![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
123 Cards in this Set
- Front
- Back
|
Space of Retzius AKA Retropubic Space |
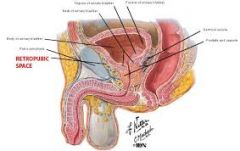
Between anterior wall of bladder & symphysis pubis |
|
|
Abnormalities in the Space of Retzius will push bladder....? |
Posterior |
|
|
Abdominal or pelvic masses will push bladder....? |
anterior OR inferior |
|
|
Vesicouterine Pouch AKA anterior cul-de-sac |
Between bladder & anterior uterus |
|
|
Pouch of Douglas AKA posterior cul-de-sac AKA Rectouterine pouch |
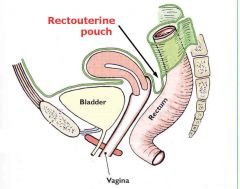
In between posterior uterus & rectum |
|
|
Which pelvic space will we refer to a lot while scanning? (common for free fluid) |
posterior cul-de-sac |
|
|
Sacrum and Coccyx |
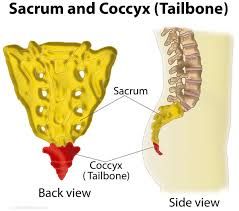
posterior bones |
|
|
Innominate bones AKA Iliac bones |
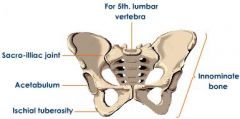
anterior & lateral to pelvic space (hip bones) |
|
|
False Pelvis |
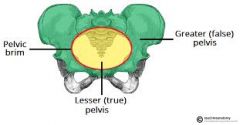
above plane - supports intestines |
|
|
True Pelvis |
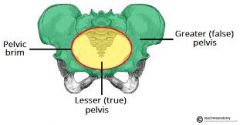
below plane |
|
|
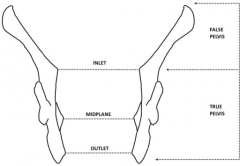
Pelvic Inlet vs. Outlet |
|
|
|
4 Types of Osseous (bony) Ligaments |
1. sacroiliac 2. sacrosciatic (sacrum, iliac, and coccyx) 3. sacrococceygeal 4. pubic |
|
|
4 Types of Suspensory (uterine) Ligaments |
1. cardinal 2. broad 3. sacro-uterine 4. round |
|
|
Cardinal ligament |
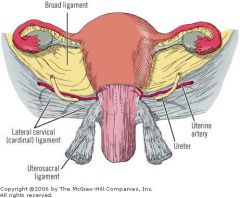
Primary support system for uterus - attaches superior & lateral from uterus - attaches inferior from vagina |
|
|
Broad ligament |
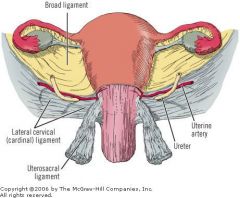
laterally from each side of uterus |
|
|
Sacro-uterine ligament |
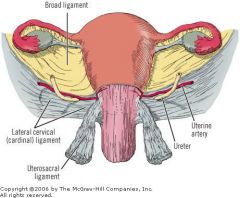
attaches uterus @ internal os to sacrum |
|
|
Round ligament |
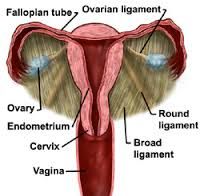
attaches uterine cornu to anterior pelvic wall |
|
|
3 False pelvis muscles |
1. rectus abdominis 2. psoas major 3. iliacus |
|
|
4 True pelvis muscles |
1. levator ani 2. coccygeous 3. obturator internus 4. piriformis |
|
|
Which False Pelvis muscle is a major cause of 'mirror-imaging artifact' in gravid patients? |
rectus abdominis |
|
|
Which False Pelvis Muscle has a 'bullseye' appearance in TRV? |
psoas major |
|
|
Primary purpose of the True Pelvis |
hold pelvic organs in place |
|
|
The levator ani and coccygeous muscles form the most caudal structure of the pelvic cavity, this is called what? |
Pelvic Diaphragm |
|
|
Which True Pelvis muscle forms the pelvic floor? |
Levator ani - which consists of the coccygeous muscles |
|
|
What is the True Pelvis triangular muscle that is located on the lateral pelvic wall? |
Obturator internus - inserts @ greater trochanter of femur |
|
|
Which True Pelvis muscle is found on the pelvic side wall? |
Piriformis - inserts @ greater trochanter of femur |
|
|
What does the Common Iliac Artery bifurcate into? |
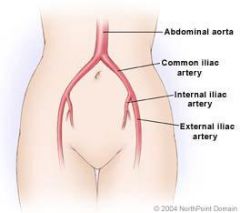
External (EIA) and Internal (IIA) Iliac Artery |
|
|
What is another name for the Internal Iliac Artery (IIA) |
