![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
144 Cards in this Set
- Front
- Back

|
Cervical Pillar Positioning |
|

|
Chamberlain's Line - On lateral cervical, line is drawn from posterior hard palate to posterior foramen magnum - Tip of odontoid should be no more than 3mm above line - Indicates basilar invagination due to bone softening disorders (paget’s, osteomalacia), rheumatoid arthritis, or congenital anomalies |
|

|
McGregor's Line - Line from posterior hard palate to most inferior surface of occiput - Tip of odontoid should not project above line more than 8 mm in males and 10 mm in females - Same significance as Chamberlain’s, but is more reliable because it is easier to find the reference points |
|
|
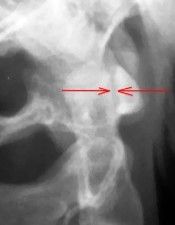
Atlantodental Interspace (ADI) - On lateral view, distance between back of anterior tubercle and front of dens - Measure at mid-portion of joint since it may be wider at the top when the spine is inflexion - Maximum= 3mm in Adults, 5mm in children - An increased distance due to loss of integrity of transverse ligament as a result of trauma, rheumatoid arthritis, dysplasias, or pharyngeal infections |
|

|
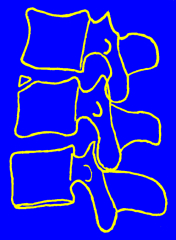
George's Line - Line drawn along posterior aspect of all vertebral bodies (in any spinal region) - Should be smooth and continuous - Can be used on flexion/extension views to evaluate for instability - A break in the line may indicate a listhesis (a slippage of more than 2 mm is significant) - Causes for an abnormal line may include trauma, DJD, normal variant in kids, or may be a positional distortion (false positive) |
|

|
Posterior Cervical Line - On the lateral view, line is drawn connecting the spinolaminar lines from C1 to T1 - Should be smooth and continuous - Should be drawn in conjunction with George’s line & holds same significance |
|

|
Sagittal Canal Diameter - On lateral view, shortest distance from the posterior vertebral body (or posterior dens) to spinolaminar line is measured - Generally, the canal diameter should be no less than 80% of vertebral body width at that level - Decreased measurement = central canal stenosis - Increased measurement = tumor or anomaly |
|

|
Cervical Gravity Line - On lateral view, line is extended down from apex of dens - Should intersect C7 vertebral body - Failure to pass through C7 indicates abnormal head carriage (perhaps due to muscle imbalance or spasm) |
|

|
Cervical Lordosis - On lateral view, line is drawn intersecting the C1 anterior and posterior tubercles - Second line is drawn along inferior endplate of C7 - Perpendiculars are erected and the superior or inferior angle is measured - 35-45 degrees is normal - Measurements outside this range MAY indicate hypolordosis or hyperlordosis |
|

(Normal) |
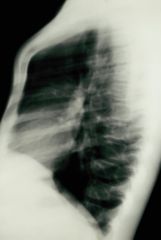
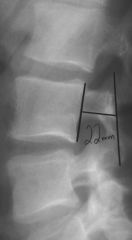
Retropharyngeal & Retrotracheal Spaces - On lateral view, measure between anteroinferior corner of C2 to posterior border of pharyngeal air shadow and between anteroinferior margin of C6 to posterior border of tracheal air shadow - Maximum measurements: 7 mm for retropharyngeal & 20 mm for retrotracheal - If increased, it indicates a space-occupying mass such as a hematoma, tumor, abscess, or goiter |
|

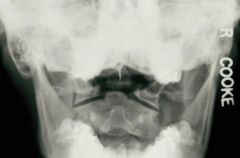
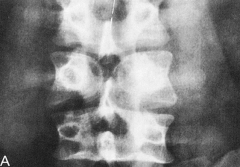
Occipitalisation of the Atlas |
Radiographic findings may include: - Incorporation of part or all of C1 into the base of the occiput - Lack of movement between occiput and C1 on flexion/extension lateral cervical radiographs - Fusion of the atlanto-occipital joints - Difficulty in seeing the atlanto-occipital region on the AP open mouth view due to a relative basilar impression |
|

Agenesis/Hypoplasia/Hypogenesis (Atlas - Posterior Arch) |
- Can happen anywhere in the spine - C1 and mid to lower cervical spine posterior arch structures most common - Complete or partial; stable or unstable - Signs of altered stress: sclerotic pedicles or anterior arch hypertrophy |
|

