysts, Foamy Honeycomb Appearance, Ground Glass on X-Ray |
|
|
What two Mycoses have to do with Pigeons and what is the difference in buzzwords?
|
1. Cryptococcus Neoformans is an Opportunistic, encapsulated yeast that Pigeon Breeders and AIDS patients get
2. Histoplasma Capsulatum is a systemic mycisis that is found where there is pigeon poop such as High Nitrogen soil and excavation/demolition sites. It is the most common pulmonary mycosis in Humans |
|
|
What is the most common pulmonary mycosis in humans?
|
Histoplasma Capsulatum
|
|
|
What is the only yeast that has a capsule?
|
Cryptococcus Neoformans
|
|
|
1. What is the morphology of Cryptococcus neoformans?
2. Who is at risk for it? 3. Where is it found? |
1. Encapsulated yeast (Extracellular Polysaccharide Capsule) with budding replication
2. Pigeon Breeders and Immunocompromised (AIDS) 3. Worldwide in soil with High Nitrogen Content |
|
|
1. Describe the Clinical Outcomes of Cryptococcus Neoformans
2. What does the disease progression depend upon the most? |
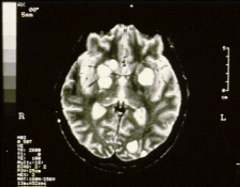
1. Acute pulmonary disease
2. Cutaneous Cryptococcus Neoformans 3. Life-threatening Encephalitis or meningoencephalitis (Pictured) 4. Fever, HA, visual disturbances, chills, mental disturbances 5. Increased Intracranial pressure 2. Dependent on --> IMMUNE STATUS |
|
|
How is Cryptococcus Neoformans Diagnosed?
|

1. India Ink stain of CSF --> Reveals Capsule (Pictured)
2. Urease + yeast 3. Latex Agglutination for Polysaccharide Capsule Antigen 4. MRI for white colonies of fungal growth in brain |
|
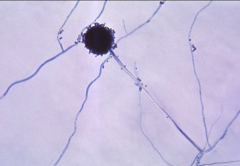
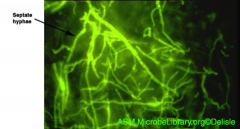
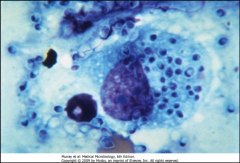
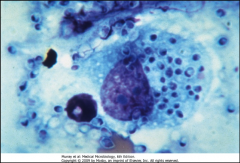
1. What is pictured here? How can you tell?
2. Who is at risk for this? 3. Where is it found, geographically? 4 How is it transmitted and how does it spread? 5. Why does this not spread in healthy people? |
1. Aspergillius Fumigatus - Branched, septate hyphae at 45 degree angles
2. Immunocompromised (AIDS) 3. Found worldwide in soil, water, and decaying matter. ALSO NOSOCOMIAL 4. Inhaled and spread via Blood (hematogenous) 5. Healthy people have normal neutrophils and macrophages, which prevent hematogenous spread |
|
|
Which two opportunistic mycoses are Nosocomial?
|
1. Aspergillius Fumigaus
2. Candida Albicans |
|
|
1. What stops Aspergillius Fumigatus from colonizing the respiratory tract?
2. What happens to the people who get this form of infection? 3. What symptomology does Aspergillius Fumigatus usually cause? |
Cystic Fibrosis creates mucous plugs that Aspergillius Fumigatus gets stuck in.
2. Causes an Allergic Reaction --> Bronchopulmonary spasm and Sinusitis 3. Fungal ball of hyphae and mucous plugs the lower respiratory tract and forms lung cavities --> Hemorrhage |
|
|
1. What is necessary for treatment of Obstructive bronchial Aspergillius Fumigatus?
2. What does the invasive/disseminated form look like and who gets this form? |
1. Surgery to remove the balls of Aspergillius hyphae and mucous.
2. Immunocompromised (AIDS) patients - Pneumonia, Meningitis, and Cellulitis in Burn Patients |
|
|
How is Aspergillius Fumicatus diagnosed and treated?
Why won't a culture for it work in diagnostics? |
1. Diagnosis - Skin Biopsy and Stain
2. Treatment - Amphotericin B 3. Too common in the lab. Won't know if you grew your sample or if it was contaminated |
|
|
1. Describe the morphology of Candida Albicans?
2. What does it produce when invading?\ 3. What is characteristic of its morphology? |
1. Oval-like yeast with buds, blastoconidia and chlamydospores
2. Produces Pseudo-hyphae and true hyphae 3. Forms germ tubes at 37C and has PHENOTYPIC SWITCHING ability - A single strain can change morphologies reversibly |
|
|
How is Candida Albicans Transmitted?
