Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
117 Cards in this Set
- Front
- Back
|
1. What are the 7 steps of palpatory Dx and Tx of viscera?
|
1. General Listening
2. Manual Thermal Diagnosis of visceral dysfunction 3. Fascial (local) listening 4. Layer palpation to level of organ 5. Motion testing in various planes (restrictions and directions of ease) 6. BLT 7. Re-assess |
|
|
2. BLT for the viscera?
|
Find the balance point(s) in all planes of motion for the dysfunctional organ
Hold it until it releases Re-assess |
|
|
3. Levels of viscerosomatic reflexes
|
T5-6R - upper esophagus
T6-9R - liver and gall bladder T8-9B - small intestine T5-9L - lower esophagus and stomach T6-9L - spleen and pancreas |
|
|
4. What is fascia?
|
“Fascia directly or indirectly influences the health of the body through coordination with the musculoskeletal system, cooperation in circulating body fluids, and by allowing generous passageway for nerves. Derangement in the fascial planes can result in venous congestion, abnormal reflexes, and a decreased range of motion. Thus myofascial techniques are crucial in eliminating fascial restrictions and allowing the body to return to a healthier state.”
|
|
|
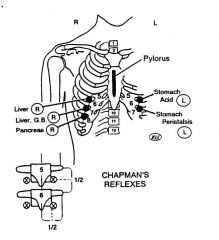
5. Chapman's points
|
|
|
|
6. What is true visceral pain?
|
This is early pain from irritation, stretching, contraction or exaggerated physiologic motor activity and dysfunction. It is midline pain, poorly localized-vague, deep, diffuse, burning ache.
• pacinian corpuscles • free nerve endings • activated by spasm or stretch • carried by visceral afferents |
|
|
7. What is viscerosomatic pain in the GI tract?
|
Pain receptors in anterior and lateral parietal peritoneum, lesser omentum, mesentery, mesocolon
Facilitated cord segments in somatic areas related to the viscera’s sympathetic innervation |
|
|
8. What is the percutaneous reflex of Morley?
|
Percutaneous Reflex of Morley: This is direct transfer of inflammatory irritation from the viscera to the parietal peritoneum and abdominal wall w/o reflex through the visceral afferent nerve on a somatic afferent near the mesentery.
It produces abdominal wall rigidity, pain, and rebound tenderness. • no pain receptors in visceral peritoneum (ie: greater omentum, spleen) • aware of pain only if affect adjacent, pain-sensitive structure |
|
|
9. What about Tx of viscerosomatic reflexes in the GI tract?
|
• Small rotatores frequently affected
• Exhibit the non-neutral type motion with preference for backward bending. with rotation and sidebending to the same side as the organ involved • HVLA is often ineffective - met with a rubbery resistance • Alerts clinician to look for visceral cause |
|
|
10. Sympathetics of upper GI tract characteristics
|
• Rapid and widespread organ and somatic changes required to meet stress (flight/fight)
• Activation of one sympathetic fiber produces 4 to 40 post ganglionic fiber activations • May be detrimental if flight/fight not needed • Example - increased sympathetic tone decreases mucosal defenses against digestive acids and enzymes. |
|
|
11. Parasympathetics of upper GI tract characteristics
|
• Dominate innervation during restful activity
• Vagus, CN X, exits via jugular foramen – left - greater curvature of stomach, duodenum – right - lesser curvature, small intestines, right colon, and organs and glands up to midtransverse colon • Stimulation will increase secretion rate of most glands |
|
|
12. What can cause a reduced lymph flow in the GI tract?
|
Flow of lymph may be hindered by poorly efficient, flattened diaphragm, torsion of the fascias around the lymphatic channels.
Slight impedance of lymphatic pathways or hindrance to the function of the diaphragm can reduce the body’s ability to recover from a disease process. |
|
|
13. What are the goals of OMT in the upper GI system?
|
• Improve visceral response to stress
• Relieve congestion • Improve circulation • Enhance removal of waste products • Improve cardiac output • Improve oxygenation and nutrition (cellular) • Enhance resistance to infection • Enhance medication effectiveness • Relaxation and comfort - diagnosis/treatment |
|
|
14. What are 5 treatments for the lymphatics and fascias of the upper GI system?
|
1. Mesenteric lift (small intestines) - frees lymphatic pathways - lift upward and to right side of abdomen - respiratory cooperation.