Odontoid Hypoplasia & Agenesis |
- Development anomaly - Complete or partial failure to form - Agenesis is rare - Associated with upper cervical instability in the absence of clinical symptoms - Characterised by reduced height of the odontoid process |
|
Os Odontoideum |
- Development anomaly - Failure of the odontoid process to unite with the body of C2 after 12 years of age - Transverse ligament of C1 is usually intact |
|

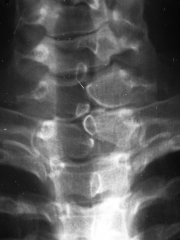
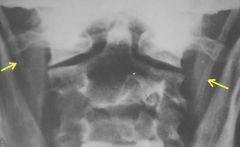
Cervical Rib (Transitional vertebra) |
- Finding needs to be differentiated from transverse process hyperplasia (no joint space) - 66% of cases are bilateral - Symptoms tend to develop in older individuals due to drooping shoulders |
|
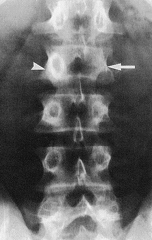
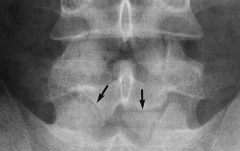
Spina Bifida |
- A vertebra which has two spinous processes as a result of two lamina failing to fuse - Clinically insignificant finding - Ratio of incidence is M:F 9:1 - Most frequent level is S1, also seen commonly at L5, C1, T12-L1 & C7-T1 |
|
|
Types of Spina Bifida |
- Small gap with no clinical symptoms is spina bifida occulta (occult=hidden) - Wide laminar defect with either meninges or spinal cord protrusion is spina bifida vera or spina bifida manifesta |
|

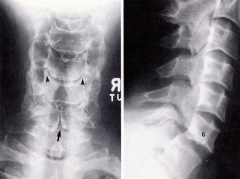
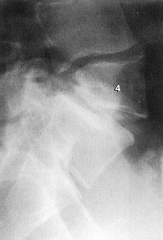
Congenital Block Vertebra |
- May be congenital or acquired (trauma) - Result of a failure of segmentation of somites, a process which normally occurs during the late first & second fetal month - Disc space is present, but is hypoplastic - Facet joint may be fused as well as spinous processes (50% of cases) - IVF is almost always present but may be altered in size |
|

Pons Posticus |
- Bony bridge arching between posterior arch & the lateral mass of C1 - Referred to as posterior ponticle or the pons posticus |
|
Cervical Spondlylisthesis |
- Rare anomaly - Characterised by absent pedicles bilaterally - Dysplasia of the articular processes - Spina bifida occulta - Most common at C6 - More common in males than females |
|

Klippel-Feil Syndrome |
- Presence of two or more blocks in the cervical & thoracic spine - Usually have a scoliosis, rib anomalies, deafness, congenital heart defects, hemi-vertebra etc. - Triad of findings: low hairline, webbed neck & decreased range of motion |
|
|
Ossiculum Terminale |
- Normal variant - Different from os odontoideum - Failure of union of the secondary ossification center at the tip of the odontoid - No clinical significance |
|
|
Ununited Apophyses |
- Normal variant - Most likely to occur at the C7 SP |
|

Hyperplastic Transverse Process |
- Normal variant - Can occur at any level - At C7: TP's extend laterally beyond those of T1 but are different to cervical ribs - At C1: TP's may enlarge and form accessory articulations with the occiput, limiting ROM |
|
Stylohyoid Ligament Calcification |
- Normal variant - From styloid process to hyoid bone - Usually asymptomatic, but can occasionally be painful |
|

Nuchal Bones |
- Normal variant - Calcific material or bone posterior to the Sp's within the nuchal ligament - Generally asymptomatic, incidental finding - May be associated with previous cervical trauma |
|

Thyroid Cartilage |
- Normal strucure that can simulate pathology - Occurs in almost everyone - Irregular mass on lateral projection - On the AP Lower Cx view, calcification of the greater horns is often mistaken for arterial calcification |
|

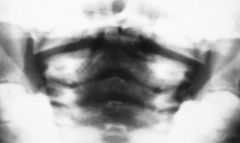
Laryngeal Constriction |
- Normal structure that can simulate pathology - On AP Lower Cx it is often mistaken for spina bifida occulta or fracture - Follow tracheal borders to differentiate |
|

