Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
64 Cards in this Set
- Front
- Back
|
What are the predisposing factors to caries history?
|
diet
fluid consumption oral hygiene habits level of undersanding and motivation drug therapy impacting on salivary flow mouth breathing |
|
|
What are the requirements for good clinical examination?
|
good light
dry field sharp probe |
|
|
What visual signs do u look for in pits and fissure caries?
|
retentive surface
dark staining white enamel |
|
|
What do u look for in approximal caries?
|
if non-cavitated: shadowing and white caries
cavitated which can affect only the dentine or including the pulp shadowing and reserse caries |
|
|
What are the visual features of cervical margin caries?
|
whitespot/non cavitated
cavitated - involving dentine or extensive |
|
|
What visual signs to look for in root caries
|
Occurs subgingivally
May occur in conjunction with abfraction lesions |
|
|
what are abfraction lesions?
|
Abfraction lesions are small cracks or notches in your teeth caused by chewing.
|
|
|
What are Class 1 to 5 mean?
|
1: pits and fissure
2: posterior approximal 3. anterior approximal 4: anterior approximal with incisal edge 5: smooth surface |
|
|
What are Mount and Hume classification?
|
Two numbers: First is site and second is size
|
|
|
The three sites in Mount and Hume (MI) are?
|
1. pits and fissures
2. approximal surfaces 3. cervical areas |
|
|
The size classification in MI is?
|
Size 0: small and early enough to be remineralised (no restoration necessary)
Size 1: minimal dentinal spread (just beyond size 0) Size 2: Moderate involvement of dentine Size 3: enlarged with weakened cusps or incisal edges Size 4: extensive loss of tooth structure |
|
|
What is 2.3 on tooth 12 mean? (MI)
|
Caries on approximal surface moderate involvement of dentine
|
|
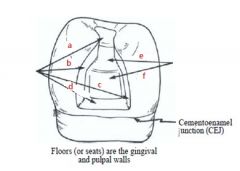
Label
|
a. Distal
b. facial c. lingual d. gingival e. pulpal f. axial |
|
|
What is Carvosurface margin?
|
Junction(ridge) between the external wall and the prepared wall
|
|
|
Carvosurface angle
|
Angle formed by the junction of a prepared wall and the external surface of the tooth
|
|
|
Enamel Wall
|
The enamel wall is that portion of a prepared external wall consisting of enamel
|
|
|
Dentinal Wall
|
The dentinal wall is that portion of a prepared external wall consisting of dentin, in which mechanical retention features may be located
|
|
|
What are the aims of cavity design?
|
remove caries
restore aesthetics and function |
|
|
What are the steps involved in cavity design?
|
Figure out access
Outline form Resistance form Retention form Convenience form Removal of carious dentine Cavity debridement |
|
|
What are the factors involved in access?
|
conservative, aesthetically acceptable, direct to caries, simple route to the dentine
|
|
|
What are Outline Form Factors?
|
Anatomy of tooth surface
Extent of peripheral caries Removal of fractured and unsupported enamel Conservation of tooth structure |
|
|
What is resistance form? What are the determining factors?
|
Form of preparation to resist fracture of tooth.
Flat pulpal floor Smooth outline Cap weak cusps Adequate bulk restorative material |
|
|
What is retention form?
|
Preparation form for mechanical retention. Eg. Amalgam
|
|
|
What is convenience form?
|
Suitable size and shape to enable proper placement of restoration
This compromises conservation of tooth structure |
|
|
Summarise Clinical Steps in Restoring a Tooth
|
Establish the required outline at minimum depth
Satisfy retention, resistance, convenience form requirements Remove deeper caries Complete cavity Pulp therapy, lining, seal tubules as required Apply matrix Bonding procedures Restoration placement |
|
|
What are the factors for the preparation?
|
Carious lesion extension, tooth morphology and function
|
|
|
What is the maximum increment depth for composite restoration?
|
2mm
|
|
|
Define C factor
|
C factor= (Bonded surface)/(Unbonded surface)
|
|
|
Class I would have C Factor of what?
|
5/1 = 5
|
|
|
What are the contraindications of composite restoration?
