![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
128 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
Adhesive Capsulitis Stages |
1. Pre-freezing 2. Feezing 3.Frozen 4. Thawing |
|
|
|
Pre-Freezing |
Gradual onset
Strength is maintained > 3 months |
|
|
|
Freezing |
Intensive pain even at rest Limited ROM 3-9 months |
|
|
|
Frozen |
Pain only with movement Significant adhesions Limited motion with scapular compensation Atrophy of deltoid, rotator cuff, bicep, tricep 9-15 months |
|
|
|
Thawing |
No pain or synovitis Significant capsular restrictions from adhesions 15-24 Months May never regain full ROM and may go under anesthetic manipulation |
|
|
|
Achilles Tendon Rupture |
Occurs 1-2 inches above the calcaneus Usually caused by pushing off a weight bearing extended knee, unexpected dorsiflexion, or forceful eccentric contraction of PF Sports that require quick changing foot work Commonly between 30-50 years old |
|
|
|
Achilles Tendon Rupture Signs and Symptoms |
Swelling over distal tendon Palpable defect above calcaneal tuberosity Pain and weakness with PF Will report hearing a snap or pop at time of injury Present with positive Thompson Test Unable to stand on toes
|
|
|
|
Thompson test |
Patient is prone, squeeze calf and ask patient to PF. Positive is the absence of passive plantar flexion |
|
|
|
Ankylosing Spondylitis |
Systemic condition characterized by inflammation of the spine and larger peripheral joints that causes destruction of the ligamentous-osseous junction with subsequent fibrosis and ossification of the area |
|
|
|
Anklyosing Spondylitis Clinical Presentation |
Recurrent and insidious episodes of LBP Morning Stiffness Impaired spinal extension Hip flexion contractures Decreased lumbar lordosis Kyphosis Fatigue Weight loss Impaired chest mobility |
|
|
|
Anklyosing Spondylitis PT Treatment |
Reduce Inflammation Maintain ROM Postural exercises Low impact exercises with emphasis on extension and rotation Aquatic Therapy |
|
|
|
NSAIDS |
Non steroidal anti-inflammatory drugs Blocks prostiglandin Prostiglandin protects the stomach lining from acid which can be an issue when taking NSAIDS long term Can cause ulcers, GI bleeding/upset, & increased risk of heart attack |
|
|
|
Asprin |
Unique NSAID that is a blood thinner |
|
|
|
NSAID + Hypertensive meds reaction |
NSAIDS may increase blood pressure which could cancel out the effects of hypertensive meds |
|
|
|
MMT Grade 0/5 (Zero) |
No contraction noted Flaccid Almost always neurological problem |
|
|
|
MMT Grad 1/5 (Trace) |
Muscle twitch/spasm is palpable |
|
|
|
MMT -2/5 |
Only able to move through less than 100% of ROM With gravity eliminated |
|
|
|
MMT 2/5 (Poor) |
Able to move through through 100% of ROM With gravity eliminated |
|
|
|
MMT +2/5 (Poor+) |
Only able to move through less than 50% of ROM Against gravity |
|
|
|
MMT -3/5 |
Able to move through more than 50% but less than 100% of ROM Against gravity |
|
|
|
MMT 3/5 (Fair) |
Able to move through 100% of ROM Against gravity but no manual resistance |
|
|
|
MMT +3/5 (Fair +) |
Able to move through 100% of ROM against gravity and minimal resistance |
|
|
|
MMT -4,4,+4/5 (Good) |
Able to move through 100% of ROM with variable degrees of resistance but patient cannot tolerate maximal resistance
|
|
|
|
MM 5/5 (Normal) |
100% of ROM without breaking against maximal resistance |
|
|
|
Lateral bending gait: prosthetic causes |
Prostheses to short Improperly shaped lateral wall High medial wall Prosthesis aligned in abduction |
|
|
|