Hypogastric artery |
|
|
What does the EIA feed? |
lower limbs |
|
|
What does the Hypogastric (IIA) feed? |
pelvic viscera, wall, perineum, and gluteal regions |
|
|
Explain the waveform of the EIA and the IIA |
high velocity high impedance flow (doesn't need constant BF) |
|
|
What does impedance flow mean? |
measures how much a structure resists motion |
|
|
What is the terminal branch of the Hypogastric Artery (IIA) ? |
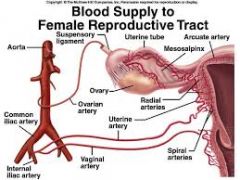
Uterine Artery |
|
|
Are the ureters, ovaries and fimbriae anterior or posterior to IIA? |
anterior |
|
|
Where are the Internal Iliac Veins compared to their arteries? |
Posterior |
|
|
Explain the waveform of the Uterine Artery |
high velocity high resistance |
|
|
Uterine plexus of veins (Venous plexus) compared to arteries |

much larger than corresponding arteries |
|
|
Where does the Ovarian Artery (gonadal) originate from? |
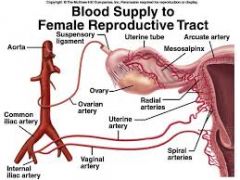
Abdominal Aorta |
|
|
What is the primary blood supply to the ovaries? |
Ovarian artery |
|
|
Explain the waveform of an Ovarian Artery |
before ovulation & Secretory - high systolic & diastolic, LOW resistance dormant ovary - low velocity, HIGH resistance |
|
|
Where do the Right and Left Ovarian/gonadal veins empty? |
right - Inferior Vena Cava (IVC) left - Left Renal Vein (LRV) |
|
|
What exists to ensure adequate blood flow if a vessel becomes obstructed? |
Collateral Pathways |
|
|
Urinary Bladder |
musculomembranous sac that serves as reservoir for urine |
|
|
Where do the Ureters insert into the bladder? |

inferior 3rd of posterior wall |
|
|
The superior aspect of the bladder has what shape? |
Dome |
|
|
3 Tissue Layers of bladder wall |
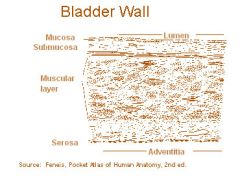
1. outer epithelial (skin) 2. middle muscularis 3. inner mucosal |
|
|
Sonographic appearance of bladder wall |

echogenic uniform thickness |
|
|
After the patient empties the bladder, which tissue layer is evaluated and what for? |
Mucosal layer for thickness (should be very thick) |
|
|
The Urethra does what? |
excretes urine |
|
|
Where does the Urethra arise? |

inferior mid portion of bladder |
|
|
Internal Urethral Sphincter |
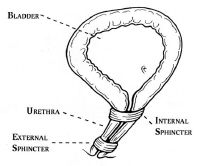
thickened area of bladder wall surrounding the urethra |
|
|
Ureters are how long? |
25-30cm |
|
|
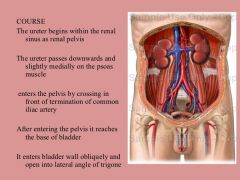
Why is the path of the Ureters important? |
Pathology in surrounding structures can cause problems in both bladder & kidneys |
|
|
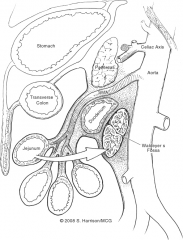
Ureter Pathway |
|
|
|
Course of Ureters within True Pelvis |
-anterior to IIA -posterior to ovaries -anterior & medial on inferior medial portion of broad ligament -anterior to lateral fornices of vagina |
|
|
How long is the Vagina? |
7-10cm |
|
|
Sonographic appearance of Vagina |
hypoechoic tubular structure with echogenic lumen (inside) |
|
|
What is the Vagina composed of? |
-smooth muscle -elastic connective tissue -squamous epithelium |
|
|
4 Fornices of the Vagina |
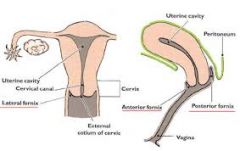