Bifid Spinous Process |
- Normal structure that can simulate pathology - Confused with spina bifida occulta - Examine the spinolaminar line to DDx - Look at cortical margins: SBO will demonstrate 2 sclerotic lines indicating true bony seperation |
|

MACH Effects |
- Normal structure that can simulate a pathology - The edge of a structure will often project a lucency across another structure it is overlying - Classically illustrated at C1/2 where the posterior arch of C1 crosses over the dens simulating a dens fracture |
|

Teeth |
- Normal structure that can simulate a pathology - On the APOM, the space between the two upper incisors may project over the dens as a vertical lucency simulating fracture - Unlikely due to vertical dens fractures being exceedingly rare |
|
Pseudosublaxation of C1 |
- Normal structure that can simulate a pathology - In young children, the lateral masses of C1 grow faster than the articular porcesses of C2 - The lateral masses may overhang C2 simulating a burst fracture (Jefferson fracture) |
|

C2/3 Facets |
- Normal structure that can simulate a pathology - On the lateral view, orientation of the facets gives the appearance of fusion - Oblique views can help in ruling out fusion |
|

Facet Notching |
- Normal structure that can simulate a pathology - The superior articular surface of a facet may show a small notch - This is not an erosion |
|

Sprengel's Deformity |
- M:F 1:2 ratio - Reduced arm abduction, torticollis may be present - Small, high positioned scapula - Scapula is rotated with the glenoid fossa directed inferiorly - Associated anomalies include scoliosis, hemivertebrae, block vertebrae, spina bifida occulta & cervical ribs |
|
Rib Synostosis |
- Seen posteriorly and may involve two or more ribs - May be a contributor to congenital structural scoliosis - Synostosis of ribs 1 & 2 is known as SRB's anomoly |
|

Rib Anterior Bifurcation |
- Most common anomaly of the ribs |
|

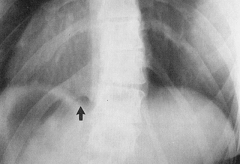
Intra-thoracic Rib |
- Supernumery rib - Intra-thoracic rib lies along the posterior thoracic wall & arising from a normally articulating rib |
|
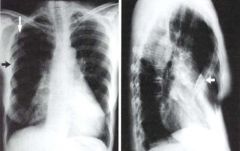
Pectus Excavatum |
- a.k.a Funnel breast, normally congential in nature - Sight of deepest depression of the sternum at the level of the xiphoid process - More common in males - Body of the sternum is longer in many case |
|
Pectus Carinatum |
- a.k.a Pigeon breast - Characterised by anterior protrusion of the upper sternum & it's costal cartilages, with flattening of both sides of the chest - Congenital malformation associated with congenital hypoplasia & weakness of the anterior segment of the hemidiaphragm |
|
|
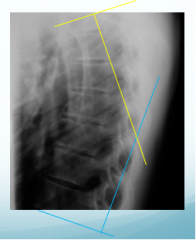
A.P. Thoracic Curve (Lateral View) - Line across superior endplate of T1 & a line across inferior endplate of T12 - Intersect perpendiculars to these lines - Normal measurements vary according to age - Generally increases with age |
|

|
Saggital Diameter of the Thoracic Canal - Measure from posterior border of bodies to spino-lamina junctions - In most cases difficult to find reference point and hence reliability is questionable |
|

|
Interpedicular Distance - Distance between medial aspects of pedicles - T6 - min 14mm, max 20mm |
|

|
Cardiothroacic Ratio - (TD) Transverse diameter of the heart - (ID) Internal diameter of the thorax - TD/ID X 100 = 39-50% (Average is 45%) |
|

Transtional Vertebra L5 |
- Sacralisation of L5 - Generally, findings involve enlargement of one or both transverse processes (hyperplastic or spatulate in appearance) - Hypoplastic disc space is frequently an associated finding |
|