Lateral bending gait: amputee causes |
Poor balance Abduction contracture Improper training Short residual limb Weak hip abductors Hypersensitive/painful residual limb |
|
|
|
Abducted Gait: Prosthetic causes |
Prosthesis to short High medial wall Poorly shaped lateral wall Prosthesis positioned in abduction Inadequate suspension Excessive knee friction |
|
|
|
Abducted gait: Amputee causes |
Abduction contracture Improper training Adductor roll Weak hip flexor Pain over lateral residual limb |
|
|
|
Cicumduction Gait: Prosthetic causes |
Prosthesis to long Too much knee friction Socket to small Excessive plantar flexion of prosthetic foot |
|
|
|
Circumduction Gait: Amputee causes |
Abduction contracture Improper training Weak Hip flexor Lack of confidence to flex the knee Painful anterior distal limb Inability to initiate prosthetic knee flexion |
|
|
|
Excessive knee flexion in stance: Prosthetic causes |
Socket set forward (in relation to foot) Foot set in excessive dorsi-flexion Stiff heal Prosthesis to long |
|
|
|
Excessive knee flexion in stance: Amputee causes |
Knee flexion contracture Hip flexion contracture Pain in anterior limb Decreased quadriceps strength |
|
|
|
Vaulting gait: Prosthetic causes |
Prosthesis to long Inadequate socket suspension Excessive alignment stability Foot in excessive plantar flexion |
|
|
|
Vaulting Gait: Amputee causes |
Limb discomfort Improper training Fear of catching toe Short limb Painful/limb |
|
|
|
Rotation of foot at heel strike: Prosthetic causes |
Excessive built in toe out loose fitting socket Inadequate suspension Rigid SACH heel cushion |
|
|
|
Rotation of foot at heel strike: Amputee causes
|
Poor muscle control Improper training Weak medial rotators Short limb |
|
|
|
Forward Trunk flexion gait: Prosthetic causes |
Socket to long Poor suspension Knee instability |
|
|
|
Forward Trunk flexion gait: Amputee causes
|
Hip flexion contracture Weak hip extension Pain with ischial weight bearing Inability to initiate prosthetic knee flexion |
|
|
|
Medial or lateral whip gait: Prosthetic causes |
Excessive rotation of the knee Tight socket fit Valgus in the prosthetic knee Improper alignment of toe break |
|
|
|
Medial or lateral whip gait: Amputee causes
|
Improper training Weak hip rotators Knee instability |
|
|
|
Capillary refill time Normal vs abnormal |
Normal=<2 seconds Abnormal=>2seconds |
|
|
|
Brown-Sequard syndrome |
Lesion on one entire side of spinal cord Same side weakness, and dorsal column deficits Opposite side spinothalamic deficits |
Usually caused by a knife stab |
|
|
Anterior cord syndrome |
Damage to anterior portion of spinal cord usually caused by compression during cervical hyperflexion B motor and spinothalamic deficits but dorsal tracts intact |
|
|
|
Posterior cord syndrome |
Compression of posterior cord, rare Motor function and spinothalamic preserved Dorsal column deficits |
These people have a wide based gait pattern and rely heavily on vision for balance |
|
|
Central cord syndrome |
Damage to central cord usually caused by cervical hyperextension B corticospinal, spinothalamic, and dorsal column damaged Motor deficits > sensory deficits UE's > LE |
|
|
|
Cuada Equina lesions |
Below L1 Peripheral nerve or LMN injury not central Usually incomplete unilateral symptoms Nerves can slowly regenerate |
|
|
|
C1-C3 SCI |
Can: talk, chew, sip & blow Dependent and on ventilator Sip & puff power wheelchair |
|
|
|
C4 |
Has diaphragm & upper trap now Can breathe on own and elevate scapula No ventilator needed Still sip & puff power wheelchair |
