![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
58 Cards in this Set
- Front
- Back
|
Acute renal failure - pre-renal, renal, post renal |
Pre-Renal: - Shock - acute tubular necrosis, cortical necrosis - Volume loss (Polyuria, diarrhoea, burns etc) - Reduced cardiac output (heart failure etc) - Systemic vasoconstriction (sepsis, anaphylx) - Excessive constriction of afferent arteriole (NSAID, contrast, NA, hypercalcaemia)
Renal Injury: - Glomerular - Severe GN (anti-GBM or vasculitis) - Tubular toxic acute tubular necrosis (gent'in) myoglobinuria crystal deposition e.g oxalate, urate tubuloinerstitial nephritis acute pyelonephritis - Vascular thrombo / atheroemboli arteritis accelerated hypertension, HUS
Post-Renal: - Urinary tract obstruction e.g. tumours of bladder , prostate tumour - Stones or crystals - strictures, catheters blocked, increased inra-abdominal pressure |
|
|
Common causes of clinical syndromes of renal disease CHRONIC RENAL FAILURE CAUSES (must know these) |
Glomerula: Chronic glomerulonephritis Diabetic Nephropathy Acute glomerulonephritis - (e.g. vasculitic GN) Whole Kidney: Polycystic kidney disease Hypertension - direct damage to kidneys or BP alone Chronic Pyelonephritis |
|
|
Common causes of clinical syndromes of renal disease PROTEINURIA / NEPHROTIC SYNDROME (must know these) |
Targeting the Podocyte: Minimal change disease Primary Focal segmental glomerulosclerosis Membranous Nephropathy
Others: Other GNs - lupus, IgAN, MCGN (mesangiocapillary glomerulonephritis) etc Diabetes Amyloidosis Myeloma Kidney |
|
|
Common causes of clinical syndromes of renal disease HAEMATURIA (must know these) |
Lower UTI - stones, infection tumour Glomerulonephritis - IgA nephropathy Inherited abnormalities - thin membrane nephropathy |
|
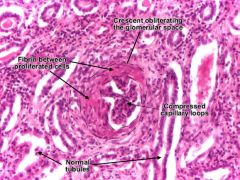
ACUTE RENAL FAILURE Glomerular lesions |
Rapidly progressive glomerulonephritis =severe destructive glomerulonephritis presents histologically as crescentic glomerulonephritis Differential: Vasculitic glomerulonephritis Anti-GBM - goodpastures severe immune complex glomerulonephritis (lupus nephritis, IgA nephropathy) |
|
|
Acute kidney injury - Presentation
|
Oliguria (urine output less < 400 mL/day) or Anuria: Presence of haematuria, proteinuria, leukocytes: - Large, painless bladder on abdominal palpation: Purpura, petechial rash, bleeding: Pericardial rub on auscultation: |
|

Anti-GBM disease
|
Antibodies to type IV collagen - goodpasture Ag Linear membrane staining for IgG on IHC Goodpasture's disease = - PULMONARY HAEMORRHAGE & ACUTE RENAL FAILURE due to anti-GBM - Lung Sx pre-date Kidney (usually) (Haemoptysis, chest pain, Cough, SOB) - Kidney Sx - haematuria, proteinuria, peripheral oedema (or face), uraemia, Hypertension. |
|
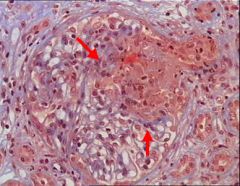
Vasculitic glomerulonephritis
|
Abs to ANCA (PR3 / MPO) = degranulation and fibrinoid necrosis - focal segmental necrosis (grenades) - arterial involvement in 20% - NO IMMUNE DEPOSITS IN GLOMERULI (pauci-immune) - crescentic proliferation |
|
Acute tubular necrosis |
MOST COMMON cause of tubular lesions - NSAIDS - commonest - Gentamicin - Heavy metals Ischaemic damage due to prolonged loss of BP. Haemorrhage, cardiogenic shock |
|
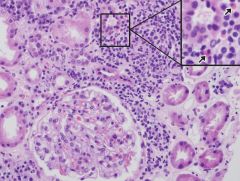
Tubulointerstitial nephritis
|
Proton pump inhibitors account for 50% - Immune response to tubular epithelium Ags - Interstitial inflammation - LYMPHOCYTIC infiltrate - Drug-induced - Abx, PPIs, NSAIDS |
|
|
Chronic Renal Failure
|
Severe, prolonged or recurrant injury e.g. vasculitis, severe HTN, Tubulointerstitial nephritis May be Insidious chronic injury e.g. Diabetes, HTN, chronic GN, polycystic kidney, chronic pyelonephritis |