Transitional Vertebra L1 |
- Lumbar ribs (See transitional vertebra L5) |
|
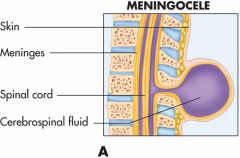
Meningocele |
- Meningocele is the soft tissue sac produced by protrusion of meninges only through a spina bifida defect - Related findings may include skin changes (hairy patch, pigmentation, fibrous tissue or prominent blood vessels - Lipoma may overlie the defect |
|
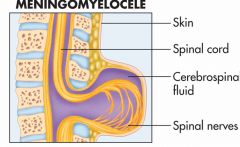
Myelomeningocele |
- A meningocele also containing spinal cord elements is referred to as a myelomeningocele - Related findings may include skin changes (hairy patch, pigmentation, fibrous tissue or prominent blood vessels - A lipoma may overlie the defect |
|

Schmorl's Nodes |
- Thought to be the result of nucleus pulposus herniation into the vertebral endplate - Common finding in the spine, affecting predominantly the lower thoracic & upper lumbar regions - Sometimes associated with Scheuermann's disease |
|

Notochordal (Nuclear) Impression |
- Broad based, curved cortical indentation of the endplate cartical surface - May be superior or inferior endplate - Normal finding in cervical spine |
|

Cupid's Bow Contour |
- Paramedian curvilinear indentations of the endplate - Typically inferior - Most common at L4 & L5 |
|
Butterfly/Sagittal Cleft Vertebra |
- Result of a failure of the lateral ossification centres of the vertebral body to unite - Findings may be masked in lateral view - Enlargement of the pedicles, increased interpeduncular distance & corresponding deforming of the adjacent vertebral endplates |
|
Limbus Bone/Limbic Vertebra |
- Non-union of the secondary growth centre for the corner of the vertebral body - Thought to result from the migration and herniation of nuclear material through this growth plate |
|

Basstrups Syndrome |
- Kissing spinous processes - Impingement between adjacent spinous processes - May be due to excessive lordosis, hyperplastic SP's or DJD motion |
|
Hemi-vertebra |
- One half of a vertebral body's ossification centre fails to develop - Dorsal hemivertebra indicates development of the posterior portion of the body only - Ventral hemivertebra indicates development of the ventral portion of the body only |
|

Knife-Clasp Deformity |
- Spina bifida of S1 plus an elongated and vertically orientated SP of L5 - SP may impinge on canal contents on extreme extension and cause pain |
|
Congential Pedicle Absense |
- Contralateral pedicle with show sclerotic changes - Must DDX from a destructive process such as mets or neurofibromatosis which will not show scelotic changes of the opposite pedicle |
|

Types of Spondylolithesis |
Type 1 = Dysplastic or aplastic (congenital abnormality allows displacement with weight bearing)
Type 2 = Isthmic (Stress fracture of the pars oracute fracture of the pars) Type 3 = Degenerative (secondary to long standingDJD, can be confused with pseudo spondylolisthesis) Type 4 = Traumatic (secondary to fractures in theposterior arch other than the pars) Type 5 = Pathological (in conjunction with generalised or localised bone disease, pagets, metastasis etc.) |
|

Pars Defect |
Type 2 Spondylolisthesis |
|

Facet Tropism |
- Requires an understanding of what is normal for that particular level and picking the facet that has turned from normal (ie. undergone facet tropism) |
|
|
Facet Assymetry |
- Where facets at the same motion unit are not running in the same plane - Generally easy to pick those facets that are running sagittal - Most coronal facets appear the same regardless of how much they are angled |
|
Oppenheimer's Ossicle |
- Non union of the tip of the inferior articular process - M/C in the Lumbar - M/B Unilateral or Bi - Persistent nonunion of the inferior articular processes |
|

Paraglenoid Sulci |
- Transmits the superior branch of the gluteal artery & supplies insertion for SI ligament - Rare in males - Usually bilateral - AKA Pre-auricular sulcus |
|
Os Acetabuli |
- Ossicle located at acetabular rim - Considered as unfused secondary ossification centres or fatigue fractures caused by overload or impingement |
|

|
Pubic ears |
|

Vascular Channels (Pelvis) |
Normal variant |
|

Bilateral Iliac Horns |
- Fong’s syndrome - Iliac horns, combined with dysplastic fingernails, hypoplastic or absent patellae |
|

Hahn's Venous Clefts |
- Venous channels - Transverse, short lucent line in the mid portion of the vertebral body - Most common in lower thoracic spine - May appear to disrupt posterior vertebral body margin - May be single or multiple |
|