anterior lateral (2) posterior |
|
|
Which Vaginal Fornice is the most common site for free fluid? |
Posterior |
|
|
Which Vaginal fornices cause shadowing on TRV cervix image |
Lateral |
|
|
Where are the ovaries located in a Nulliparous person? |
ovarian Fossa AKA Fossa of Waldeyer |
|
|
The ovaries are suspended by what 3 ligaments? |
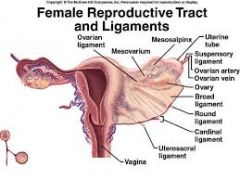
1. suspensory 2. ovarian 3. mesovarium |
|
|
Ovarian parenchyma contains numerous follicles that give rise to what? |
functional ovarian cysts AKA Follicular cysts |
|
|
What size are the ovaries pre-menarche? |
3.0cm3 |
|
|
What size are the ovaries post-menstrual? |
5.8cm3 |
|
|
The ovaries are largest in the pre-ovulatory phase and smallest in the...... |
luteal phase |
|
|
The Uterus is a muscular structure suspended by ligaments in the..... |
midline of true pelvis |
|
|
What is the most superior aspect of the Uterus? |
Fundus |
|
|
What is the body of the Uterus called? |
Corpus |
|
|
What is the area of the Uterus called between the body and the Cervix? |
Isthmus (Lower Uterine Segment) |
|
|
Cervix compared to Uterus |
- more fibrous - less muscular - 2-3cm long - less freely movable |
|
|
What factor is highly variable with the Uterus? |
position |
|
|
What is the Dual Blood Supply to the Uterus? |
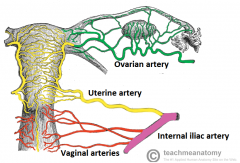
Uterine & Ovarian arteries |
|
|
The size of the Uterus is affected by what? |
Hormones |
|
|
Size of prepubescent Uterus |
2.8cm long 0.8 cm AP |
|
|
What happens to the size of the Uterus from birth to 4 years? |
decreases |
|
|
At what age does the Uterus start to grow? |
8 years |
|
|
Size of Uterus at Reproductive age? |
7cm long 4cm wide |
|
|
Size of the Uterus after multi-parity? |
8.5cm long 5.5cm wide |
|
|
Size of Uterus post-menopause? |
small 3.5-6.5cm long 1.2-1.8cm AP |
|
|
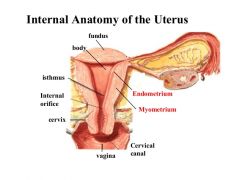
3 Uterine Layers |
1. serosa (parametrium) 2. muscularis (myometrium) 3. mucous (endometrium) |
|
|
Serosa (parametrium) |
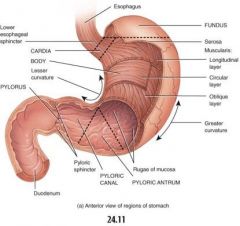
peritoneal covering of uterus - covers fundus and most of body |
|
|
3 layers of Muscularis / Myometrium and their sonographic appearance |
1. inner = hypoechoic "subendometrial halo" 2. middle = more echogenic 3. outer = may appear as cystic changes |
|
|
What is the innermost Uterine Layer? |
Mucous / Endometrium |
|
|
The Endometrium varies in thickness and echogenicity. What are some of the factors? |
phase of menstrual cycle parity age HRT (hormone replacement therapy) |
|
|
About how thick is the Endometrium just before menses? |
6mm |
|
|
About how thick is the Endometrium just after menses? |
1mm |
|
|
What should the Endometrium not exceed past in a premenopausal person? |
14-16mm |
|
|
What should the Endometrium not exceed past in a postmenopausal person? |
8mm |
|
|
Sonographic appearance of Endo during Early Proliferative Phase (day 5-9) |
thin echogenic line |
|
|
Sonographic appearance of Endo during Late Proliferative Phase (day 10-14) |
THICKENS due to ESTROGEN Hypoechoic compared to echogenic basal layer |
|
|
