![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
42 Cards in this Set
- Front
- Back
|
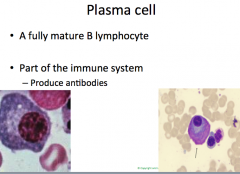
Review: what is a plasma cell |
|
|
|
review: hematopoietic stem cell cascade |

|
|

|
d |
|
|
Antibody production: relative proportions of IgG, IgM, IgD, IgA |

|
|
|
detection modalities for antibodies |
|
|
|
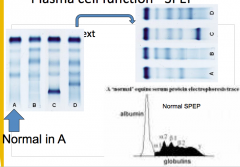
example of serum protein electrophoresis interpretation |
|
|
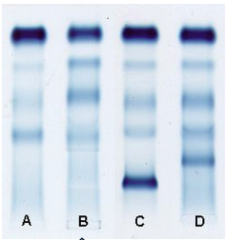
what is going on in B |
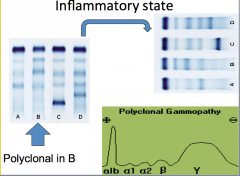
this can be caused by infection, sepsis, inflammatory condition, or malignancy causing inflammation "polyclonal gammopathy" |
|
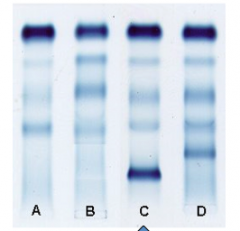
what is happening in C |
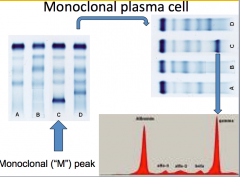
Monoclonal M peak |
|
|
NB: do NOT confuse monoclonal vs. polyclonal picture. !! |
OK |
|
|
what are potential causes of polyclonal gammopathy |
infection inflammation liver disease |
|
|
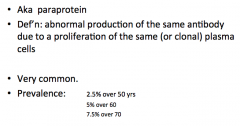
Def'n of monoclonal protein/paraprotein prevalence |
|
|
|
Spectrum of primary plasma cell disease? 4 |
|
|
|
conceptual organization of primary plasma cell disease |
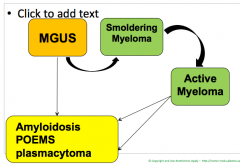
MGUSis baseline condition. POEM: polyneuropathy, organomegaly, endocrinopathy and M something.. With skin changes andsclerotic bone changes. Should know MGUS and multiplemyeloma |
|
|
MGUS 1j. prevalence 2. benign 3. risk of transformation? |
|
|
|
MGUS: 1% baseline risk of transformation. but.. what are some high risk features? 3 |
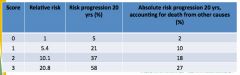
1. Non-IgG M protein 2. M protein > 15 g/L (smoldering) 3. abnormal free light chain ratio presence or absence of these features helps us time our follow up testing |
|
|
how is MGUS different from multiple myeloma |
|
|
|
Paraprotein end damage in MM what is the mnemonic you need to know? |
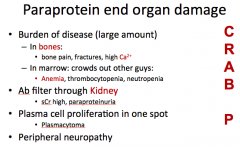
more like CRAB PP |
|
|
Urine microscopy finding in MM |
bence jones protein |
|
|
why does MM lead to anemia and not pancytopenia |
Myeloma cell crowding: doesn’t leadto pancytopenia like acute leukemia. Leads to anemia, often present when firstdiagnosed with multiple myeloma. |
|
|
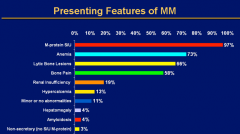
Presenting features of MM |
|
|
|
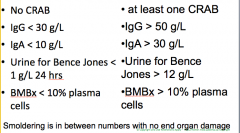
for exam purposes: def'n of MGUS vs. MM 1. CRAB/no CRAB 2. IgG level 3. IgA level 4. Bence Jones 5. Bone Marrow Biopsy findings |
|
|
|
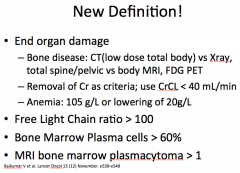
for interest, there is a new definition |
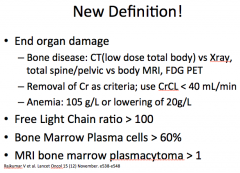
CRAB 123 ra ra ra!! |
|
|
what are investigations to do in MGUS |
|
|
|
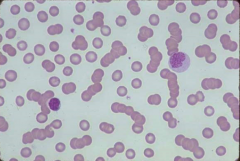