2. Visceral manipulation of individual viscera 3. Doming of diaphragm 4. Thoracic inlet and inferior thoracic outlet 5. Lymphatic pump techniques |
|
|
15. How do you treat the sympathetics in the upper GI tract? (3 types of treatments)
|
1. Chapman’s reflexes
2. Rib raising 3. Ventral abdominal inhibition -celiac ganglion -superior mesenteric ganglion -inferior mesenteric ganglion |
|
|
16. How do you treat the parasympathetics in the upper GI tract? (3 types of treatments)
|
1. Cervical treatments especially OA and AA
2. Soft tissue techniques of suboccipital area 3. Cranial - occipitomastoid suture area (releases vagus as it exits through jugular foramen) |
|
|
17. What are the 3 basic tenets of visceral manipulation in the upper GI tract?
|
1. An organ or viscera in good health has physiologic motion
a. mobility - voluntary or diaphragmatic b. motility - inherent motion 2. Restriction implies functional impairment 3. Motion repeated thousands of times daily can bring about significant changes to organ, and to adjacent structures |
|
|
18. What is the visceral rhythm? (How many Hz?)
|
7-8 cycles per minute for visceral
Craniosacral rhythm is 8-12 Diaphragmatic respiratory rhythm is 15 - 18 |
|
|
19. What are the 2 phases of the motility cycle?
|
2 phases -
Inspir - coincides with cranial flexion Expir - coinsides with cranial extension These are toward and away from midline |
|
|
20. How does one do "visceral testing"?
|
• Mobility tests - make organ move directly
• Motility tests - “listening” • Paired organs tested together • If suspect more than one organ involvement –pressure on suspect organ while monitoring will inhibit any influence on the monitored organ |
|
|
21. What are the 3 *types* of Tx for the viscera in the upper GI?
How often? |
1. Direct
2. Indirect 3. Induction techniques (accentuate the larger motion) Results should be expected in 15 cycles 3-4 weeks between treatments |
|
|
22. What are the 4 contraindications for visceral Tx in the upper GI?
|
1. Acute infection (except bladder)
2. Foreign bodies (IUD’s, etc) 3. Calculi (relative - must carefully evaluate) 4. Thrombosis |
|
|
23. What are the sympathetics in the lower GI tract?
|
• Right half of colon T10-T11
• Left half of colon T12-L2 • Chapman reflexes • Inferior collateral sympathetic ganglion • Hyperactive sympathetic nervous system secondary to intense visceral afferent activity • Influences related to spinal cord segments – causes muscle spasm |
|
|
24. What about Chapman's reflexes in the lower GI system?
|
Diagnosis and treatment
•Lateral side of thigh •Anterior half of iliotibial band *Colon cancer – doesn’t send off Chapman reflexes b/c it is a slow growing cancer. |
|
|
25. Hyperactivity of sympathetics in the lower GI causes?
|
Hyperactivity causes:
o Increase in flatulence o Abdominal distention o Constipation o Ileus (inactivity) |
|
|
26. What are the parasympathetics in the lower GI tract?
|
•Right vagus nerve
o Right side of colon •Pelvic splanchnic o Left side of colon and pelvis S2,3,4 •Increased activity o Increase in motility and glandular secretions •Decreased activity o Decrease motility and glandular secretion •IBS caused by increased and decreased activity |
|
|
27. Goals of OMT in lower GI?
|
Effective in treatment of colitis, CD, IBS, diarrhea of idiopathic means
Goal to normalize nervous system outflow |
|
|
28. What happens if the lymphatics are congested or inhibited in lower GI?
1/2 |
• Metabolic changes
• Increased interstitial fluid and congestion • Build up of waste • Decrease oxygen and nutrients leads to: o Increased fibrosis o Scarring o Increased healing time o Increased infection |
|
|
29. What happens if the lymphatics are congested or inhibited in lower GI?
2/2 |
• Vulnerable to increased pressure on thin mesenteries leading to edema – inhibits healing
• Thoracic diaphragm – drainage thru thoracic duct • Pelvic diaphragm – spasm secondary to disease and surgery of lower sigmoid, rectum, and anus - Innervated by pudendal (S2-S4) |
|
|
30. What are DRGs?
|
DRGs tell you how long the insurance allows the pt to stay in the hospital.