|
|
|
C5 |
Can flex and supinate elbow, shoulder ER, Abd, and some flexion Not dependent in ADLs but does need assistance Independent in manual w/c with projections or power w/c with joy stick Van with hand controls |
|
|
|
C6 |
Has all shoulder motion, pronation, wrist extension (Tenodesis grasp) |
|
|
|
C7 |
Has all shoulder/elbow, wrist motion. Has finger extension but not flexion Independent in ADLs and transfers Able to get w/c in and out of car Manual w/c without projections but with friction hand rims |
|
|
|
C8 to T1 |
Has all shoulder, wrist, elbow, finger motion Able to RTW without structural barriers Manual w/c with standard hand rims |
|
|
|
T4-T6 |
Improved trunk control, respiration, and perctoral girdle stability Physiological standing with B KAFOs with spinal attachment |
|
|
|
T9-T12 |
More trunk endurance Household ambulation with B KAFOs and B crutches |
|
|
|
L-L3 |
Functional ambulation B KAFOs and B crutches Has hip flexion and adduction, and knee extension |
|
|
|
L4-L5 |
Has strong hip flexion, strong knee extension, weak knee flexion, low back muscles Functional ambulation B KAFOs and B crutches or canes. |
|
|
|
Moro |
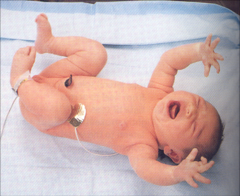
28 weeks to 5 months Stimulus: head drops into extension Response: Arms abduct with fingers open followed by crossing trunk into adduction and crying |
Abnormal persistence interferes with: Balance reactions when sitting Protective responses in sitting Eye hand coordination |
|
|
Root |

28 weeks to 3 months Stimulus: touch cheek Response: turning head to same side with mouth open |
Abnormal persistence interferes with: Oral motor development Development of mid line Control of the head Optical righting, visual tracking Social interaction, attention |
|
|
Palmer Grasp |

Birth to 4 months Stimulus: Pressure in palm on ulnar side of hand Response: Flex of fingers causing strong grip |
Abnormalpersistence interferes with: Ability to grasp & release objects voluntarily Weight bearing on open hand for propping, crawling, & protective response |
|
|
Stepping |
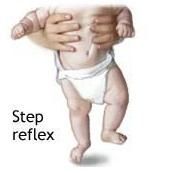
38 weeks to 2 months Stimulus: Supported upright position on soles of feet on firm surface Response: Reciprocal flex/ext of legs |
Abnormal persistenceinterferes with: Standing & walking Balance reactions & weight shifting in standing Development of smooth coordinated reciprocal movement of LEs |
|
|
Plantar Grasp |
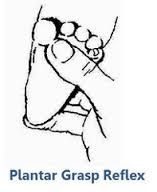
28 weeks to 9 months Stimulus: Pressure at base of toes Response: Toe flexion |
Abnormal persistence interferes with: Ability to stand with feet flat Balance reactions & weight shifting in standing |
|
|
Babinski Reflex |

Birth to 18/24 months Stimulus: Run object from heel to base of toes Response: Extension of the big toe and fanning of toes |
Abnormal persistence interferes with: Ability to stand with feet flat on surface Causes- Coordination & weakness in motor control (UMN lesion) |
|
|
Galant Reflex |

30 weeks to 2 months Stimulus: Touch skin along spine from shoulder to hip Response: Lateral flexion of trunk to side of stimulus |
Abnormal persistence interferes with: Development of sitting balance Can lead to scoliosis |
|
|
Asymmetric Tonic Neck Reflex (ATNK) |
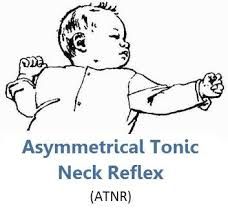
Birth to 6 months Stimulus: Turn head to one side Response: Extension of arm & leg toward same direction of turn. Flexion of arm & leg on opposite side of turn. Spine curved with convexity towards face side. |