Sonographic appearance of Endo in the Secretory Phase (day 15-28) |
- thick & hyperechoic Endo - becomes isoechoic to basal layer |
|
|
What happens to the Functional Layer during the Secretory Phase? Why? |
becomes thickened, soft, and edematous (like a pillow) Because of PROGESTERONE |
|
|
What happens to the functional layer during the Late Proliferative Phase? Why? |
Thickens due to ESTROGEN |
|
|
What does Proliferate mean? |
Grow |
|
|
What are the normal Uterine Positional Variants? |
- version (anteversion) - flexion (anteflexion) |
|
|
Version |
relationship between cervix & vagina |
|
|
Flexion |
relationship between cervix & uterine body |
|
|
How is the Corpus usually flexed? |
anteriorly on cervix (anteflexion) |
|
|
Anteverted / Anteflexed |
corpus, fundus, and cervix in normal position |
|
|
Retroverted |
corpus/fundus normal cervix tilted backwards on vagina |
|
|
Retroflexed |
corpus/fundus tilted backwards cervix normal |
|
|
Retroverted & Retroflexed |
corpus, fundus, and cervix ALL tilt backwards |
|
|
Sonographic evaluation of Retroversion |
EXTREMELY limited (sound beam isn't hitting correct structures) |
|
|
2 ways to differentiate between fundal fibroid & dropout artifact.... |
- lack of displacement of endo - lack of contour abnormality |
|
|
Retroversion is a normal variant until when? |
14-16wk gestation |
|
|
Incarcerated Uterus |
fundus fails to rise into false pelvis from sacral hollow during pregnancy (uterus is stuck in sacral hollow) |
|
|
S/S of Incarcerated Uterus |
- UTI - severe pelvic pain - multiple ER visits between 13-17wks |
|
|
3 Sonographic groupings of findings for Incarcerated Uterus |
1. pregnancy very deep in cul-de-sac 2. maternal bladder ANTERIOR to uterus (should be inferior) 3. cervix visualized between bladder and pregnancy |
|
|
Differential Diagnosis for Incarcerated Uterus |
ectopic or abdominal pregnancy (ALWAYS make sure pregnancy is INTRAUTERINE) |
|
|
Complications if Incarcerated Uterus is NOT diagnosed |
- spontaneous abortions - uterine rupture (can be fatal) |
|
|
Treatment if Incarcerated Uterus is diagnosed early |
manual reposition of uterus |
|
|
Fallopian tubes extend.... |
laterally from cornu to ovaries |
|
|
How long are average Fallopian Tubes? |
10cm |
|
|
Where are the Fallopian Tubes located? |
in superior portion of broad ligament |
|
|
What is the narrowest portion of the Fallopian Tubes that travels through the cornu? |
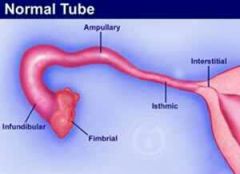
Intramural / Interstitial |
|
|
What is the longest portion of the Fallopian Tubes? |
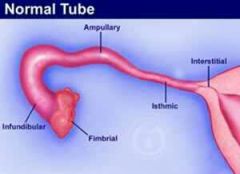
Isthmic
|
|
|
Fimbriated portion of Fallopian tubes |
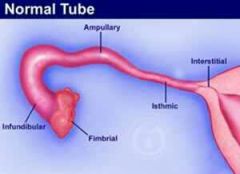
open portion of tube adjacent to ovary |
|
|
Fimbria |
surround ovary and capture ovum |
|
|
Osteum |
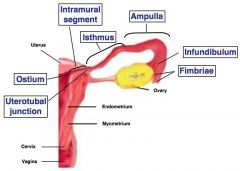
open end into peritoneal cavity (chute) |
|
|
Infundibulum |
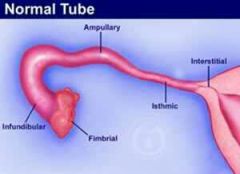
inner, funnel-shaped cavity of ampullary portion |
|
|
Why is the infundibulum funnel-shaped? |
increased likelihood that ovum will go in |