|
|
|
31. How often do you treat a lower GI post op patient?
|
Treat post op pt 3x a day until bowel sounds are heard
|
|
|
32. Signs and symptoms of stage 1
|
STAGE 1:
• Immediately post op consider hemodynamics and electrolyte imbalance • Decrease or absent bowel sounds • Decrease breathing due to neuromuscular splinting • Paraspinal musculature – reflex hypertonicity secondary to surgical interruption of dermatome and myotome segments |
|
|
33. Three treatments for stage 1
|
Tx of STAGE 1:
1. Inhibition of hypertonic paravertebral muscles to state of relaxation -2-3 min 2. Inhibition of hypertonic paravertebral muscle sin the thoracic spine, especially at site of surgery 3. Indirect fascial release of the diaphragm thoracic inlet, mid cervical spine (phrenic nerve) |
|
|
34. Signs and symptoms of stage 2
|
STAGE 2:
• Less neuromusclular splinting • Hemodynamic and electrolytes are normalized • Bowel sounds present • Pt on oral fluids • Breathing much more regular |
|
|
35. Three treatments for stage 2
|
Tx of STAGE 2:
1. Apply inhibition to paravertebral segments related to sympathetic innervation of the viscera of the surgical site Look for TTC? 2. Rib raising bilateral (1-3 minutes) 3. Indirect fascial release of tissue a. At surgical site b. At thoracic and sternal region c. Cervical paravertebral areas |
|
|
36. Signs and symptoms of stage 3
|
STAGE 3:
• Pt ambulating • Oral intake better • Minimal neuromuscular splinting |
|
|
37. Three treatments for stage 3
|
Tx of STAGE 3:
• Inhibition of paravertebral muscles at site • Specific manipulation of segmental vertebral units • Pectoral traction w/lympathic and pedal pumps |
|
|
38. What is another good Tx to do for all post op GI pts?
|
***Condylar decompression and CV4 are good techniques at all stages***
|
|
|
39. Symptoms and findings of sympathetic dominant pt
|
• Symptoms
o Constipation o Abdominal distention o Flatulence • Findings o Chapman tenderpoints |
|
|
40. Five treatments for a sympathetic dominant pt
|
1. Circular massage of Chapmans points
2. Rib raising T10-11 (inhibitory) 3. Soft tissue to paraspinal area of T12-L2 4. Inferior mesenteric ganglion 5. Thoracolubar paraspinal inhibition (Increase bowel activity which improves ileus and diminishes bloating) |
|
|
41. Symptoms of a parasympathetic dominant pt
|
•Symptoms
o Nausea and vomiting o Diarrhea o Cramps (hyperactivity of colon) •Exam o Right colon - OA, AA, occipitomastoid sutures o More tension on the right |
|
|
42. Four areas to treat in a parasympathetic dominant pt
|
1. Treat C3-5 to influence the phrenic nerve
2. Sacrum – *rock easily on superior transverse axis (moves freely) 3. Innominates – superior shear – fix shear 4. Lumbosacral spine |
|
|
43. What about lymphatic congestion Dx and Tx?
|
• Check for fascial torsion and somatic dysfunction of thoracic inlet
• Soft tissue -Lumbar spine -Lower 6 ribs -Xiphoid process (dome diaphragm) • Relaxation of pelvic diaphragm -Relieves congestion and pain in pelvis |