Injection Granuloma |
- Cystic Calcification seen at site of muscular injections - Usually within the posterior lateral buttocks - Represents fat necrosis with subsequent calc. - Seen with corticosteroid therapy - Used with inflammatory processes such as Systemic Lupus Erythematosus or RA - Long term steroid use may lead to excessive bone demineralization |
|
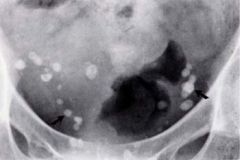
Phleboliths |
- Concretions, representing calcification of thrombi attached to the walls of veins - Most frequently seen within the pelvic basin below the ischial spines - The significance of phleboliths is undefined |
|

Inguinal Skin Folds |
Appears as a break/fracture |
|

George's Line (Lumbar) |
- Line drawn on the posterior margins of vertebral bodies following posterior longitudinal ligament - The line should be smooth, regular and uninterrupted |
|

Lumbar Angle of Lordosis |
- a.k.a Lumbar Curve Angle - Draw lines along superior endplate of L1 & inferior endplate of L5 on lateral view - Then draw perpendiculars to these lines - Measure the superior or inferior angle 35-45 degrees is “normal” < 35° = hypolordosis (disc herniation, muscle spasm, etc.) > 45° = hyperlordosis (facet syndrome, swayback posture, etc.) |
|

Lumbosacral Disc Angle |
- Draw lines along inferior endplate of L5 and sacralbase
- Anterior angle formed should be within 10-20 degrees - The lines should intersect posterior to IVF > 20° = DJD facets, potential facet imbrication < 10° = possible acute disc herniation |
|
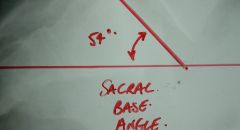
Sacral Base Angle |
(Ferguson’s Sacral Base Angle) - One line along sacral base, the other parallel to bottom of film - Posterior or anterior angle should be 26-57° - It is suggested that an increased angle stresses the facet joints |
|

Lumbar Gravity Line |
(Ferguson’s Weightbearing Line) - Draw a vertical line down from center of L3 - Should intersect the anterior 1/3 of sacral base - If anterior to sacrum, indicates anterior weight bearing; if anterior more than 10 mm, suggests anterior shearing stress on facets - If line falls in posterior 2/3 of sacrum, it indicates posterior weight bearing and possible facet imbrication |
|

Meyerding’s Grading Method for Spondylolisthesis |
- To classify a spondylolisthesis, the sacral base is divided into four equal parts - The relative position of the posterior-inferior corner of the fifth lumbar body to these segments is made - Note, this method of grading could be applied to any level where a listhesis has occurred |
|

Ullmann's Line |
- Line extended upward at a 90 degree angle to thesuperior surface of the sacral base at its anterior margin - That line should not intersect the L5 body |
|

Interpedicular Distance |
- On the AP, the distance between the medial aspect of the pedicles is measured - The measurements vary depending on age and spinal level - The distance increases as you go caudally - Increased distance = tumour or anomaly - Decreased distance = stenosis or dysplasia - Sagittal dimension must also be evaluated |
|
Saggital Canal Measurement |
(Eisenstein’s Method) - On the lateral projection, one line connects the superior articular process with the inferior articular process - The second line is drawn along the posterior aspect of the vertebral body at the same level - Measure from the middle of the posterior vertebral body to the first line (minimum is 15mm) - Best to assess as a ratio of body size vs canal (below 15 mm =spinal stenosis) - The best way to determine the canal size is axial imaging such as C.T. or M.R.I. |
|
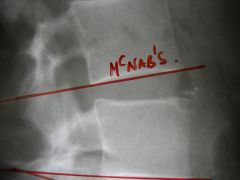
McNab's Line |
- Used to visualise facet imbrication (overlapping of facets) - Drawn from L2-4 but not L5 - A line drawn through the inferior body endplate - The superior facets of the vertebra below should be below this line |
|
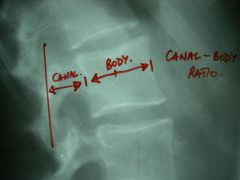
Canal to Body Ratio |
- Require both A-P and lateral views of lumbar spine - A-P view: distance between pedicles and width of vertebral bodies - Lateral view: A-P diameter of body and distance between body and articular process - Canal body ratio: A x B :C x D, the ratio will vary according to the lumbar level - The higher the ratio, the smaller the spinal canal (i.e. indicator of spinal stenosis) |
|

