Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
80 Cards in this Set
- Front
- Back
|
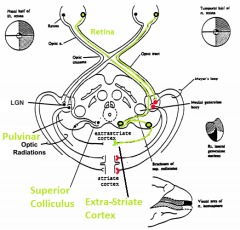
What are the two major visual pathways? |
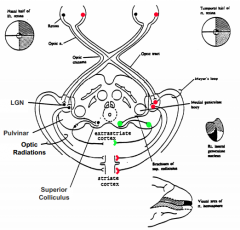
- Geniculo-Striate System (red)
- Retino-Tectal System (green) |
|
|
What is the function of the geniculo-striate system?
|
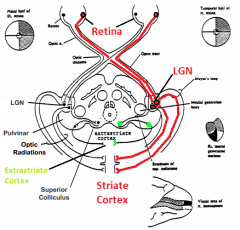
Conscious Visual Perception
|
|
|
What is the function of the retino-tectal system?
|
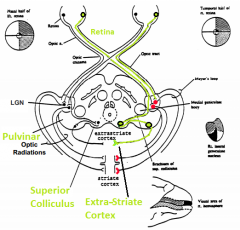
Directing eye movements and visual attention
|
|
|
What is the pathway of fibers through the geniculo-striate system?
|
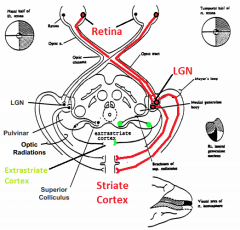
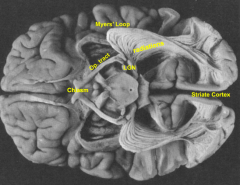
- Retina (via optic n., optic chiasm, and optic tract)
- Lateral Geniculate Nucleus (LGN) (via Meyer's loop) - Striate Cortex - Extrastriate Cortex |
|
|
What is the pathway of fibers through the retino-tectal system?
|
- Retina
- Superior Colliculus - Pulvinar - Extrastriate Cortex |
|
|
If you hear a loud noise and respond to it, which visual system are you using?
|
Retino-tectal system (directs eye movements and visual attention)
|
|
|
What is the name of the primary visual cortex?
|
Striate cortex
|
|
|
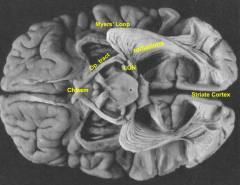
What is the pathway from the lateral geniculate nucleus to the striate cortex?
|
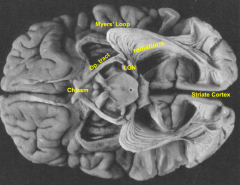
Optic radiations (Myer's Loop)
|
|
|
How can damage to the temporal lobe affect vision?
|
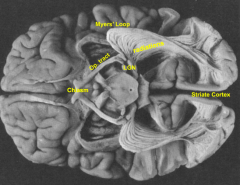
- Can damage Myer's loop (part of the optic radiations)
- Would lead to a restricted visual field defect |
|
|
What is a common side effect of temporal lobectomies? Why would this procedure be done?
|
- Damage to Myer's Loop (leads to restricted visual field defect)
- Used to relieve temporal lobe epilepsy |
|
|
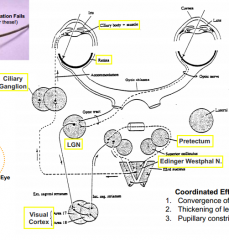
Retinal signals controlling pupillary constrictor muscles travel through what structures?
|
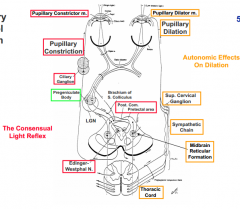
- Receptor in retina detects light (optic n. --> optic chiasm --> optic tract)
- Fibers synapse at pregeniculate body - Fibers continue to pretectal area and some cross to opposite side on posterior commissure (to get consensual response) - Fibers synapse at Edinger-Westphal Nucleus in midbrain - Travel back to ciliary ganglion on CN III - Synapse at ciliary ganglion - Fibers innervate pupillary constrictor m. |
|
|
What structure is responsible for the consensual pupil response?