|
|
44. Where are the spinous processes in relation to the vertebral body in the lumbar spine?
|
The spinous processes are at the same level as the vertebral body
|
|
|
45. Characteristics of the lumbar vertebrae
|
Transverse Process are long and thin and directed laterally
Large vertebrae support postural weight Wedge Shaped & higher anterior to maintain lordosis |
|
|
46. Latissimus dorsi
|
Origin:
-T7-12 -Iliac crest -Thoracolumbar fascia Insertion: -Intertubercular groove of humerus Action: -Adducts, extends, internally rotates arm -Raises body to arms during climbing -Extension and lateral flexion of the lumbar spine Innervation: -Thoracodorsal nerve (C6-8) |
|
|
47. Gluteus maximus
|
Origin:
-Thoracolumbar fascia -Dorsal sacrum -Sacrotuberous ligament -Ilium Insertion: -Iliotibial band -Greater tuberosity of femur Action: -Extends hip and stabilizes torso Innervation -Inferior Gluteal nerve (L5,S1-2) |
|
|
48. Quadratus lumborum
|
Origin:
-12th rib -Lumbar transverse processes Insertion: -Iliolumbar ligament -Iliac crest Action: -bilateral contraction creates extension -unilateral contraction causes extension with ipsilateral sidebending Innervation: -T12 and L1-4 ventral rami |
|
|
49. Piriformis
|
Origin:
-Lateral border of the sacrum Insertion -Greater trochanter Action: -External rotation of extended thigh -Abduction of flexed thigh Innervation: -L4-S3 ***Only muscle to bridge the anterior SI joint*** |
|
|
50. Psoas major
|
Origin:
-Transverse process of T12-L5 Course: -Along pelvic brim behind inguinal ligament in front of hip joint Insertion: -Lesser trochanter of Femur Action: -Flexes and internally rotates hip Innervation: -L1-3(2-4) ventral rami |
|
|
51. Iliacus
|
Origin:
-Superior 2/3 of iliac fossa -Inner lip of illiac crest -Ventral sacroilliac and iliolumbar ligaments -Upper lateral sacrum Course: -Iliac spines & capsule of hip joint Insertion: -Lateral tendon of psoas Innervation: Femoral nerve (L2-L3) |
|
|
52. Importance of iliopsoas?
What does it do? |
Important in function and stability
Actions: -Hip flexion -Lumbar sidebending (unilateral contraction) -Constant activity in erect posture |
|
|
53. Lumbar ligaments
|
1. Anterior longitudinal ligament
-From the base of the occiput to the anterior sacrum 2. Posterior longitudinal ligament -From posterior body of the axis down to the sacrum. -It narrows as it descends |
|
|
54. Iliolumbar ligament
|
Attaches:
-Transverse processes of L4 & L5 & iliac crest Increase stability at the lumbosacral junction -Commonly strained in traumatic injuries *First ligament to become tender with lumbar posture changes -Tender area 1” superior & lateral to PSIS on the iliac crest |
|
|
55. Nucleus pulposus
|
Fluid filled
Surrounded by anulus fibrosus Moves in opposite direction to vertebral motion |
|
|
56. Physical exam for back pain
|
General physical exam
Gross Lumbar Active Range of Motion: -PROM if limitations in AROM -Flexion -Extension -Sidebending -Rotation Segmental Motion Testing Neurological Examination -Motor, Sensory, Reflexes Special Tests as indicated |
|
|
57. Tests for individual muscles
|
Iliopsoas
-Thomas Test Piriformis -Internal Rotation of Lower Extremity Latissimus dorsi, Gluteus maximus, Quadratus lumborum -More complicated -History -Palpation of muscle area |
|
|
58. Pathogenesis and symptoms of herniated disc
|
Pathogenesis:
Narrowing of Posterior longitudinal ligament -Posterolaterally -Most commonly L5-S1 & L4-L5 Symptoms: Sharp low Back Pain with radiculopathy -Worsened with Valsalva Motor, sensory deficits & decreased reflexes associated with affected nerve root |
|
|
59. L4 neuro exam
|
Tibialis anterior:
-Foot inversion & Dorsiflexion -Patellar reflex* -Deep peroneal nerve (L4, L5, S1) Sensation: -Medial aspect of foot sensation -Medial leg to tibial crest |
|
|
60. L5 neuro exam
|
Extensor Hallicus longus
-Great toe extension -Deep peroneal nerve (L5) Gluteus medius -Abduct the leg when lat rec -Superior gluteal nerve (L5) No reflex Sensation: Lateral leg and Dorsum of foot |
|
|
61. S1 neuro exam
|
Peroneus longus and brevis: Foot eversion
-Sup. Peroneal Nerve (S1) Gastrocnemius / Soleus: -Tibial Nerve S1-S2 Gluteus Maximus: -Inferior Gluteal Nerve (S1) -Resist Hip extension while pt is prone Achilles tendon reflex* Sensation: Lateral foot sensation |