Koehler's Teardrop |
Not a true anatomic structure but a confluence of osseous structures: - Medial border = ilioischial line - Lateral border = medial acetabulum - Inferior border = inferior acetabular notch - “Teardrop Sign” =non-lucent interior may indicate pathology, such as blasticmetastasis |
|

Ischiopubic Synchondrosis |
- Irregular, bulbous appearance at the junction of the ischium and inferior pubic ramus just before closure - One side may finish development before the other - Once thought to be an area of osteonecrosis, but this theory has been discarded - It's not a tumor! |
|

Acetabular Roof |
- Normal stress on superior aspect of acetabulum leads to a sclerotic roof - Should NOT be confused with degenerative sclerosis - Wolff’s Law: bone responds to increased stress by increasing strength, and responds to decreased stress by decreasing strength |
|

Fovea Capitus (centralis) |
Attachment site of ligamentum teres appears as an erosion or osseous destructive process |
|
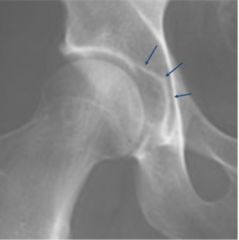
Superior Acetabular Notch |
- Superomedialbreak in the acetabular surface where the ligamentum teres attaches - Don’tconfuse with fracture |
|

Symphysis Pubis |
- Irregulararticular surfaces in the paediatric age group due to the amount of growthand stress occurring there - NOT a sign of inflammatory destruction - Cannot adequately assess this joint until after age 22-25, when growth is complete |
|

Prominent Ischial Spines |
- Ischial spines may appear to protrude deep into the pelvis - Actually form part of the posterolateral border of the pelvis - May simulate tumour |
|

Hip Joint Space Width |
- Superior joint space: space between most superior point of the femur articular surface and adjacent acetabular cortex (min 3mm) - Axial joint space: space between the femoral head and the acetabulum immediately lateral to the acetabular notch (min 3mm) - Medial joint space: space between the most medial surface of the femoral head and opposing acetabular surface (min4mm) |
|

Acetabular Depth |
- On an anterior posterior view a line is drawn from the superior margin of the pubis at the symphysis joint to superior lateral acetabular margin - The greatest distance from this line to the acetabular floor is measured (Male: min 7mm) (Female: min 9mm) |
|

Symphysis Pubis Width |
The distance measured is between the opposing articular surfaces, halfway between the superior and inferior margins of the joint |
|

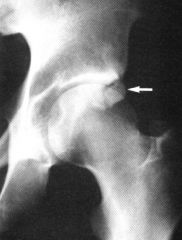
Shenton's Line |
Line following the inferior margin of the femoral neck which when continued into the pelvis should follow the superior margins of the obturator foramen |
|

Ilio-Femoral Line |
A line along the lateral margins of the ilium should continue as an unbroken curve along the superior margins of the femoral neck |
|
|
Skinners Line |
- A line at a 90 degree angle to long axis of femur at the superior margin of the greater trochanter continues into the pelvis and should fall at or below the fovea capitis - Difficult to attempt without a long bone study |
|

Femoral Angle |
Angle formed by the axis of the neck and the long axis of the shaft of femur |
|

Measurement of Protrusio Acetabuli |
- Kohler's line is drawn from pelvic border of ilium to medial border of body of ischium - If the acetabulum dome passes medially to Kohler's line a protrusio acetabuli is present |
|
Tear Drop Distance |
- Used for the early detection of Perthes disease - Distance from medial aspect of femoral capital epiphysis to vertical line drawn along the lateral margin of pelvic tear drop |
|

Klein's Line |
- A line is drawn tangential to the superior margins of the femoral neck - Bilateral examinations should be made - Assessment for slipped femoral capital epiphyses |
|

Triradiate Cartilage |
- The cortical surface of the pelvic brim appears to extend into the pelvic cavity - When combined with the lucency of the growth plate, it may simulate a fracture |
|

Hilgenreiner's Line (Y-Y Line) |
- On a paediatric A-P pelvis, a line drawn through the triradiate cartilage of both hips just inferior to the ilia, extending beyond the ilia - This is a baseline from which other measurements are made, and with no inherent significance |
|

