Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
60 Cards in this Set
- Front
- Back
|
What are the two podocytopathies?
|
Minimal change disease
Focal segmental glomerulosclerosis |
|
|
What are important findings in minimal change disease?
|
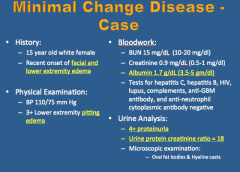
Facial and lower extremity edema
Pitting edema Low albumin 4+ proteinuria Urine protein creatinine ration = 18 |
|
|
Describe the following in minimal change disease:
Age Most common cause of ... Onset of edema BP Renal function What type of proteinuria? |
|
|
|
Pathogenesis of minimal change disease?
Two major types? Causes of each type? |
|
|
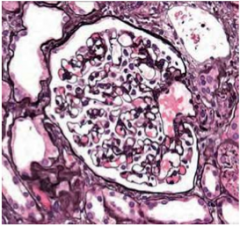
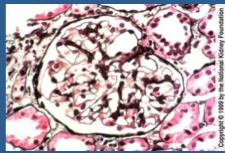
What is shown here? Pathology?
|
Glomerulus
Minimal! |
|
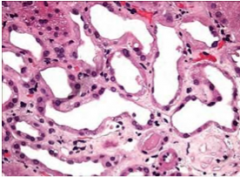
What is shown here? Pathology?
|
Tubules
Minimal! |
|
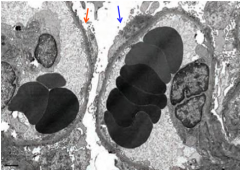
What is shown with each arrow? Red and blue.
|
Red = detachment of foot processes
Blue = effacement of foot processes |
|
What is shown here?
|
Answer from class.
|
|
|
What is the cornerstone of treatment for minimal change disease? Children have the best response to what? Is this the same for adults? Is recurrence common? What should you do if there is a poor response to a steroid?
|
|
|
|
What are some common clinical findings in focal glomerulosclerosis?
|
Lower extremity edema
Hypertension Pitting edema High creatinine Low albumin 4+ proteinuria Urine protein/creatinine ratio elevated |
|
|
Is FSGS increasing in incidence?
Is proteinuria selective in FSGS? Is hypertension present in FSGS? 50% of patients with FSGS develop what within 10 years of diagnosis? |
|
|
|
What is the "novel discovery" that is in the circulation in patients with primary FSGS?
|
suPAR
|
|
|
What does the suPAR do?
|
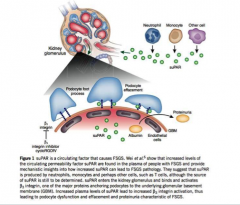
Produced by neutrophils, monocytes, and T cells -> enters glomerulus --> binds and activates B3 integrin, anchoring protein of GBM
|
|
|
What are the two major types of FSGS?
|
Primary and secondary
|
|
|
What is the cause of primary FSGS?
|
Idiopathic
|
|
|
What are causes of secondary FSGS?
|
Familial
Infection Drugs Adaptive structural-functional response (loss of nephron mass -> partial removal of kidney tissue) |
|
|
What are some familial secondary causes of FSGS?
|
Mutations in genes for alpha-actinin-4, podocin, and TRCP6
APOL1 |
|
|
What are infectious causes of FSGS?
|
HIV, parvo virus
|
|
|
What are some drugs that cause FSGS?
|
Pamidronate, heroin, lithium
|
|
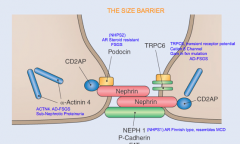
How are these proteins of the podocyte slit diaphragm involved in proteinuria?
|
Answer from class
|
|
|
What is the significance of APOL1 in the secondary cause of FSGS?
|
A sequence variant in the apolipoprotein L1 gene (APOL1) on chromosome 22 appears to be strongly associated with an increased risk of FSGS and renal failure in individuals of African descent.
� |
|
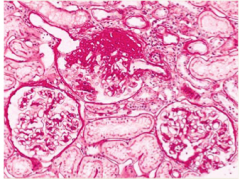
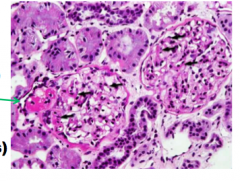
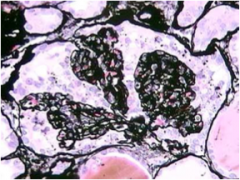
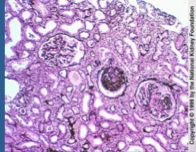
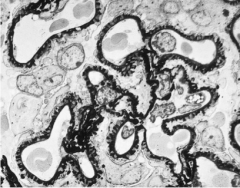
What is shown here?
|
Focal segmental glomerulosclerosis:
One involved, two uninvolved glomeruli, illustrating that it is focal. Involved glomerulus has a large area of disease, illustrating that it is segmental. |
|
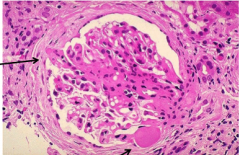
What is shown here?
