![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
244 Cards in this Set
- Front
- Back
|
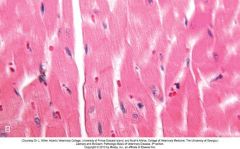
Left Ventricle Hypertrophy |

|
|
|
Individual cadiomyocytes hypertrophied |
|
|
|
Osteoporosis - Atrophy |

|
|
|
Atrophic liver - hepatocytes smaller/narrower & sinusoids correspondingly wider |
|
|
|
Cerebellar hypoplasia |

|
|
|
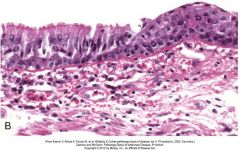
MetaplasiaAirway epithelium in response to chronic inflammation Normal Columnar cells replaced with abnormal stratefied squamous epithelium |
|
|
|
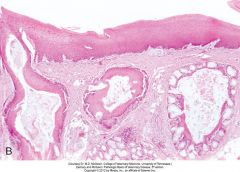
Metaplasia Vitamin A necessary for maintenance of normal epithelium. Deficiency → epithelium and goblet cells in glands replaced by keratinised stratified squamous epithelium |
|
|
|
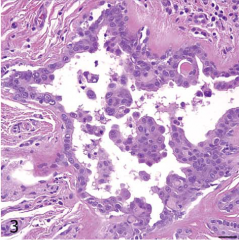
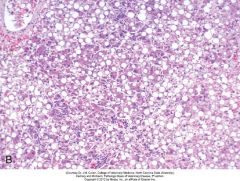
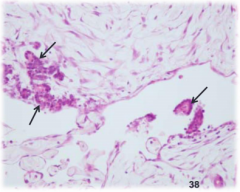
Canine Mammary Gland Dysplastic duct with crowded and disorganised epithelial cells projecting into lumen. |
|
|
|
Anaplastic cells - failure to differentiate - cant tell what type of cells they are |
|
|
|
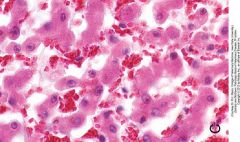
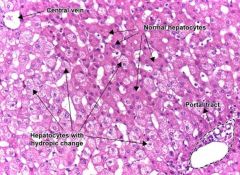
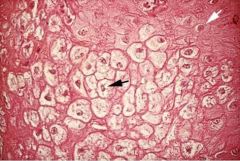
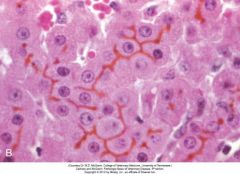
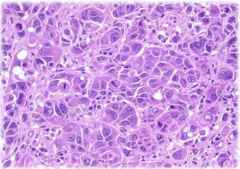
Hydropic ('watery') degeneration of hepatocytes |
|
|
|
Hydropic degeneration - squamous epitheliumBlack arrow identifies swollen but still viable cellNucleus displaced, ‘clearing’ of cytoplasm, cell borders remain intact |
|
|
|
Fatty Degeneration of Liver |
|
|
|
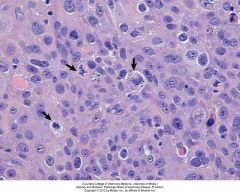
Liver Necrosis Cells around central vein showing signs of necrosis Cytoplasmic palor - loss of RNA and protein Nucleus shrinkage (karyopyknosis), fragmentation (karyorrhexis), lysis (karyolysis) |
|
|
|
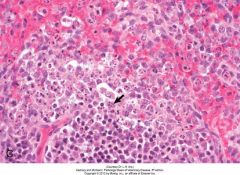
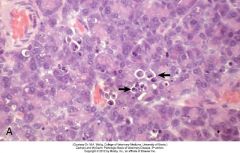
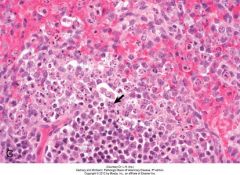
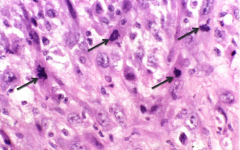
Karyorrhexis in splenic lymphocytes - dog with parvovirus infection. Lymphocyte nuclei fragmented as a result of viral attack (arrow). |
|
|
|
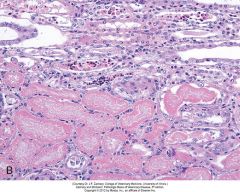
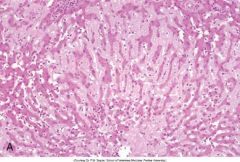
Coagulation necrosis of renal tubular epithelial cells Necrotic cells have ‘ghostly’ appearance - homogeneous pale eosinophilic cytoplasm but retained cell outlines (structured necrosis) and nuclear changes such as karyopyknosis and karyolysis. |
|
|
|
Liquefactive necrosis, lung abscesses, cow Liquified material consists of cell debris & large numbers of mostly neutrophils (bacteria not visible with H&E stain) |
|
|
|
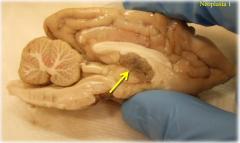
Liquefactive necrosis, brain, dog The clear/pale zone in the cerebral cortex represents areas of near total loss of cells and tissue. The cells in the spaces are macrophages attempting to clear up the damage. Grossly, this would have a fluid consistency. |
|
|
|
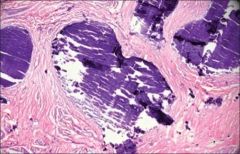
Caseous Necrosis Tuberculosis, lymph node, cow Necrosis is structureless - cell walls disrupted, tissue architecture lost, a mixture of nuclear and cytoplasmic amorphous granular debris |
|
|
|
Fat necrosis, dog. Necrosis with inflammation, basophilic foci of saponification & cholesterol clefts |
|
|
|
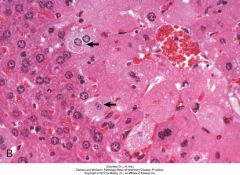
Apoptosis, Pancreas, rat Individual acinar cells shrunken with chromatin condensed and fragmented (arrows). Inflammation absent. |
|
|
|
Pathological mineralisation/calcification If present in large amounts it appears as gritty white granular deposits grosslyMicroscopically as amorphous basophilic granules of varying size – intra or extra cellular Dystrophic Where deposited in areas of necrosis |
|
|
|
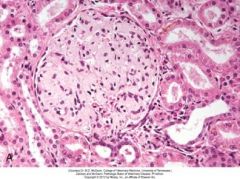
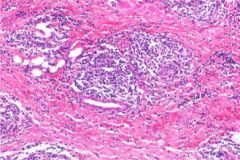
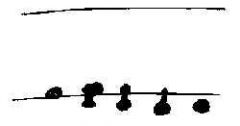
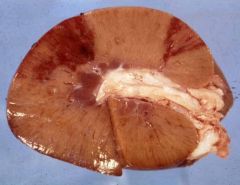
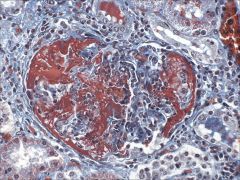
Amyloidosis, kidney, cross section, dog Black foci (dots) are glomeruli-containing amyloid stained by Lugol’s iodine Renal glomerulus contains large amounts of pale homogeneous eosinophilic material (amyloid) using H&E stain |
|
|
|
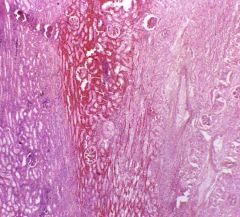
Amyloidosis, liver, dog Spaces of Disse expanded by eosinophilic proteinaceous material (amyloid) that has caused atrophy of hepatic cords (H&E stain) |
|
|
|
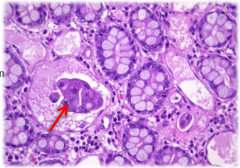
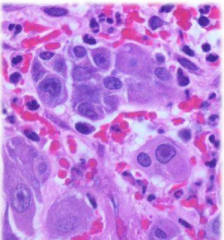
JaundiceBile casts in bile canaliculi - result of a high rate of bilirubin excretion by liver secondary to widespread haemolysis |
|
|
|
Acute Hyperaemia of the brain in acute encephalitis |
|
|
|
Fibrin exudate of acute inflammation |