Perkin's Line |
- A vertical line is drawn downward from the rim of the acetabular roof intersecting Hilgenreiner’s line, forming 4 quadrants - The femoral epiphysis should lie mainly in the lower medial quadrant - If the epiphysis lies in an outer quadrant, it may indicate subluxation (lower) or dislocation (upper) |
|

Acetabular Angle or Index |
- Anoblique line is drawn connecting the superior acetabular rim to Hilgenreiner’sline at its intersection with the lowest aspect of the ilium - Thelateral angle formed should be no more than 30° degrees, with not more than 5°difference bilaterally - Anangle above either limit may indicate congenital hip dysplasia |
|

Risser's Sign |
- Pelvicossification centres - Primary= 3 centres (ilium, ischium, and pubis) join at 7-8 years at the TriradiateCartilage; the ischiopubic synchondrosis alsofuses at 7-8 - Secondary= Appear throughout pelvis around puberty and unite between 15-25 years; found at acetabular rim (2 centres), iliaccrest, AIIS, ischial tuberosity, pubic symphysis - Risser’ssign = iliac crest apophysis used to determine remaining skeletal growth, appears from ASIS to PSIS, then ossifies |
|
Developing Epiphyses |
- Canbe very irregular and asymmetrical in the developing pediatric knee - Canbe confused with osteonecrosis of the, which looks similar - Clinicalcorrelation is essential (Always!) |
|

Zone of Provisional Calcification |
- Can be very sclerotic at times, possibly due to the amount of activity at the physis at the time of the x-ray - As long as the fibular zone is not equally sclerotic when compared to the femur and tibia, it is normal - Involvement of all three bones probably indicates heavy metal toxicity, such as lead poisoning |
|

Vacuum Cleft |
Maybe visible if the joint is under valgus or varus stress or distraction. |
|

Remnant Growth Plate |
- Scleroticline that sometimes replaces the physis after closure - Looks like impaction fracture |
|

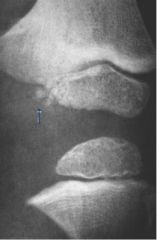
Patellar Position |
- On the lateral view, the length of the patella (pole to pole) is compared to the length measured from the inferior pole of the patella to the superior notch of the tibial tuberosity - The lengths should be equal, with up to 20% difference being insignificant - The knee MUST be flexed to 45° to take this measurement |
|

Axial Relationship of Knee Joint |
- AB (blue): Mid femoral shaft - CD (purple): Mid Tibial shaft - EF (orange): Tangents across distal articular surfacesof femur - GH (yellow): Tangents to distal aspects of Tibialarticular surfaces |
|

Ankle/Foot Stress Views |
- Usually inversion stress, since this is the most common ankle injury, but eversion may be done also - Evaluates ligamentous integrity |
|

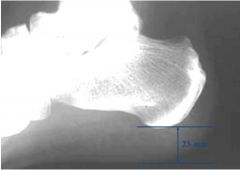
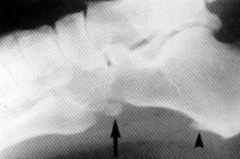
Boehler's Angle |
- A line is drawn from the highest point on the anterior part of the calcaneus to the highest point in the middle of the calcaneus - A second line is drawn from the central highest point of the calcaneus to the posterior highest point - The smaller angle formed at the intersection of these two lines is Boehler's angle - The small, posterior angle should be at least 28° - Less than 28° = calcaneal fracture or dysplasia |
|
Heel Pad Thickness |
Shortest distance between the plantar surface of the calcaneus and external skin contour is measured |
|
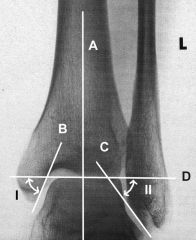
Ankle Lines |
A. Long axis of tibial shaft: this line is continuous with vertical axis of the talus B. Line tangent to articular surface of medial malleolus C. Line tangent to articular surface of lateral malleolus D. Line drawn at tangent to the superior edge of dome of talus - Fibular Angle (FA) = Angle formed between D and C - Tibial angle (TA) = Angle formed between D and B |
|

Axial Angle |
- AB: Axis of the shaft is drawn between 2 points each measured to lie in the midline of the diaphysis - CD: Line between apex of the greater tuberosity to the junction of the shaft with the distal extremity of the articular surface of the head (the point where the medial cortex changes from a band to a line) - Normal 60 degrees |
|