|
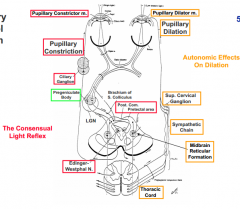
Some fibers cross to other side of midbrain via Posterior Commissure (in pretectal area)
|
|
|
If there is damage to the midbrain that cuts the posterior commissure, what is the effect?
|
No consensual light reflex response
|
|
|
What is the pathway for dilating the pupil?
|
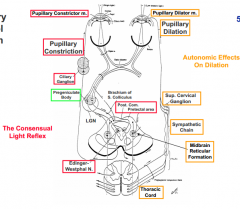
- Retinal receptors respond to decrease in light (CN II --> optic chiasm --> optic tract)
- Fibers synapse at pregeniculate body - Fibers continue to Midbrain Reticular Formation - Fibers descend to thoracic spinal cord - Head to sympathetic chain and synapse at Superior Cervical Ganglion - Fibers innervate Pupillary Dilator m. |
|
|
What does emotion do to the pupils?
|
Can cause dilation via the sympathetic autonomic system
|
|
|
What is accommodation?
|
Focusing the eye
|
|
|
What is the pathway of fibers for accommodation?
|
- Retinal ganglion cells (CN II --> optic chiasm --> optic tract)
- Synapse at Lateral Geniculate Nucleus (LGN) - Fibers go to visual cortex - Pass through pretectal area and synapse at Edinger Westphal Nucleus - Fibers continue back to ciliary body, synapsing at ciliary ganglion |
|
|
What muscles are responsible for accommodating the eye?
|
Ciliary body muscle
|
|
|
When the ciliary muscle contracts, what happens to the lens?
|
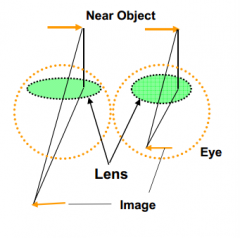
Lens thickens - increased optical power (see better nearby)
|
|
|
What happens when the ciliary muscle relaxes?
|
Lens flattens
|
|
|
What three things happen when attention is directed to nearby objects?
|
1. Convergence of the 2 eyes
2. Contraction of the ciliary muscle to thicken the lens 3. Pupillary constriction |
|
|
What is the effect of the lens thickening?
|
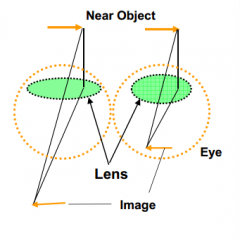
Increases optical power so that you can see up close
|
|
|
Why do old people have to wear bifocals?
|
Accommodation fails (ciliary muscle doesn't contract as well to thicken the lens)
|
|
|
Why does pupillary constriction help you to see objects up close?
|
- Increases depth of field (increases range over which image is focused)
- If you look through a small hole your vision will be sharper even without glasses |
|
|
How is accommodation different from the pupillary reflex?
|
- Can be voluntarily controlled
- Regulated by a negative feedback mechanism that automatically adjusts the focal power of the lens - Pathway includes cerebral cortex, only such reflex pathway |
|
|
Why is the visual cortex needed for the accommodation reflex and not pupillary reflexes?
|
Cortex is needed for analysis to determine if the image is blurry (out of focus)
|
|
|
What happens to the topography of the receptor array (retina) as the signal is transmitted through the rest of the brain?
|
Retinotopy is preserved
|
|
|
What is the difference between the visual field and the image on the retina?
|
Reversed (left is right) and Upside-down (top is bottom)
|
|
|
How is the retintopy preserved?
|
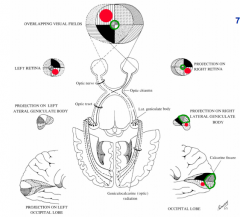
Fibers in adjacent ganglion cells in each hemiretina stay together
|
|
|
What happens to fibers from the nasal half of the retina (nasal hemiretina)?