|
|
Glomerular injury - 4 types of origin - immune-mediated, genetic, non-immune deposits, vascular |
Immune-mediated Glomerulonephritis: - Complement mediated - ANCA vasculitis Genetic: - Basement membrane disorders - Lysosomal storage disorders Non-immune deposits: - Hyperlipidaemia - Amyloidosis - Deposition of light chains (myeloma) Vascular: - Diabetes mellitus thrombosis - Fibrinoid necrosis in HUS - accelerated Hypertension |
|
|
Glomerulonephritis All cause renal fibrosis and risk of chronic renal failure if prolonged fibrosis (=scarring) |
Minimal Change disease or membranous nephritis = podocyte injury, no proliferation = PROTEINURIA
IgA nephropathy Lupus nephritis = Inflammation and/or mesangial proliferation = HAEMATURIA / NEPHRITIC
Anti-GBM disease Vasculitis = necrosis, crescents (blown apart) = Acute renal failure |
|
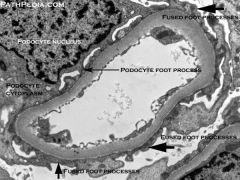
Minimal change disease
|
Acute onset of nephrotic syndrome Commonest in children (can occur any age) STEROID RESPONSIVE - Normal by light microscopy and IHC - EM - podocyte foot effacement |
|
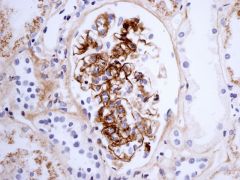
Membranous nephropathy
|
Ideopathyic (80%) - autoimmune to podocyte antigen (75% PLA2R) Secondary (20%) - Drugs - SLE - Malignancy (Ca lung or colon) - Infections (HBV EBV, syphilis)
Nephrotic Syndrome
Sub-epithelial deposits of IgG and C3 Reactive new membrane formed between deposits - membranes spike on silver stain - Podocyte produces NEW BM - Dense deposits of Ag-Ab-Complement |
|
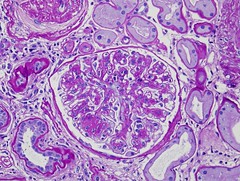
Diabetic Nephropathy
|
Type of diabetic microangiopathy - THICK LEAKY BASEMENT MEMBRANES (T1DM w/ good glucose control prevents) (T2DM irrelevant control, inevitably develops) - Nodular glomerulosclerosis (Kimmelstiel-Wlison Lesions) Exudative Lesions (Fibrin caps) Arteriolar hylinosis (arteriole hyaline - sclerosis (nodular balls of collagen)
Presents: Microalbuminuria -> Overt Proteinuria -> Chronic renal Failure |
|
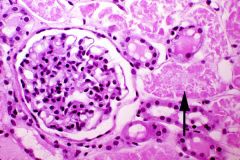
IgA Nephropathy
|
Commonest Glomerulonephritis - IgG predominant deposits (accompanied by IgG auto-Abs to IgA!) Presentation: - Variable - asymptomatic haematuria - proteinuria - acute or chronic failure Histology varies.... - Mesangial hypercellularity - Segmental sclerosis
20-30% ESRF 20 yrs post diagnosis |
|
Lupus Nephropathy
|
Major cause of SLE morbidity and mortality - Immune complexs, IgG, IgM, IgA, C3, C1q in mesangium +/- capillary wall - variable clinical presentation - variable histology - any glomerulonephritis |
|
|
NephROTIC v.s. NephRITIC syndrome |
Nephrotic Syndrome: - Protienuria - Reduced blood protein = oedema - May be increased fat in blood (inflammation of podocytes, increases permeability - loss of protein/oncotic pressure = RAAS, Na+ retention)
Nephritic Syndrome: - Haematuria - Oligouria / Anuria - Hypertension (Inflammation of epithelial barrier = blood in urine, decrease in kidney blood flow = reduced urine output, RAAS = HTN) |
|
|
Effects of kidney failure
|
INCREASED: Salt - HTN Water - Oedema, SOB Potassium - Arrhythmia Phosphate - Itching, contributes to bone disease Waste (Urea/acid) - Sickness, anorexia, encephalopathy, SOB
DECREASED: Vit D - Bone disease EPO - Anaemia Salt - Dehydration Water - Thirst |
|
|
Degree of renal failure
|
Mild >30% function, no symptoms Moderate 15-30% HTN, anaemia, lack Vit D Severe - 5-15% progressively unwell, loss of appetite, nausea, tired, breathless End-Stage <5% v. ill, death unless treat |
|
|
Signs of renal disease
|