|
|
|
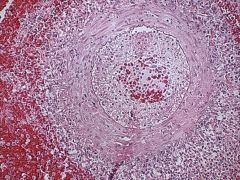
Granuloma formation Lymphocytes and area walled off with fibronous material - Tuberculosis in the lung |
|
|
|
Neutrophils First line of defense in acute inflammation Death of large numbers can lead to liquefaction of tissues - formation and accumulation of pus |
|
|
|
Eosinophils Present in allergic or parasitic disease Can also phagocytose |
|
|
|
Macrophages (Monocytes in circulation) Acute and Chronic Inflammation Large oval with kidney bean nuclei and foamy cytoplasm Develop into multinucleated giant cells with horse shoe nuclei |
|
|
|
Lymphocytes B or T lymphocytes (cant be distinguished by histological appearance) Small round sounds mostly nucleus Enter areas of acute inflammation after 24-48hrs |
|
|
|
Plasma Cells Activated B lymphocytes - producing antibodies Pink/red cytoplasm possibly with halo of white above the nucleus |
|
|
|
Fibroblasts Proliferate in chronic inflammatory lesions Play a role in healing and repair Produce collagen and extracellular matrix proteins |
|
|
|
Diffuse acute fibronous pericarditis |
|
|
|
Serous inflammation in the coelmic cavity of a bird (clear fluid - very little protein) |