|
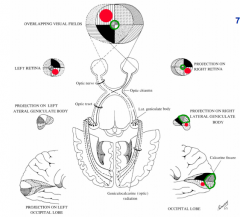
Cross in the optic chiasm so that fibers from the same visual field in each eye travel together
|
|
|
What happens to fibers from the temporal half of the retina (temporal hemiretina)?
|
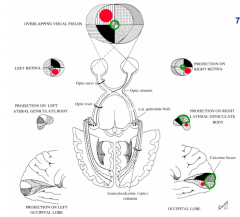
Do not cross via the optic chiasm - stay on the same side
|
|
|
The fovea has what kind of distribution?
|
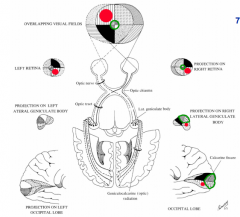
Greatly expanded (green) relative to the periphery
|
|
|
The R half of the retina sees what part of the visual field? Which side of the brain does it project to?
|
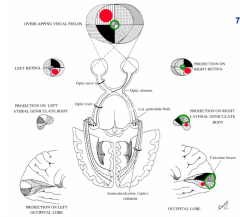
- R half of retina on each eye sees L visual field
- R half of retina projects to R side of brain (follow black quadrant or red dot) |
|
|
The L half of the retina sees what part of the visual field? Which side of the brain does it project to?
|
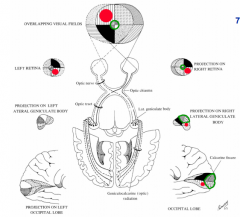
- L half of retina on each eye sees R visual field
- L half of retina projects to L side of brain (no black quadrant in LGN or cortex) |
|
|
If you lesion the L LGN, what will the deficit be?
|
Lose R half of visual field from each eye
|
|
|
If you lesion the R LGN, what will the deficit be?
|
Lose L half of visual field from each eye
|
|
|
Why is there a cortical over-representation of the fovea?
|
- Enhanced acuity at center of gaze
- Fovea contains more ganglion cells than the periphery --> more fibers and cells --> more corteical area |
|
|
What is the benefit to having a cortical over-representation of the fovea and under-representation of the periphery?
|
- Greatest detail and information from center of gaze
- Wide coverage and less detail of periphery |
|
|
Lesions of visual cortex that affect the fovea lead to what deficits?
|
Severe deficits
|
|
|
Lesions of visual cortex that affect the periphery lead to what deficits?
|
Can go unnoticed (unless the physician is alert enough to test this in detail)
|
|
|
What would be a possible reason for mapping the human visual cortex with a fMRI?
|
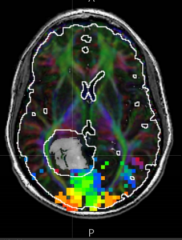
Pre-surgical planning:
- Tumor (gray) near visual cortex (colored pixels) - Want to remove tumor without damaging vision if possible |
|
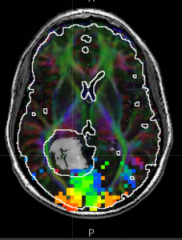
What do the colors represent on this fMRI?
|
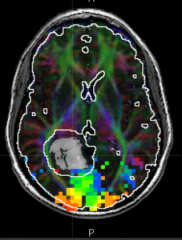
- Red/orange represent the center of the gaze
- Blue/green represents periphery |
|
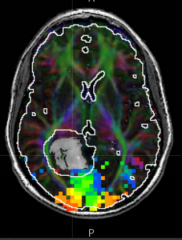
How come you can see the afferent visual pathways in this fMRI?
|
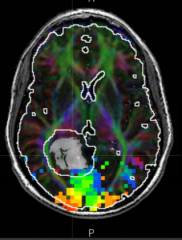
Diffusion Tensor Imaging (DTI) identified the white matter tracts
|
|
|
How can you see the tumor (gray)?
|
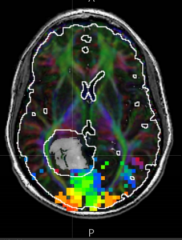
Fluid Attenuated Inversion Recovery MRI (FLAIR)
|
|
|
What does the white line/circle around the tumor represent?