|
|
62. How can you determine which disc is herniated based on physical examination?
|
Iliopsoas: T12, L1, L2, L3
Quadriceps: Femoral Nerve, L2,L3,L4 - extensor of the knee Hip adductor group: Obturator N. - L2, L3, L4 - adduction of hip Tibialis anterior: Deep Peroneal N. - L4 - foot dorsiflexion with inversion |
|
|
63. S2, S3, S4 neuro exam
|
Motor Testing:
Intrinsic muscles of the foot Sensory Testing: 3 concentric rings around the anus S2: outer S3: middle S4: innermost |
|
|
64. Herniated disc exam and Tx?
|
1. Physical Examination
a. Paraverterbral muscle spasm b. Straight leg raising test positive c. Rectal weakness 2. Imaging a. MRI if needed 3. Treatment i. Soft tissue ii. Muscle relaxation iii. Gentle OMT in acute setting – Indirect iv. Chronic – Direct techniques o.k. Conservative i. Bedrest, NSAIDS, Steroids, Muscle relaxants Surgery i. If deficit is progressive or severe or if pain is intolerable |
|
|
65. What is spinal stenosis?
|
Definition:
Narrowing of spinal canal Etiology: Degenerative changes - Osteoarthritis Symptoms: Aching low back pain to lower leg(s) Worsened by lumbar extension Standing, walking, lying supine Relieved by sitting |
|
|
66. Spinal stenosis exam and Tx?
|
1. Physical Examination:
a. Pain exacerbated by lumbar extension b. Compression: Hypotonic anal sphincter 2. Imaging: a. X-Ray: Osteophytes 3. Treatment: a. OMT Decrease restrictions & increase ROM (Myofascial, Indirect techniques) b. NSAIDS c. Epidural injection d. Surgery (Laminectomy with decompression as last resort) |
|
|
67. What is spondylosis?
|
Degenerative changes within the intervertebral disk with ankylosing of adjacent vertebral bodies
|
|
|
68. What is spondylolysis?
|
Definition:
Defect / fracture of pars interarticularis WITHOUT anterior displacement of the vertebral body Symptoms: Similar to spondylolisthesis Diagnosis: -Oblique x-rays show the fracture as a “collar” on the neck of the scotty dog -Bilateral oblique standing x-ray views (Collar on the neck of Scottie dog) |
|
|
69. What is spondylolisthesis?
|
Definition:
Anterior displacement of one vertebral body in relationship to the one below Occurs in 20-70% of patients with spondylolysis Found primarily in lumbar spine Most often L5 on S1 (75%) |