- Proteinuria - Haematuria - Hypertension - Altered urine output - oligouric/polyuric - Uraemia (kidney failure) (commonly DM) MULTISYSTEM: SLE hereditary renal disease - PKD, Alport's syndrome (kidney ear eye - collagen defect) |
|
|
NephROTIC syndrome - Leaky Glomeruli - Various histology |
Triad of: 1. Proteinuria - >3.5g/day 2. Hypo-albumin-aemia - <25g/dL 3. Oedema Associated: - Hyperlipidaemia (CHOLESTEROL HIGH) - Hypercoaguable (RISK VTE) *anticoagulate |
|
|
Mechanisms of Proteinuria
|
Glomerular - increased permeability - albumin Overflow - increased plasma conc exceeding re-uptake capacity of tubules (e.g. bence-jones - DIPSTIX NEGATIVE) Tubular - Impaired reabsorption of normal filtrate - b2 microglobulin Secreted - Tamm-Horsfall protein (part of renal matrix, decreased in urine when stones forming) |
|
|
Tubulo-interstitial Nephritis |
- Loss of concentrating power - Inability to secrete molecules - Inability to reabsorb = thirst (dehydration) polyuria, nocturia (ADH doesn't work) - Autoimmunity or allergic response to drugs (PPI, Abx, Anti-inflammatory) or infection - ACIDOSIS and GLYCOSURIA Pathologically: PPI-induced interstitial nephritis EBV / CMV / toxoplasma infection Sarcoid Sjorgen's |
|
|
NephRITIC syndrome - Inflamed glomeruli - Glomerulonephritis - loss of glomerular function |
Presents with: - Haematuria - Reduced filtration = oliguria, uraemia, fluid retention (mild), HTN Pathology: - Post-strep glomerulonephritis (following sepsis) - IgA nephropathy (most common) - SLE - Microscopic polyangitis - Granulomatosis with polyangitis (Wegner's) - Anti-GBM |
|
|
Causes of Haematuria - Macroscopic (Coca Cola urine) - Microscopic (4% of cases this is benign) - Associated features allow localising |
RENAL CAUSES: = Renal failure! - Loss of renal function - HTN - Proteinuria - Any Age - No Evidence of Obstruction - Occupation (solvents) UROLOGICAL CAUSES: MALIGNANCY = pain free, renal function preserved (unless both obstructed), Older age, occurs late, aniline dyes exposure, drug exposure STONES = May be obstructed, Dehydration, Family Hx, PAIN, agonising renal colic |
|
|
Acute Kidney Injury - Medical emergency |
Biochemical presentation: - Hyperkalaemia - Metabolic acidosis - Waste product accumulation - High levels of renally excreted drugs |
|
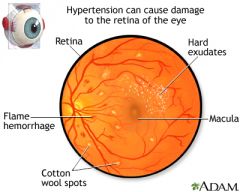
Long standing Hypertension - end organ damage
|
Brain - Strokes, lacunar infarcts Eyes - Hypertensive retinopathy Heart - Left ventricular hypertrophy, ECG/ECHO! Kidneys - Haematuria and proteinuria -Urinalysis EPO increases in AKI, not chronic kidney disease |
|
|
Calcium, bone and phosphate Distinctions for acute and chronic kidney disease |
Urea and creatinine - High in both Potassium - High in both (academia) pH - Low (academia) for both Calcium - Low in chronic, not enough time to breakdown bone - precipitates in tissues - acute retention = normal acutely Phosphate - High in chronic - PTH breaks down bone, phosphate precipitates calcium PTH - High in chronic Alk Phos - High in Chronic (bone turnover) Bone Radiology - Loss in chronic Hb - Low in chronic (loss of EPO) Renal Size reduced in chronic (except PKD) |
|
|
Diagnosing Renal disease
|
Immunology: Immunoglobulins - monoclonal bands/myeloma Bence Jones Protein - myeloma Electrophoresis - free light chains/myeloma ANA/DNA binding - SLE Anti-GBM - goodpastures ANCA - wegners/GPA Cryoglobulins - precipitate on cold Anti-streptolysin O antigen (ASOT) |
|
|
Commonest tumours of kidney
|
Adults - renal cell carcinoma Children - Wilm's Tumour (nephroblastoma) |
|
|
Benign tumours of Kidney
|