|
Tooth is under heavy occlusal stress
Tooth cannot be isolated Patient is allergic or sensitive to composite |
|
|
What are preoperative procedures of composite restoration?
|
Clinical and radiographic examination
Plaque removal Shade selection Occlusal analysis |
|
|
When polishing composite what is the order of colours to use?
|
yellow
grey white |
|
|
How do u check the occlusion?
|
using articulating paper
|
|
|
What does it mean by MI 2.2-4?
|
proximal caries with moderate (involving dentine) to extensive caries lesion
|
|
|
What are the advantages of composite restoration?
|
aesthetics
more conservative restorations biocompatible durable predictable |
|
|
What are the preoperative procedures for composite restoration?
|
radiographic examination
plaque removal shade selection occlusal analysis |
|
|
Should you bevel in posterior preparation?
|
no. it increases restoration size occlusally and proximally
jeopardizes enamel at cavosurface margin |
|
|
What is the ideal carvosurface angle in posterior prep?
|
larger than 90 degrees
|
|
|
Incorrect placement of matrix would result in what?
|
overhanging
incorrect proximal contouring inadequate contact point under or overfilling the retorative material |
|
|
when is beveling acceptable?
|
for anterior surface restorations eg Class III, IV, and V
Where there are enough enamel support |
|
|
what are sub classification of cutting hand instruments?
|
chisels and excavators
|
|
|
give example of a chisel and a excavator
|
chisel: gingival margin trimmer
excavator: spoon excavator |
|
|
give advantages of rubber dam usage
|
soft tissue protection
prevention of inhaling or swallowing protect from chemicals isolation |
|
|
what are the usage of high speed hp?
|
removing previous restoration
creating outline form initial caries removal |
|
|
when do u use low speed hp?
|
refine cavity, remove caries, polish
|
|
|
which bur to use for removing amalgam?
|
tungsten carbide bur
|
|
|
With tactile examination, how does cavitated enamel lesion feel?
|
chalky
|
|
|
Classify the criteria for radiographic criteria for caries diagnosis
|
1 incipient: < half way thru enamel
2 moderate: > half way thru enamel 3 advanced: <half way thru dentine 4 severe: > half way thru dentine |
|
|
when to use fissure sealant?
|
at risk patient
poor oral hygiene inappropriate diet poorly motivated parent/patient disabled patient |
|
|
Which tooth can be applied with fissure sealants?
|
upper and lower molars
|
|
|
what medical conditions for fissure sealants?
|
xerostima
mouth breather mental disability existing caries Sjogrens syndrome |
|
|
Do u use fissure sealants on 8 year old with dark stained molars?
|
no. it's arrested caries.
not needed |
|
|
what are non invasive method of diagnosis?
|
vision
probing trans illumination bitewing radiograph laser fluorescence |
|
|
what are invasive methods of caries diagnosis?
|
enamel biopsy
air abrasion |
|
|
If the fissure is sound then do u apply fissure sealant?
|
no, but monitor 6 monthly
|
|
|
When to apply sealants only?
|
when patient is in a low risk group
less than two other caries in a well maintained mouth take BW radiograph to eliminate possibility of occult caries |
|
|
When to use compostie and fissure sealant?
|
decalicified fissure on high risk group
enamel biopsy is indicated |
|
|
When to use GIC and sealant?
|
Enamel biopsy shows caries extends just into denine
minimal lateral spread |
|
|
Features of resin sealants?
|
flowable (low viscosity)
release fluoride better retention rates |
|
|
What are the prepartion for resin sealant?
|
pumice / water slurry with rubber prophy cup
then wash thoroughly then etch with 35% phosphoric acid for 15 seconds and wash |
|
|
what is the extent of etching areas?
|
beyond the fissures so that all enamel surfaces are sealed
|
|
|
what is the maximum and minimum time for etching?
|
15 minimum
60 maximum |
|
|
what is involved in prep for GIC sealants?
|
isolation
use conditioner rather than etchant 20% poly acrylic acid |
|
|
what is the purpose of using conditioner for GIC prep?
|
removes smear layer
|