|
|
70. How are spondylolistheses graded?
|
Grading is based on degree of displacement on the vertebra below
I - 0% - 25% II - 25% - 50% III - 50% - 75% IV - 75% or greater |
|
|
71. Symptoms of spondylolisthesis?
|
Symptoms:
-Aching low back pain with or without radiation buttock, posterior thigh, leg or foot -Pain increased in extension -Tight hamstrings -Aggravated by activity and relieved by rest -Usually painless in children |
|
|
72. Physical exam and imaging of spondylolisthesis
|
Physical Exam:
Hypertonic Hamstring muscles (Grade I & II) -if severe enough may induce gait changes Neurological deficits only in higher grades -III and IV lead to postural deformities --Exaggerated lumbar lordosis --Backward tilting of pelvis --Protruding abdomen -L5-S1 spondylolisthesis is assoc with L4 disc herniation Imaging: Lateral X-Rays: Reveal forward slippage |
|
|
73. Treatment for spondylolisthesis
|
1. OMT
-Reduce lumbar lordosis -Soft tissue, indirect myofascial -Muscle energy hamstrings -Stretching exercises to hamstrings ***HVLA is contraindicated*** Conservative: -Weight loss -Exercise Surgery: -Grade III or IV -Rapidly progressing symptoms -Gait abnormalities |
|
|
74. What is piriformis syndrome?
|
Definition:
Peripheral neuritis of the sciatic nerve caused by somatic dysfunction of piriformis Etiology: Spasm, trauma, repeated stressors, sacral base unleveling, external pressure (wallet) Symptoms: -Similar to disc herniation with radiation, local buttock pain. -Sciatic Nerve pierces through the piriformis in some patients Treatment: -OMT -Muscle energy to Piriformis -Sacrum |
|
|
75. What is psoas syndrome?
|
Etiology:
Hypertonic psoas due to any of the following: -Prolonged hip flexion -Organic causes --Appendicitis --Ureteral calculi --Salpingitis Symptoms: Aching back pain with possible radiation to groin Imaging: Not needed unless persistent Treatment: -Rest -Muscle energy to stretch iliopsoas muscle is effective -L1 or L2 Somatic Dysfunction -Contralateral Piriformis somatic dysfunction |
|
|
76. Physical exam findings for a psoas syndrome (non specific)
|
1. Positive Thomas Test
2. Flexed or extended somatic dysfunction of L1 or L2 3. Positive pelvic shift test to the contralateral side 4. Sacral dysfunction on an oblique axis 5. Contralateral piriformis spasm |
|
|
77. Physical exam findings for a psoas syndrome on the LEFT
|
Positive Thomas Test on the left
L2 F RLSL L On L Sacral Dysfunction Right Piriformis spasm |
|
|
78. What are the red flags to look out for with lumbar problems?
|
1. Severe low back pain with sudden onset and without history of trauma
(i.e. dissecting aortic aneurysm) 2. Claudication symptoms with back pain (Spinal stenosis) 3. Pain that wakes the patient from sleep (Malignancy until proven otherwise!) 4. Rapidly progressing neurological deficits (Epidural abscess/ infection) |
|
|
79. What are the 6 components of a full sacral Dx?
|
1. Standing Flexion test
2. Seated Flexion test 3. Sulci Depth 4. ILA depth and vertical orientation 5. Spring test 6. Sphinx test |
|
|
80. Transverse axis of the sacrum (Superior, middle, inferior)
|
Superior
-located at S2 segment, posterior to SI joint -Respiration and craniosacral motion Middle -located at anterior convexity, S2 sacral body -Postural flexion and extension -Sacroiliac axis Inferior -Inferior limb of SI joint (looks like an L) -Ilial (innominate) rotation |
|
|
81. Standing flexion test
|
If there's a problem, this will identify the side of the problem
Hook your thumbs under the patients PSIS and look to see if they move together when the patient is asked to bend over (flex). If one PSIS moves first and farther than the other, that side is the one with the dysfunction. *Cannot make a Dx from this test alone; need to do the seated flexion test |
|
|
82. Seated flexion test
|
Only sacral motion as the inominates are locked out.