|
|
|
Serous Inflammation microscopic view |
|
|
|
Catarrhal inflammation microscopic view Thick mucus with abundant goblet cells Occurs in parasitic disease and chronic inflammation Exudate if opaque thick fluid |
|
|
|
Fibronous peritonitis Gelatinous exudate due to coagulation by the amount of fibrin Can adhere to tissues and create casts of areas |

|
|
|
Purulent (suppurative) inflammation Pus exudate due to death of neutrophils Thoracic empyema or pyothorax |

|
|
|
Cellulitis Non-encapsulated suppurative inflammation in the subcutaneous tissue |

|
|
|
Eosinophilic myositis Exudate contains large numbers of eosinophils Associated with parasites, hypersensitivity and unknown mechanics Exudate is green discoloured |

|
|
|
Haemorrhagic Inflammation Haemorrhagic Enteritis Large number of erythrocytes associated with sever damage to endothelial cells |

|
|
|
Pyogranuloma Neutrophils at center of granuloma - could be bacterial cause |
|
|
|
Myocardial fibrosis Pale areas of fibroblasts - regeneration could not occur so switched to repair |
|
|
|
Granulation tissue Fibroblasts forming in perpendicular to blood vessels with lymphocytes throughout |
|
|
|
Fibrous connective tissue (Fibrosis) Decrease in blood vessels and cells - scar formation |

|
|
|
Scar; Renal Infarct |
|
|
|
Proud Flesh Excess/exuberant proliferation of granulation tissue |

|
|
|
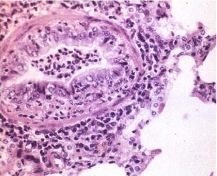
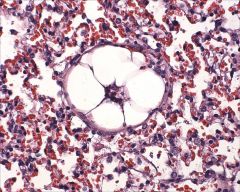
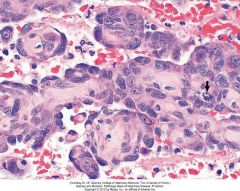
Anaphylaxis Pulmonary oedema (alveolar spaces filled with proteinous fluid) Vascular congestions (alveolar wall filled with blood) |
|
|
|
Hypersensitivity type 1 Oedema and mast cells present |
|
|
|
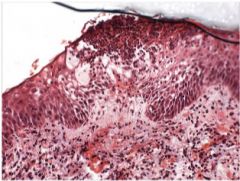
Flea Bite Nibble A break of the epidermis - replaced with degranulated eosinophils and neutrophils |
|
|
|
Heave line on horse Muscles used to struggle for breath |

|
|
|
Brincho thickening Inflammatory cells within the lumen Even slight thickening of airways cause massive increases in resistance |
|
|
|
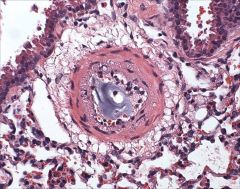
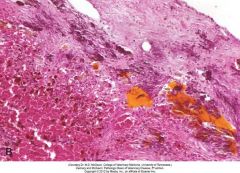
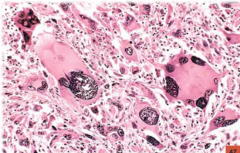
Tuberculosis lesion Bright eosinophilic material is fibrin Clear spaces are oedema Lymphocytes and macrophages present |
|
|
|
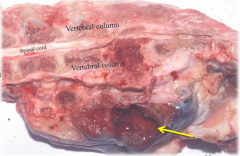
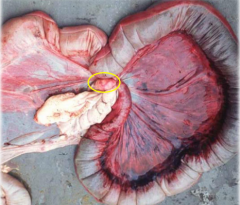
Local Congestion due to small intestine volvulus (twisted bowel) Blue color due to deoxygenated haemoglobin, wet, swollen Can lead to necrosis Passive process due to decreased venous outflow from affected area (General caused by congestive heart failure) |