rouleaux ≠ agglutination |
|
|
|
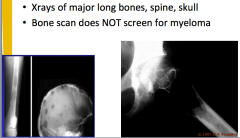
Skeletal survey: what are the components |
|
|
|
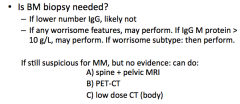
when to do a bone biopsy in MGUS? |
|
|
|
note: if still suspicious for MM, but no evidence, 3 tests you can do |
1. spine + pelvic MRI 2. PET-CT 3. Low dose CT body |
|
|
Staging of MM |
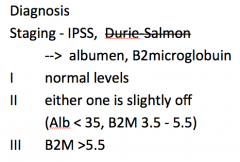
IPSS = international prognostic scoring system |
|
|
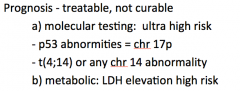
Prognosis of MM 1. tests to determine high risk disease (molecular and metabolic) |
|
|
|
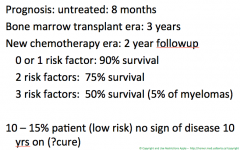
Prognosis of MM 1. prognosis untreated 2. bone marrow transplant 3. new chemotherapy 4. cure? |
|
|
|
Principles of therapy 1. intent of therapy 2. 5 treatment modalities |
|
|
|
"cellular treatment" of MM 2 modalities, 2 subtypes |
|
|
|
how to decide between autologous vs. analogous |
age, co morbidities.. I think younger patients typically receive allogeneic..? |
|
|
chemo agents that can be prescribed in MM? these change rapidly so DNM |
|
|
|
if patient is candidate, can give chemotherapy + cellular transplant note the benefit conferred by this tx.. |
|
|
|
MM: when to use RT/surgery? |
bone disease and SPINAL CORD COMPRESSION eg fractures, plasmacytoma, painful lytic lesion |
|
|
kyphoplasty |
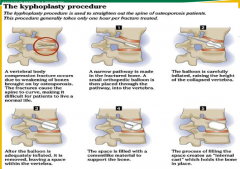
reinflation of a compression fracture in vertebral body, filled with cement |
|
|
complications of myeloma: hyperviscosity
1. pathophysiology 2. clinical presentation |
|
|
|
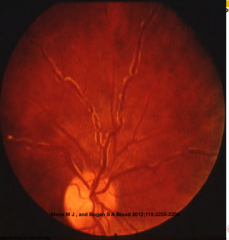
Funduscopic appearance of patient with WM andmixed cryoglobulinemia. Note the marked retinal venousengorgement and “sausaging.” The white material at the edgeof the veins may be cryoglobulin. IgM and cryoglobulin problem.. Little sausage like links alongvessels. Vessels thicken.. What an IgMhyperviscositylooks like on fundoscopy. |
|
|
Myeloma complications: immune dysfunction: 1. pathophys 2. clinical presentation |
immune dysfunction: 1. cause: hypogammaglobinemia (tx to replace with IVIg 2. present with recurrent infection |
|
|
MM complications: amyloid |
Wiki.. Amyloidosis is a rare disease that results from accumulation of inappropriately folded proteins. These misfolded proteins are called amyloids. When proteins that are normally soluble in water fold to become amyloids, they become insoluble and deposit in organs or tissues, disrupting normal function.[2][3] The type of protein that is misfolded and the organ or tissue in which the misfolded proteins are deposited determines the clinical manifestations of amyloidosis. |
|
|
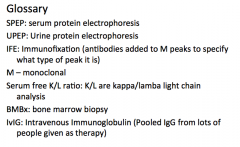
term glossary |
|