If positive; Sacroiliac dysfunction If negative, but had a positive standing flexion test; iliosacral dysfunction If both tests are positive, can be combination of a bunch of dysfunctions. |
|
|
83. Spring test
|
1. Patient is prone, hand on LS junction
2. Gentle, rapid pressure applied 3. Good spring- negative test 4. Poor spring - positive test (Sacrum is locked in extension) |
|
|
84. Three things absolutely necessary to make a sacral Dx
|
1. Sacral sulci
2. ILA's 3. Spring test |
|
|
85. Forward sacral torsions
|
Described relative to L5
Sacrum is flexed -The deep sulcus will be on the opposite side of the axis of rotation Includes: -Left on left -Right on Right |
|
|
86. Backward sacral torsions
|
The deep sulcus will be on the same side as the axis of rotation
Sacrum is extended Includes: Left on Right Right on Left |
|
|
87. Left on Left
|
Deep sulcus: right
Inferior/posterior ILA : left Seated flexion test: + on right Spring test: negative |
|
|
88. Right on Right
|
Deep sulcus: left
Inferior/posterior ILA : right Seated flexion test: + on left Spring test: negative |
|
|
89. Left on Right
|
Deep sulcus: right
Inferior/posterior ILA : left Seated flexion test: + on left Spring test: positive |
|
|
90. Right on left
|
Deep sulcus: left
Inferior/posterior ILA : right Seated flexion test: + on right Spring test: positive |
|
|
91. Left unilateral flexion
|
Deep sulcus: left
Inferior/posterior ILA : left Seated flexion test: + on left Spring test: negative Negative sphinx test |
|
|
92. Right unilateral flexion
|
Deep sulcus: right
Inferior/posterior ILA : right Seated flexion test: + on right Spring test: negative Negative sphinx test |
|
|
93. Bilateral flexed
|
Deep sulcus: left and right
Inferior/posterior ILA : left and right Seated flexion test: negative Spring test: negative |
|
|
94. Left unilateral extension
|
Deep sulcus: right
Inferior/posterior ILA : right Seated flexion test: + on left Spring test: positive Positive sphinx test |
|
|
95. Right unilateral extension
|
Deep sulcus: left
Inferior/posterior ILA : left Seated flexion test: + on right Spring test: positive Positive sphinx test |
|
|
96. Bilateral extended
|
Deep sulcus: shallow left and right
Spring test: positive |
|
|
97. What is the Hoover test?
|
Tests for malingerers
Patient supine and physician holds beneath the patients calcaneus When the patient tries to raise one leg there should be contralateral pressure on the opposite heel if that person is trying. |
|
|
98. Review - what is the sphinx test?
|
AKA BACKWARD BENDING TEST
Evaluates sacral base movement posterior or anterior Normal = lumbar extension = anterior sacral base motion = Negative Method: 1. Note depth of the sacral sulci with thumbs 2. Patient comes up on elbows 3. Note the depth of the sacral sulci Interpretation: More Asymmetric: Positive (backward torsions b/c sacrum cannot flex) More Symmetric: Negative (forward torsions) |
|
|
99. Straight leg raising test
|
Evaluate for sciatic nerve compression
-Raises leg till patient feels pain -Then bring leg just below the level of pain and dorsiflex foot Positive test will causes pain secondary to sciatic nerve compression (b/c dorsiflexion stretches the sciatic nerve) Normal leg can be raised to 70-80deg of hip flexion *False positive due to tight hamstrings (will not cause pain when you dorsiflex foot) |
|
|
100. Motions of the pelvis
|
Anterior and Posterior Rotation about the SI joint about 3 transverse axes surrounding S2:
-Respiratory -Cranial -Dynamic Shearing/gliding about the SI joint Inflare and Outflare (adducted/abducted) Abduction or Adduction of Pubic symphasis Shearing/gliding about the Pubic symphasis |
|
|
101. Anterior inominate rotation
|
ASIS: more inferior
PSIS and Ischial tuberosity more superior on same side Ipsalateral leg may appear to be longer The side of the positive standing flexion test is the side on which the dysfunction is located and side on which the above signs will be found. |
|
|
102. Posterior inominate rotation
|
ASIS: more superior
PSIS and Ischial tuberosity more inferior on same side Ipsalateral leg may appear to be shorter The side of the positive standing flexion test is the side on which the dysfunction is located and side on which the above signs will be found. |