Width of Joint Space (Shoulder) |
- Measured between anterior rim of the glenoid fossa and medial aspect of the humeral head - Average is 4-5mm |
|

Fat Pad Sign |
- Normal - Also in wrist/hand |
|

Congential Hip Dysplasia |
- Acetabular and femoral head deformities together with dislocation of the hip joint at birth can be grouped together as examples of congenital hip dysplasia (CHD) - Dislocation can be evaluated for at birth using orthopaedic tests such as Ortolani’s and Barlow’s tests - Positive findings would lead to hip radiographs being taken which should demonstrate some or all of Putti’s triad - Radiographic findings may include: small or absent femoral capital epiphysis, lateral displacement of the femur & increased acetabular angle (putti’s triad) |
|

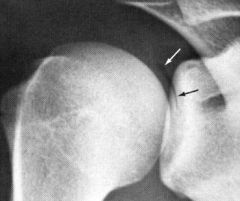
Bipartite Patella |
- Normal knee variant - Maturepatella made of two pieces - Separatefragment at upper/ outer quadrant - Bilateralin 80% |
|

Tripartite Patella |
- Normal knee variant - Mature patella made of 3 pieces - "Multipartite”= >3 pieces |
|

Ludloff's Patch |
- Normal knee variant - A lucency in the distal femoral epiphysis - Best seen around the age of 16 years |
|

Os Fabella |
- Normal knee variant - Sesamoid bone within the tendon of the lateral head of the gastroc - Bilateral in 2/3 to 3/4 More common in Males: - Round or oval - Well corticated |
|

Talar Beak |
- Normal ankle variant - An osseous projection off the anterior/ superior talar neck |
|

Calcaneal Apophysis |
- Normal ankle variant - A fragmented and sclerotic appearance to the calcaneal apophysis - Given the name Sever’s Disease |
|

Tarsal Coalition |
- Normal ankle variant - A fibrous or osseous union between two tarsal bones |
|
Os Peroneum |
- Normal ankle variant - Located adjacent to the cuboid |
|

Os Trigonum |
- Normal ankle variant - Located posterior to the ankle joint |
|

Phalangeal Synostosis |
- Normal foot variant - a.k.a symphalangism |
|

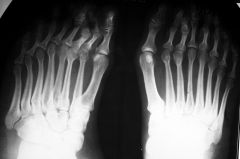
Hallux Valgus |
- Normal foot variant - Lateral deviation of the first digit - Medial protrusion of proximal 1st MT - May be associated with a bursa medial to the 1st MTP joint - May be congenital, but most likely relates to improper footwear |
|
Polydactyly |
- Normal foot variant - Increase in number of fingers and toes |
|

Duplication of the 1st Digit of the Foot |
Normal foot variant |
|

Rhomboid Fossa |
- Normal shoulder variant - Developmental variation at the attachment site of the costoclavicular ligament |
|
Vacuum Phenomenon |
- Normal shoulder variant - A radiolucency noted in the joint space - Represents gas within the joint capsule |
|
Supraclavicular Foramen |
- Normal shoulder variant - Allows passage of the medial branch of the supraclavicular nerve |
|

Pseudotumor Appearance |
- Normal shoulder variant - Cystic appearance produced by the greater tuberosity |
|

Olecranon Foramen (aka Supratrochlear Foramen) |
Normal elbow variant |
|

Radioulnar Synostosis |
- Normal elbow variant - Usually bilateral - May decrease supination or pronation |
|

Supracondylar Process |
- Normal elbow variant - An osseous projection on the anteromedial aspect of the distal humerus - Struther’s ligament may extend inferiorly from this process to the medial epicondyle - May cause neurovascular signs or symptoms |
|

Carpal Coalition |
- Normal wrist variant - Fusion between the capitate and hamate possibly involving the triquetrum and pisiform |
|

Madelung's Deformity |
- Normal wrist variant - Delayed growth of medial distal radius - May result in a posterior subluxation of the ulna |
|

Syndactyly |
- Normal hand variant - A defect of mesenchymal organization resulting in any degree of webbing or fusion of the fingers or toes |
|

Vascular or Nutrient Canals |
Normal hand variant |
|

Sesamoid Bones of the Hand |
Normal hand variant |
|

Duplication of the 1st Distal Phalanx |
Normal hand variant |