Abnormal persistence interferes with: Feeding Visual tracking Development of crawling Can lead to scoliosis, hip subluxations, etc. |
|
|
Symmetrical Tonic Neck Reflex |

6-8 months Stimulus: Head positioned either in flexion or extension Response: When head is flexed arms & legs are flexed. When head is extended, arms & legs are extended |
Abnormal persistence interferes with: Ability prop on arms in prone Attain & maintain hands and knee position Crawling reciprocally Sitting balance when looking around Use of hands when looking at object in hands while seated |
|
|
Angle of torsion |
Between shaft and neck of femur in transverse plane Normal: 15-25 degrees |
|
|
|
Anteversion |
Increased angle of torsion Causes toe in/genu valgus |
|
|
|
Retroversion |
Decreased angle of torsion Causes toe out |
|
|
|
5 Major Subdivisions of the Brain (embryonic development) |
1. Telencephalon = Cerebral Hemispheres 2. Diencephalon = thalamus & hypothalamus 3. Mesencephalon = midbrain 4. Metencephalon = pons & cerebellum 5. Myelencephalon = medulla oblongata |
|
|
|
Some main Front lobe functions |
1. Motor Movement 2. Expresive speech 3. Personality characteristics 4. Intellectual function 5. Reasoning 6. Abstract thinking 7. Olfaction 8. Aggression 9. Sexual behavior |
9 total |
|
|
Some main functions of the Occipital Lobe |
1. Vision 2. Recognition of size, shape, & color |
4 total |
|
|
Some main functions of the Parietal lobe |
1. Control gross sensation 2. Control fine sensation 3. Contains the postcentral gyrus which is responsible for sensation |
3 total |
|
|
Some main functions of the Temporal lobe |
1. Interpretation of language 2. Discrimination of sound and speech 3. Memory processing centers |
3 total |
|
|
What cranial nerves are located in the midbrain |
Center for visual reflexes so, CN 3 & 4 |
|
|
|
What cranial nerves are located in the pons |
CN 5,6,&7 |
|
|
|
What is the function of the medulla |
Center for automatic control of respiration and hear rate |
|
|
|
What is the function of the cerebellum |
Control muscle control, tone & posture |
|
|
|
What is CN 1 & what would present when damaged |
Olfactory anosmia (loss of sense of smell) |
|
|
|
What is CN 2 & what would present if damaged |
Optic Monocular blindness Loss of pupillary constriction Absence of blink reflex |
|
|
|
What is CN 3 & what would present if damaged |
Occulomotor Ptosis (dropping eye lid) Dilation of pupil |
|
|
|
What is CN 4 & what would present if damaged |
Trochlear Diplopia (double vision) Failure to rotate eye up & out |
|
|
|
What is CN 5 & what would present if damaged |
Trigeminal Loss of facial sensation Weakness in muscles of mastication Jaw deviation to ipsilateral side |
|
|
|
What is CN 6 & what would present if damaged |
Abducens Diplopia Inability to look to the side |
|
|
|
What is CN 7 & what would present if damaged |
Facial
Ipsilateral face paralysis Dry mouth Loss of taste anterior 2/3 of tongue Bell's Palsy |
|
|
|
What is CN 8 & what would present if damaged |
Vestibulocochlear Vertigo Nystagmus Disequilibrium Tinnitus Loss of hearing |
|
|
|
What is CN 9 & what would present if damaged |
Glossopharyngeal Slight dysphagia Partial dry mouth Loss of taste on posterior 1/3 of tongue |
|
|
|
What is CN 10 & what would present if damaged |
Vagus Palpitations tachycardia vomiting slowing of respiration ipsilateral paralysis of soft palate & larynx Hoarseness |
|
|
|
What is CN 11 & what would present if damaged |
Accessory Phonation Weakness if shrugging ipsilateral shoulder & turning head to contralateral side |