Green arrow? Black arrows? |
Focal segmental glomerulosclerosis:
Hyalinosis: accumulation of leaked plasma proteins and lipids. Large accumulation = green arrow Small accumulation = black arrow |
|
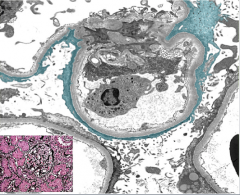
What is shown here? What is each arrow pointing to?
|
Focal segmental glomerulosclerosis
Left = adhesion of involved segment to Bowman capsule Bottom = hyalinosis |
|
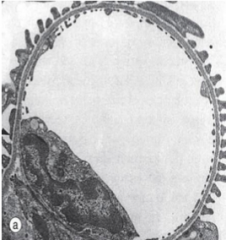
What is this?
|
Normal glomerulus
|
|
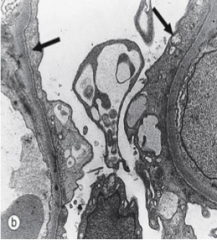
What is this?
|
Focal segmental glomerulosclerosis = foot process effacement (similar to minimal change disease)
|
|
|
What are the five subtypes of FSGS? In order of frequency.
In which two will you see heavier proteinuria? Which of these has the worst survival and which is more likely to obtain remission? |
Not specified
Perihilar Tip Collapsing Cellular Collapsing = worst Tip = remission |
|
What is the stain? What is the type of FSGS?
|
Silver stain = collapsed BM and two adhesions
Collapsing type FSGS |
|
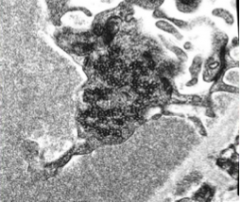
What is shown here?
|
Electron microscopy of collapsing type FSGS.
|
|
|
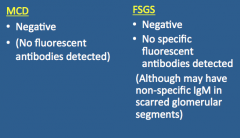
In MCD and FSGS what will immunofluorescence microscopy be?
What might you see in FSGS? |
|
|
|
How do you treat FSGS?
Which is most commonly used? What are other treatment options? |
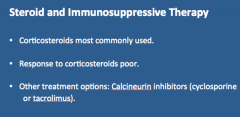
Steroid and immunosuppressive therapy.
|
|
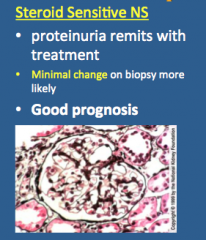
What is shown here? Does proteinuria remit with treatment? What is more likely on the biopsy? Prognosis?
|
|
|
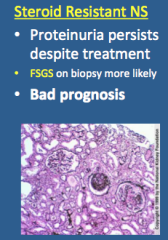
What is shown here? Does proteinuria persist despite treatment? What is more likely on biopsy? Prognosis?
|
|
|
|
True or false:
MCD and FSGS may be part of the same disease spectrum. Why is sampling error possible in some cases? |
True
FSGS is focal and localized more to the deep juxtamedullary glomeruli |
|
|
What may develop in children with repeated relapses of MCD with steroid responsive nephrotic syndrome?
|
FSGS secondary to repeated renal injury supporting an evolution process.
|
|
|
Non-scarred glomeruli of patients with FSGS resemble those of what?
|
MCD
|
|
|
Loss of glomerular capillary charge barrier in both MCD and FSGS leads to what? What is the difference between the two?
|
Heavy proteinuria --> may be less selective is FSGS secondary to large pores
|
|
|
What is shown in bright red? Weird orange/red color?
How do they appear? Why can't large circulating immune complexes deposit in the subepithelial regions? Filtered antibody interacts with what? What may the endogenous antigen be? |
1. Post infectious glomerulonephritis
2. Membranous nephropathy May be assembled locally by "in situ" interaction or deposited antigen with filtered antibodies Large circulating immune complexes cannot deposit in the subepithelial regions as they are too big to pass through the glomerular basement membrane (GBM) Filtered autoantibody interacts with a locally generated endogenous antigen Endogenous antigen may be a protein or glycoprotein expressed on the podocyte cell membrane |
|
|
What are the two models of membranous nephropathy (in situ formation)?
|
1. Filtered "cationic" antigen
2. Autoimmunity model |
|
|
Explain the filtered cationic antigen model of membranous nephropathy (in situ).