- Usually small (<5mm) - No clinical significance - papillary adenoma HOWEVER: Angio-myo-lipoma, Onco-cytoma >5mm, clinically significant, mimics malignant tumour on imaging Oncocytoma = mahogany brown, central scar, nests of benign cells, round nuclei and eosinophilic cytoplasm Angiomyolipoma = blood vessels, smooth muscle and fat - yellow fat - reddish vessels FAT visible on radiology |
|
|
RENAL CELL CARCINOMA (RCC) |
RCC - 85% of adult malignant renal tumours - 65% are >65 years M>F Smoking doubles the risk, VHL increases risk, end stage renal disease increases risk clear cell often chrom 3 abnormalities (VHL 3p)
- CLEAR CELL is the commonest - Epithelial cells of renal tubules, can be benign to v. agrressive, Often single mets - often lung - Local Growth = renal capsule - Vascular = renal vein and IVC lymphatic = Para-aortic LN
PRESENTATION: - May present with systemic symptoms, mets often to lungs and bones TRIAD: 1.Haematuria 2.Loin pain 3.Mass (10% cases) Commonest = haematuria Paraneoplastic: -Polycythemia -Fever
SURVIVAL: Age, Size (<7cm=>90% 5yrs, >7cm=<50% 5yrs) Stage (10-30% 5 Yr survival w/ mets), grade worse = collecting duct > clear cell > papillary
TREATMENT: - Surgical - Nephrectomy +/- adrenal - Partial nephrectomy and laproscopic (nephron sparing) - Tyrosine kinase inhibitor SUTITINIB (resistance develops) - High freq USS experimental treatment |
|
|
Wilm's tumour - nephroblastoma
|
Children <5 years, rarely older (rare but commonest blastoma) Presentation = Abdominal mass Spread = direct, lymphatic, venous Prognosis = >90% w/ aggressive chemo/radio Appearance: - large rounded mass, undifferentiated cells - Blastoma recapitulates developing foetal cells (tubules, glomeruli, stroma, deletion 11p) |
|
|
Transitional cell carcinoma - UROTHELIAL CARCINOMA 2nd most common kidney cancer |
Similar to transitional carcinoma of bladder - urothelium (transitional epithelium) renal pelvis - Difficulat to diagnose - hard to Bx, radiological - Fills renal pelvis |
|
|
RENAL STONES!
|
Commonly intra-renal - renal calyces or renal pelvis Urinary bladder CALCIUM (oxalate +/- phosphate) = 70% TRIPPLE stones (magnesium, ammonium, phosphate) = 15% Uric acid = 5-10% Causes: - Hypercalcaemia - Dehydration - Nidus of infection - Obstruction - urinary stasis / infection EFFECTS/PRESENTATION: - PAIN!! urinary colic - Haematuria (damage) - Obstruction HYDRONEPHROSIS - Chronic infection PYELONEPHRITIS (STONES, STASIS, INFECTION contribute to one another) |
|
|
Hydronephrosis
|
Dilation of ureater (hydroureter) Dilation renal pelvis+collecting (hydronephrosis) CHRONIC OBSTRUCTION Causes: - PUJ obstruction - Ureteric reflux (bladder valve abnormality) - Tumours of lower tract - Stones - Prostatic enlargement / ureter compression SECONDARY EFFECTS: - Loss of renal parenchyma = chronic renal fail - Urinary stasis=stones, infection, pyonephritis (frank pus), pyelonephritis (inflammation of renal parenchyma) |
|
|
Pyelonephritis
|
= Inflammation usually BACTERIAL affecting tubules, interstitium and pelvis (glomerulonephritis= intrinsic of glomeruli) ASCENDING - usually from UTI - may be haematogenous spread
CAUSES: - PREDISPOSED TO UTI (diabetes, immunosuppressed, female) - anatomical abnormality of tract congenital ureteric or bladder abnormality chronic obstruction due to stones/fibrosis |
|
|
Renal cysts
|
Simple = common, rarely symptomatic, thin walled cortical epithelial cyst filled with urine - PKD - Adult - Dominant APKD1 - chrom 16 haematuria, hypertension, renal failure, bilateral massive kidneys. Cysts in other organs - liver and pancreas (ALSO Berry aneurysm - 30%) 5-10% of all end stage renal disease - PKD - Children - recessive cysts and fibrosis in liver as well |