|
|
103. Superior inominate shear
|
Ischial Tuberosity, ASIS, PSIS, and med. malleoli more superior on same side
The side of the positive standing flexion test is the side on which the dysfunction is located and side on which the above signs will be found. |
|
|
104. Inferior inominate shear
|
Ischial Tuberosity, ASIS, PSIS, and med. malleoli more inferior on same side
The side of the positive standing flexion test is the side on which the dysfunction is located and side on which the above signs will be found. |
|
|
105. Superior pelvic shear with hip replacement history
|
Internal Rotation risks dislocation of the hip joint in this patient population
External rotation will allow for some “packing” of the hip joint to allow for traction then pull of the lower extremity to translate to the pelvis Goal is to limit the loss of energy from pull to pelvis so less force is needed |
|
|
106. Pelvic inflare
|
Distance of ipsilateral ASIS to midline decreased
Standing flexion test positive ipsilaterally Superior ASIS ipsilaterally Equal to superior PSIS ipsilaterally Pubic rami equal Iliac Crest superior ipsilaterally Ischial tuberocity equal |
|
|
107. Pelvic outflare
|
Distance of ipsilateral ASIS to midline increased
Standing flexion test positive ipsilaterally Inferior ASIS ipsilaterally Equal to superior PSIS ipsilaterally Pubic rami equal Iliac Crest inferior ipsilaterally Ischial tuberocity equal |
|
|
108. Pubic symphasis abduction/adduction
|
Abducted
Pubic Symphasis widened Adducted Pubic Symphasis narrowed |
|
|
109. Superior/inferior pubic shear
|
Superior
Pubic tubercle is superior ipsilaterally Standing flexion test is positive ipsilaterally usually Inferior Pubic tubercle is inferior ipsilaterally Standing flexion test is positive ipsilaterally usually |
|
|
110. What is sacroilitis?
|
Direct inflammation at the SI joint causing pain
Often refers to the groin (ant hip region) Anti-inflammatory and steroid injection |
|
|
111. What is lateral trochanteric bursitis?
|
Iliotibilal band irritation of bursa = inflammation
Injection, medications, pelvic balancing |
|
|
112. What is Coccidynia?
|
Pain at the coccyx
Malpositioning due to injury, fracture, pubococcygeal strain Often treatable with intrarectal BLT/MFR. WHAT?!?!?! |
|
|
113. Vascular problems in the pelvis
|
1. Peripheral Vascular Disease
Diminished vascular return due to incompetence of lower extremity veins 2. Lower Extremity Edema Multiple potential causes 3. DVT Clot formation within the deep veins of the lower extremities Risk of embolizing to the lungs |
|
|
114. GI problems related to pelvis
|
1. Incontinence Bowel
Can be a medication effect or loss of sphincter tone Pelvic diaphragm can be the cause of a muscular issue 2. Irritable Bowel Syndrome Functional issue. Structure can be the culprit 3. Diarrhea or Constipation Multiple causes Releasing pelvic congestion can improve symptoms 4. Illeus Bowels stop functioning – multiple casues Pelvic splanchnics and pelvic congestion 5. Small Bowel Obstruction Actual obstruction of small or large intestine Pelvic splanchnics and pelvic congestion |
|
|
115. Renal problems related to pelvis
|
1. UTI: Cystitis
Pubic dysfunction usually accompanies this Improving blood flow to and from can help 2. Nephrolithiasis Especially when the stone is at the ureter near the bladder Fascial torsion here may inhibit passing |
|
|
116. Urogenital problems related to pelvis
|
1. Incontinence Bladder
Again Pubic dysfunction predominates 2. Erectile Dysfunction Pubic dysfunction and parasympathetic tone 3. BPH Congestion within Prostate Pubic Diaphragm 4. Prostatitis Infection within Prostate Pubic Diaphragm 5. Endometriosis Endometrial tissue outside the uterus Pain is then hormonally mediated OMT to and from area may be helpful 6. Dysparanuria Male: ejaculation is sympathetically mediated but blood to and from is key (Pelvic Diaphragm) Female: Dryness (hormonal and blood flow), vaginal muscle/fascial restriction (Pubic Diaphragm and Vaginal Release) |
|
|
117. Respiratory problems and pelvis
|
Asthma/COPD/Pneumonia:
Sacrum improperly rocking about SI joints can impede respiration Pelvic Diaphragm restriction can impede respiration |