What is the primary source of infection? Where can it NOT grow? |
1. Nosocomial - Into the bloodstream
2. Patient is the primary source of the infection 3. Cannot grow in the stomach |
|
|
What are the features of Oropharyngeal Candidiasis from Candida Albicans?
|
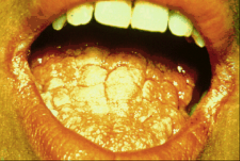
1. Burning and Dryness of the mouth, Loss of taste, Painful swallowing
2. ORAL THRUSH - white plaques like milk curd on buccal mucosa in Infants, Elderly, and AIDS |
|
|
1. What are the features of Hematogenous Candidiasis?
2. What are the clinical symptoms possible from Candida Albicans? 3. What do healthy people get when they get Candida Albicans? 4. How is it diagnosed? |

1. Acute or Chronic Septicemia
2. Growth on: Vulvovaginal, Skin, GI, Lungs, Urinary Tract, Meninges, Endo/Myo/Pericardium, Buccal Mucosa 3. Rash in skin folds such as fat fold and arm pits, 4a. Microscopy and Histology (KOH, PAS, GMS) 4b. Culture |
|
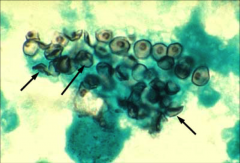
1. What is pictured here?
2. What is the other name for this? 3. What are the 3 manifestations of this? |
1. Silver Staining Cysts of Pneumocystis Jiroveci
2. P. Carini 3a. Ubiquitous -- Acquired young, found in lungs, and P2P spread 3b. Pneumocystosis - AIDS patients, but declining due to HAART therapy - Interstitial Pneumocystis, Mononuclear Infiltrate, Cyanisis, NON-PRODUCTIVE COUGH 3c. Extrapulmonary manifestations |
|
|
1. What does the pathology of Pneumozystis Jiroveci look like when the patient has Pneumocystosis?
2. What does a patients T-Cell count have to be for this? 3. How is it diagnosed? 4. How is it treated? |
1a. Foamy Honeycomb appearance
1b. Looks like GROUND GLASS on X-Ray 2. <50cells/microL 3a. Silver Stain for Cysts 3b. Lavage to grap respiratory tract cells since the cough is non-productive 4. Cannot treat it with no immune system to work with |
|
|
1. What is the morphology of a prion?
2. Why can we get mad cow disease even when we cook the meat thoroughly? 3. What is the other name for Mad Cow Disease? 4. What is the disease called when you get it from injection, contact with contaminated medical devices, or Inherit it? |
1. Abnormally folded protein into Beta-Pleated-Sheets
2. Heat does not destroy prions 3. Bovine Spongiform Encephalopathy 4. Creuzfeldt Jakob Disease (CJD) |
|
|
What are the 3 Inheritable Prion Diseases?
|
1. Creutzfeldt Jakob Disease
2. Fatal Familial Insomnia (FFI) 3. Gerstmann-Straussler-Scheinker (GSS) |
|
|
What is Kuru and who gets it?
Where is this located? What is characteristic of Prion diseases? |
Prion disease obtained from the Kuru Tribe cannibalizing their enemies
New Guinea NO INFLAMMATION |
|
|
What is PrPc and what does it do?
Where is PrPc found? What is the mechanism of prion diseases? |
1. PrPc is a normal protein - Maintains neuronal integrity of the brain and responds to Oxidative Stress
2. PrPc is found in the brain and in the peripheral nerves and ganglia 3a. PrPscrapie touches PrPc 3b. PrPc's alpha helices fold into Beta-sheets 3c. The infection spreads and forms Amyloid Fibrils, which kill neurons |
|
|
1 and 2. What is the diagnostic characteristic of Spongiform Encephalopathy?
3. What are the clinical characteristics of the pathogenesis of Prion diseases? |
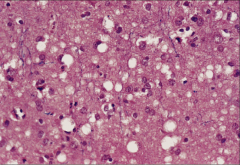
1. Small vacuoles within the Neuropil from neuronal loss followed by glial cell proliferation to fill in the gaps
2. No Inflammatory response 3a. Progressive neurodegeneration 3b. Unknown Incubation period 3c. Loss of muscle control and Tremors 3d. Shivering, Myoclonic Jerks 3e. Loss of coordination 3f. Rapidly progressing dementia --> Mistaken for Alzheimers |
|
|
How are prion diseases diagnosed?
What is it often mistaken for? What is the treatment for them? |
Autopsy or based on clinical grounds
It is often mistaken for alzheimer's There is no treatment |