|
|
Causes of UTI
|
Uncomplicated - E.coli in 80% (rest-proteus, enterobacteriaceace, strep, chlamydia, adenovirus, ureaplasma, fungi) Complicated - E.coli in 50% (Klebsiella, Enterobacteriaceae, Pseudomonas) |
|
|
Risk factors for UTIs
|
HOST DEFENCES: - Urine - osmolality, urea, organic acids, low pH, uromucoid = altered host defences - Tamm-Horsfall Protein - mannose binding - Mechanical - flushing, ureteric peristalsis, VUJ - Prostatic fluid HOST FACTORS: - Age (increases with age) - Gender (females at greater risk) - Preganacy - 1-3%, dilated ureters, poor peristalsis, lower bladder tone, ureteric obstruction - Obstruction - prostate, tumour - Mechanical - sex, catheter, spermicides - Genetic - blood group, immune response - Neurological disease (MS, DM, Neuropathy) - Reflux - Stones |
|
|
Uncomplicated UTI - Sx - Organisms |
Sx: - Dysuria, urgency, frequency (50% of women have no bacteruria) Culture negative- 30% = Chlamydia, candida 30% = low grade bacteruria 20% recurrant (post menopause, coital practice, genetic) |
|
|
Complicated UTI |
Acute pyelonephritis: = Fever, loin pain, Rigors, Dysuria, Renal tender, 15-30% BACTERAEMIC = BLOOD CULTURES Pregancy: - Affect the outcomes of pregnancy - asymptomatic bacteriuria in 5% - 20-40% risk of pyelonephritis UTIs in Men - uncommon younger than 50 years UTIs Children: - Non-specific Sx - Associated with reflux in 50% of children <5 |
|
|
Complications of UTI
|
CHRONIC Pyelonephritis Chronic interstitial nephritis - scarring from recurrent infection Papillary Necrosis - especially DM, sickle, obstruction, analgesic nephropathy Abscesses: uncommon - risk factor = DM / stones - intrarenal / perinephritic BACTERAEMIA - 30% mortality - common cause of community bacteraemia (gram -ve sepsis worsens the outcome) |
|
|
Catheterisation - related UTI
|
Colonisation - asymptomatic catheter-associated bactinuria should not be treated - Risk about 5% per day - 20% of catheterised patients develop bacteriuria, 6% develop symptoms of UTI - Treat + remove catheter, + Gentamicin IM/IV |
|
|
Diagnosis of UTI
|
Urinalysis: Leucocyte esterase: - sterile pyuria: Treated UTI, fastidious organism, TB, foreign body, tumour Nitrites: - A bacterial metabolite - Low sensitivity / high specificity - FALSE NEG = Vit C, S.G. Leukocytes + Nitrates both negative = 92% NPV
Urine culture: - Pregnant women (first antenatal screen), after Rx screen monthly, treat on symptoms - Elderly people with significant signs - Recurrent cystitis - Treatment failure CULTURE IF SIGNS OF UTI AND....: - immuncompromise (DM, drugs, HIV) - indwelling catheter - abnormal GI tract |
|
|
Treatment of UTI
|
Hydration - IV fluids if vomiting Acidify urine (potassium citrate in cystitis) Analgesia Frequent voiding (forcefully) Avoidance of risk factors Antibiotics: NITROFURANTOIN - 1st line (also trimethoprim, cephalexin) Co-Amox or Ceftriaxone - 2nd line Uncomplicated - 3 days as good as 7 Complicated - imaging, 10-14 days, +/- IV Abx, PREGNANCY: - avoid Tetracycline, Ciprofloxacin |
|
|
Differential for a UTI
|
Urethral syndrome - no signif bacteriuria Interstitial cystitis Atrophic vaginitis / urethritis (lack of oestrogen) Urethritis, vaginitis, cervicitis = chlamydia, gonorrhoea, herpes, other sexually transmitted Drug-induced cystitis - allopurinol, NSAIDs Pinworms / threadworms |
|
|
Transitional epithelium - urothelium
|
- Renal pelvis to the urethra - tough, protective layer from osmosis and pH METAPLASIA - squamous metaplasia in repeated trauma, infection or inflammation (common but tumour as a result uncommon) Carinoma of urinary tract common in bladder >90% urothelial cancer 8% squamous cell carcinoma 1-2% adenocarcinoma Age: 50-80 (rare<40) M>F 3:1 |