Provide an example: |
Deposits --> cross endothelium and GBM --> localize in SUBEPITHELIAL SPACES as restricted by size of slit diaphragm --> antibodies localize and cause nephritis
Endostreptin, NSAP, SPEB in acute post-streptococcal glomerulonephritis (APSGN) |
|
|
Explain the autoimmunity model of membranous nephropathy (in-situ):
Which one do you see in primary MN? Congenital MN? |

Autoimmunity model --> locally generated antigen and filtered antibody
Primary = M-type phospholipase A2 receptor (PLA2R) Congenital = Neutral endopeptidase, NEP |
|
|
What is the autoantibody in idiopathic (not secondary MN)?
|
Autoantibodies to M type phospholipase A2 receptor (PLA2R)
|
|
|
Where is PLA2R expressed?
|
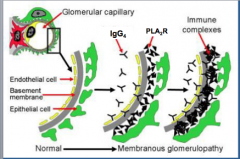
Expressed by podocytes in normal human glomeruli and was co-localized with IgG4 in immune deposits in glomeruli of patients with idiopathic MN.
|
|
|
Two types of MN?
Causes of secondary: Infection Autoimmune Drugs Maligancy |
Primary and secondary
Infection = Hep B, syphilis, malaria Autoimmune = SLE Drugs = gold, penicillamine, captopril, NSAID Malignancy = lung cancer, colon cancer, melanoma |
|
|
What is the most common cause of nephrotic syndrome in Caucasian adults?
When is the peak incidence? Male/Female? What percent spontaneously resolve? What percent progress to renal failure? What percent proteinuria with variable renal dysfunction? |
|
|
|
What are some risk factors for loss of renal function in MN?
|
|
|
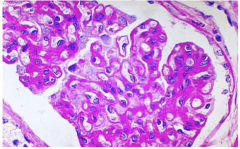
What is shown here?
|
MN
Thickened basement membrane without increased cellularity |
|

What is shown here?
|
MN: immunofluorescence
Granular deposits of immunoglobulin (IgG) and complement (not shown but would look the same) |
|
What is shown here?
|
Membranous Nephropathy:
Diffusely thickened basement membrane with subepithelial deposits separated by spikes of new GBM (“spike and dome” pattern). |
|

What is shown here?
|
MN:
Thickened basement membrane with subepithelial deposits (colored blue here) separated by spikes of new GBM (“spike and dome" pattern) |
|
|
Is MN nephrotic or nephritic? Why? Comment on the resolution of subepithelial deposits if the disease is secondary.
|
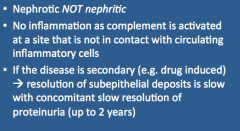
|
|
|
What occurs in the prescence of subepithelial deposits?
What is the mechanism? What is washed away into urinary space? |
Retraction and effacement of podocyte foot processes
Complement dependent process mediated by membrane attack complex (C5b-9) Intermediate chemotactic fragments (C3a and C5a) |
|
|
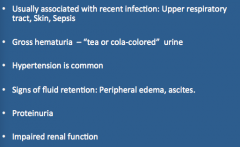
What are some indications of post-infectious glomerulonephritis?
|
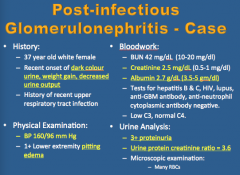
Dark color urine, weight gain, decreased urine output
BP increased Pitting edema High creatinine Low albumin 3+ proteinuria Urine protein ratio about 3 |
|
|
Again, indications of PIGN?
|
|
|
|
What are common lab results in PIGN?
|
Low C3 and normal C4 (alternative pathway activation)
Elevated anti-streptolysin O (ASO) titers if preceded by throat infection Elevated anti-DNAse B titers if preceded by skin infection Positive blood culture in sepsis |
|
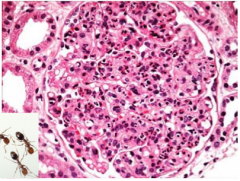
What is shown here?
|
Post streptococcal glomerulonephritis
Diffuse endocapillary proliferation and infiltration by numerous neutrophils "polys" look like ants |
|
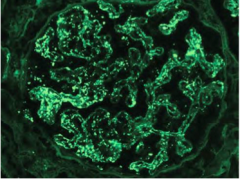
What is shown here?
|
Immunoflourescence of post-streptococcal glomerulonephritis: Diffuse granular deposits in capillary walls and mesangium (especially IgG and C3)
|
|
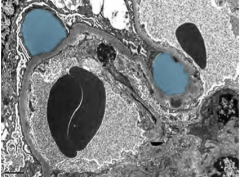
What is shown here?
|
PSGN
"Dome shaped" subepithelial humps in blue! |
|
|
How do you treat PIGN? Supportive measures?
|
Supportive = control hypertension (antihypers and diuretics), renal replacement therapy (if severe kidney dysfunction)
Treatment = treat underlying infection |
|
|
Prognosis of PIGN?
|
Good prognosis with resolution of hypertension
Normal C3 levels by 6 weeks Resolution of hematuria within 12 months |