|
|
|
What is CN 12 & what would present if damaged |
Hypoglossal Unilateral paralysis of the tongue Deviation to ipsilateral side with protrusion |
|
|
|
What are the 5 terminal branches of the Brachial plexus and spinal levels? |
1. Axillary C5-6 2. Musculocutaneous C5-6 3. Radial C6-T1 4. Median C6-T1 5. Ulnar C8-T1 |
|
|
|
What are the 5 terminal branches of the Lumbosacral plexus and spinal levels? |
1. Femoral L2-4 2. Obturator L2-4 3. Sciatic L4-S3 4. Tibial L4-S3 5. Peroneal L4-S2 |
|
|
|
What are the functions of the Clavicle?(3) |
1.Acts to hold the upper limb free from trunk to allow freedom of movement 2. Attaches upper limb to axial skeleton 3. Transmits forces from upper limb to axial skeleton |
|
|
|
What is the function of the Coracoclavicular ligament? |
Prevents upward dislocation of humeral head |
|
|
|
What is the scapular to humeral ratio for elevation? |
1:1 30°-90° 2:1 90°-180° |
|
|
|
What degrees of elevation happens at the Glenohumeral joint? |
120° |
|
|
|
What degrees of elevation happen at the Scapulothoracic joint? |
60° |
|
|
|
What muscles produce upward rotation of the shoulder?(2) |
Trapezius Serratus Anterior |
|
|
|
What muscles produce downward rotation of the shoulder?(3) |
Rhomboids Levator Scapula Pectoralis Minor |
|
|
|
What muscles produce scapular protraction?(2) |
Serratus Anterior Pectoralis Minor |
|
|
|
What muscles produce scapular retraction? (3) |
Rhomboids Middle Trapezius Lower Trapezius |
|
|
|
What muscles produce scapular elevation? (3) |
Upper Trapezius Levator Scapula Rhomboid Major |
|
|
|
What muscles produce scapular depression? (2) |
Latissimus Dorsi Pectoralis Minor Lower Trapezius |
|
|
|
What is Crutch palsy? |
Compression of the radial nerve from crutches in axila |
|
|
|
Open pack for Glenohumeral joint |
55° Abd, 30° H/Add. |
|
|
|
Open pack for Ulnohumeral joint |
70°flexion, 10° supination |
|
|
|
Open pack for Radiohumeral joint |
full extension and supination |
|
|
|
Open pack for Proximal Radioulnar joint |
70°flexion. 35° supination |
|
|
|
Open pack for Distal Radioulnar joint |
10° supination |
|
|
|
Open pack for Radiocarpal joint (wrist) |
Neutral with slight ulnar deviation |
|
|
|
Open pack for Iliofemoral joint (hip) |
30° flexion, 30° Abd, slight ER |
|
|
|
Open pack for Tibiofemoral (knee) |
25° flexion |
|
|
|
Open pack for Talocrural joint (ankle) |
10° PF, and neutral |
|
|
|
Closed pack for Glenohumeral joint |
Abd, ER |
|
|
|
Closed pack for Ulnohumeral joint |
Extension |
|
|
|
Closed pack for Radiohumeral joint |
90° flexion, 5° supination |
|
|
|
Closed pack for proximal & distal Radioulnar joint |
5° supination |
|
|
|
Closed pack for Radiocarpal joint (wrist) |
Extension with radial deviation |
|
|
|
Closed pack for iliofemoral joint (hip) |
Full extension & IR |
|
|
|
Closed pack for Tibofemoral joint (knee) |
Full extension & ER of tibia |
|
|
|
Closed pack for Talocrural joing (ankle) |
Max DF |
|
|
|
Closed pack for Subtalar joint |
Supination |
|
|
|
Capsular pattern for Glenohumeral joint |
ER>ABD>IR |
|
|
|
Capsular pattern for Ulnohumeral joint |
Flexion>Extension |
|
|
|
Capsular patern for Radiohumeral joint |
Flexion, Extension, Supination & Pronation |
|
|
|
Capsular pattern for Proximal Radioulnar |
Pronation=Supination |
|
|
|
Capsular pattern for Radiocarpal joint (wrist) |
Flexion=Extension |
|
|
|
Capsular pattern for Iliofemoral joint (hip) |
IR>Flexion>Abd |
|
|
|
Capsular pattern for Tibiofemoral joint (knee) |
Flexion>Extension |
|