|
|
Renal cell carcinoma Transitional cell carcinoma * PRESENTS - Painless Haematuria * |
Carinoma of urinary tract common in bladder>90% urothelial cancer 8% squamous cell carcinoma 1-2% adenocarcinoma Age:50-80 (rare<40) M>F 3:1 RISKS: - Aniline dye worker (rubber, plastic, benzidine) - SMOKING (arylamines) biggest risk - @ 20yrs - analgesic abuse (phenacentin - paracetamol) - Cyclophosphamide (immunosuppressive) - Chronic infection (schistosomiasis = squamous cell carcinoma) - Congenital defects (treated = increased risk) |
|
|
Renal cell Carcinoma - Presentation, Dx
|
Presentation: - HAEMATURIA (20% with gross haematuria, 10% with microhaem have bladder Cancer) - Dysuria - LUTS (lower urinary tract symptoms) - Pelvic pain (advanced disease) Diagnosis: - Urine cytology - picks up high grade, low grade doesn't shed as easily - Cystoscopy + Bx - Imaging - Uss, CT
UROTHELIAL CARCINOMA STAGING -non-muscle invasive v.s. muscle invasive - can be in situ - papillary - exophytic into lumen - Invasice through lamina propria or beyond muscle wall -Grade 1-3 (WHO 2004 high/low/PNLMP) - Low grade don't invade/progress but recur - High grade often progress, invade - risk mets
PROGNOSIS: well differentiated, non invasive = benign poorly differentiated, solid, muscle invasion - poor prognosis |
|
|
SQUAMOUS CARCINOMA - of the bladder
|
- Tend to be poor prognosis (far worse than urothelial) - Often from metaplastic squamous epithelium (Diverticula, stones SCHISTOSOMAL infection) |
|
|
Bladded adenocarcinoma
|
Uncommon: Primary or CONSIDER SECONDARY - prostate or rectum Risk: - Urachal remnants (embryological), glandular metaplasia, bladder extrophy |
|
|
Prostate - Benign Hyperplasia
|
INNER ZONE: Glandular, muscular and fiberous - Affects 75% men 70-80 years - Complex hormonal dependance - Outflow obstruction - LUTS - LUTS: - Trouble starting (hesitancy) - Decreased Flow - Trouble stopping (terminal dribbling) - Instability (nocturia, frequency) - COMPLICATIONS: - Trabeculation - Diverticula - Acute retention - Infection (due to stasis + ^ volume) - Bladder and kidney stones - Hydroureter +/- Hydronephrosis - Renal impairment |
|
|
Prostate cancer OUTER ZONE |
1:9 lifetime risk, commonest UK male cancer Most die with not from, 1/3 men >75yrs 1% cases in men <50yrs (BRCA2) RISK: -AGE! - Heredity - BRCA2, commoner in afro-carribean - ?hormones - castration protective - ?diet - calcium + high animal fat bad; selenium and vit E protective - IGF01, incidence lower in diabetes PRESENTATION: - often asymptomatic - PSA/DRE when large = LUTS, haematuria when advanced = Bone pain DIAGNOSIS: - DRE - PSA - Transrectal USS - Needle Bx - TURP - transuretheral resection of prostate - MRI GLEASON'S Grade= 5 patterns, architecture and degree of differentiation. Higher=worse |
|

Prostatic Intraepithelial Neoplasia (similar to DCIS / CIN) |
- Precursor lesion = DYSPLASIA - Cell and nuclear pleomorphism - loss of ordered maturation - Mitotic activity -HASN'T INVADED BEYOND BASAL CELL LAYER GLEASON'S Grade= 5 patterns, architecture and degree of differentiation. Higher=worse
TNM stage |
|
|
Treatment for Prostate carcinoma
|
Localised - T1/T2 - remains in prostate Local advanced - T3/T4 - beyond capsule Metastatic - lymphatic spread to LNs Distant Mets - Lytic lesions of bone TREATMENT; - age/stage dependant - Active surveillance (repeated Bx) - Watchful waiting - Surgery (radical prostectomy) - Irradiation (external/brachytherapy) - Hormonal manipulation, androgen blockade - Crytherapy |