|
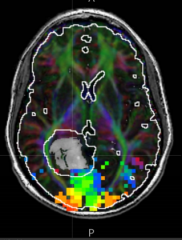
5 mm distance - high likelhood of being damaged if tumor is fully resected during surgery
|
|
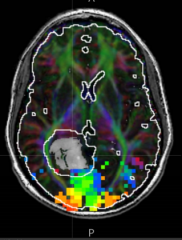
What is the most critical thing to be aware of when resecting this tumor (gray)? What could happen?
|
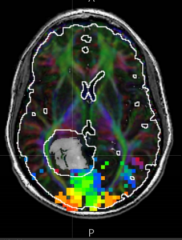
- The proximity of the optic radiation (green fiber track) near the lateral border of the tumor (within the 5 mm boundary / white outline) is the most concerning
- If this is cut would lead to complete hemianopia (loss of vision in a hemifield) |
|
|
What is a hemianopia?
|
Loss of vision in a hemifield
|
|
|
What is a quadrantanopia?
|

Loss of vision in a quadrant
|
|
|
What does the term homonymous mean?
|
Corresponding loss in each eye
|
|
|
What does the term heteronomous mean?
|
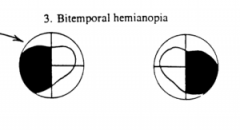
- Non-corresponding loss in each eye
- A loss of vision in either both nasal halves (binasal hemianopia) or both temporal halves of the visual field (bitemporal hemianopia) |
|
|
What would a lesion of the optic nerve on the right side cause?
|
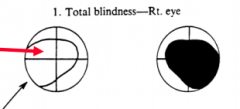
Total Blindness in right eye
|
|
|
What would a lesion of the R optic nerve near the optic chiasm cause?
|
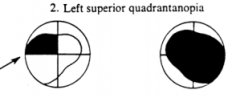
- Total blindness in R eye
- Left Superior Quadrantanopia |
|
|
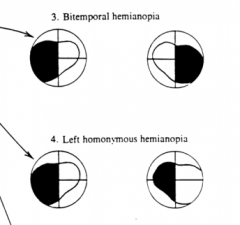
What would a lesion of the optic chiasm cause?
|
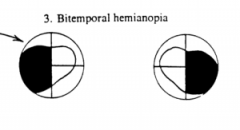
Bitemporal hemianopia (heteronomous hemianopia)
|
|
|
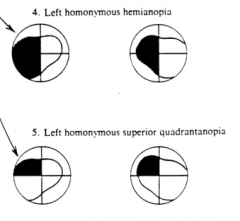
What would a lesion of the R optic tract cause?
|

Left Homonymous Hemianopia
|
|
|
What would a lesion of the Meyer's Loop (half of the optic radiations) on the R side cause?
|
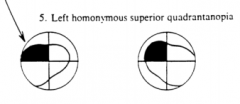
L Homonymous Superior Quadrantanopia
|
|
|
What would a lesion of all of the fibers going to the striate cortex / visual cortex on the R side cause?
|
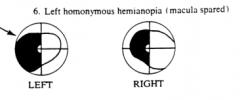
Left Homonymous Hemianopia (macula spared?)
|
|
|
What does a photoreceptor signal?
|
The intensity of light at a small point:
- Position (x,y) - Wavelength - Time - Eye (R vs L) |
|
|
If a photoreceptor only tells us intensity (position, wavelength, time, and which eye), how does the visual system figure out everything else that it is seeing?
|
- Many intervening stages --> hierarchy of visual areas
- Multiple pathways --> "parallel" processing streams |
|
|
Lesions to the extrastriate cortex, will show what kind of deficits?
|
- More functionally specific
- Selective loss of function (agnosias) rather than blindness |
|
|
What is an agnosia?
|
- Loss of ability to recognize objects, persons, sounds, shapes, or smells while the specific sense is not defective nor is there any significant memory loss
- Associated w/ brain injury or neurological illness |
|
|
What are the inferred attributes of vision from the retinal images and sensory cues regarding "what" you are seeing?
|
- 3D form (shape, size, rigidity)
- Surface properties (color - brightness/hue/saturation, visual texture, specular reflectance, transparency - shadows/highlights) |
|
|
What are the inferred attributes of vision from the retinal images and sensory cues regarding "where" things are that you are seeing?
|
- 3D spatial relationships (relative positions, 3D orientation in space)
- 3D movement (trajectory, rotation) |
|
|
What cortical area surrounds the calcarine fissure?
|
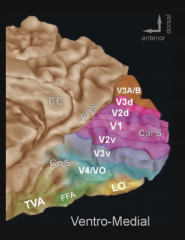
V1 - Primary visual cortex
|
|

What is CoS (to left of blue area)? POS (above purple)
|

CoS - Collateral Sulcus
POS - parieto-occipital sulcus |
|
|
What surrounds the Primary Visual Cortex (V1)?
|
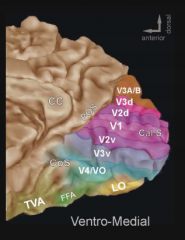
Second Visual Area V2d and V2v (dorsal/ventral)
|
|
|
What are the components of the higher-level extra-striate visual area?
|
V3, VP, V3A, V4, V8
|
|
|
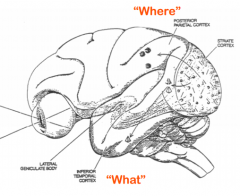
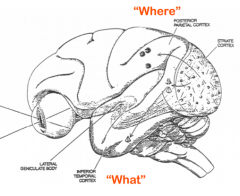
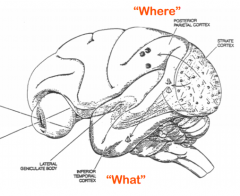
The extrastriate visual areas are organized into what two specialized systems? Functions?
|
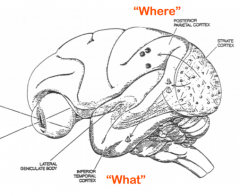
- Temporal Lobe Pathways (ventral pathway) - recognition of objects ("what is it?"
- Parietal Lobe Pathways (dorsal pathway) - localization of objects ("where is it?") |
|
|
Which special system pathway is involved in directing visual attention to an object of interest?
|
Parietal Lobe Pathways for localization
|
|
|
What are the visual implications of a lesion to the temporal lobe?
|
Impairs recognition
|
|
|
What are the visual implications of a lesion to the parietal lobe?
|
Impairs allocation of attention, "attentional neglect"
|
|
|
The parietal lobe pathway / dorsal pathway has also been termed what? Why?
|
"Action" Pathway - emphasizes its role in how visual information is used
|
|
|
The ability to navigate the world using a mental "map" involves what parts of the brain?
|
Medial Temporal Lobe
Hippocampus |
|
|
Lesions of what parts of the brain produce blindness?
|

Up to and including V1 (and probably V2)
|
|
|
Deficits in visual areas beyond V1 can cause what issues?
|
Selectively impair different aspects of visual perception without causing complete blindness
|
|
|
What is hMT+? What does a lesion of this area cause?
|
- Human Middle Temporal visual area plus surrounding motion sensitive areas
- Selective loss of motion perception (just see flashes of stillframes, not a smooth progression) |
|
|
What are V4/V8 a part of? What does a lesion of this area cause?
|
- Components of higher-level extrastriate visual areas
- Cerebral achromatopsia (caused by damage to the cerebral cortex of the brain, rather than abnormalities in the cells of the eye's retina) |
|
|
What is FFA? What does a lesion of this area cause?
|
- Fusiform Face Area
- Prosopagnosia - inability to recognize familiar faces - Often accompanies cerebral achromatopsia (lesion of V4/V8) |
|
|
What is PVA? What does a lesion of this area cause?
|
- Complex of an unknown number of parietal visual areas
- Primarily on R side, lesions cause attentional neglect |
|
|
What is achromatopsia? What causes it?
|
- Loss of color vision due to cerebral cortex injury
- Lesion of V4/V8 |
|
|
What is prosopagnosia? What causes it?
|
- Inability to recognize familiar faces
- Lesion of FFA (fusiform face area) |