|
|
|
Local Congestion due to gastric volvulus (twisted stomach) Vein drainage from the stomach is blocked Blue color due to deoxygenated haemoglobin, wet, swollen Passive process due to decreased venous outflow from affected area (General caused by congestive heart failure) |
|
|
|
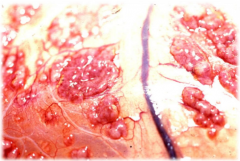
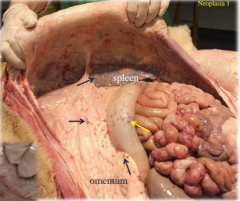
Hyperaemia of the small and large intestine and cecum Increased arterial blood flow to the area Red due to oxygenated haemoglobin, heat, swollen Pathological - secondary to inflammatory mediators due to tear in colon (Physiological due to normal increased workload and flow) |

|
|
|
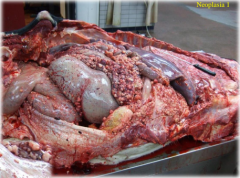
Hyperaemia due to ruminal tear leading to peritonitis Red due to increased blood flow to the area due to inflammatory mediators and oxygenated haemoglobin |

|
|
|
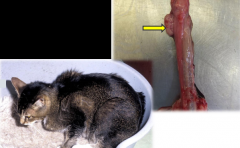
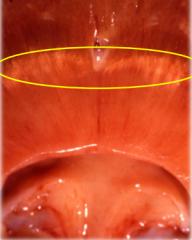
Hyperaemia of the trachea - bright red luminal appearance Commonly seen in animals that have major respiratory distress prior to death |

|
|
|
Diagram of haemorrhage due to rupture of blood vessel Escape secondary to vascular damage (trauma/ inflammation) |

|
|
|
Diagram of haemorrhage due to diapedesis Red blood cells pass through intact blood vessel walls secondary to congestion (increased pressure) |
|
|
|
Petechiae of gums Small 1-2mm spots of haemorrhage |

|
|
|
Petechiaetion on kidney 1-2mm spots of haemorrhage |

|
|
|
Petechiae in cortex of crossection of kidney Damage due to toxin |
|
|
|
Haemorrhage within cortex of kidney Red blood cells accumulating between tubules Coagulative necrosis of tubular epithelial cells due to toxin |

|
|
|
Areas of petechiae and ecchymoses Petechiae 1-2mm spots of haemorrhage (purpura slightly larger vasculitis) Ecchymoses 2-3cm spots of haemorrhage |

|
|
|
Haematoma formation in a kidney Substantial solid clot Blood clotting in a localized area |

|
|
|
Large area of extravasation at medial aspect of left hind leg due to tearing of abducters of the leg Large region of haem within tissue Hyperaemia and oedema also present |

|
|
|
Extravasation near the rostral aspect of the nose (on the right side of image) Dura is expanded by large amounts of blood Subdural haemorrhage secondary to traffic accident |
|
|
|
Contrecoup Haemotoma just caudal to the cerebellum Caused by blunt trauma to the front of the head Brain moves forward in impact resulting in tearing of blood vessels in the back of the brain |

|
|
|
Cerebellar coning Pressure in the brain case increases pushing the cerebellum through the opening of the foramen magnum Cerebellum becomes flattened and cone shaped |

|
|
|
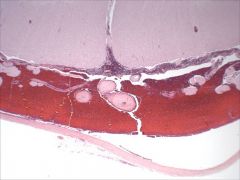
Microscopic view of subdural haemorrhage |
|
|
|
Microscopic view of haemorrhage of tissue due to leaky and faulty blood vessel |
|
|
|
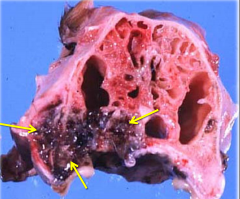
Bulging haemotoma in the lateral ventricle of the brain Site of loss can determine how critical the haemorrhage is - brain very critical |

|
|
|
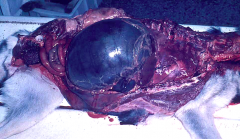
Pericardial sack - blue due to deoxygenated blood |

|
|
|
Resolving haemorrhage Macrophages phagocytose red blood cells resulting in haemosiderin |

|
|
|
Macroscopic view of oedema filling the abdominal cavity |

|
|
|
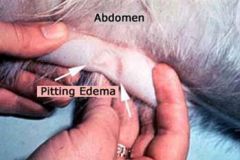
Pitting Oedema When you push your finger into an area of oedema if takes a moment to return to previous shape |
|
|
|
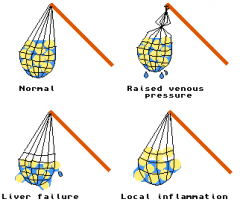
Diagram of 3 main reasons for oedema formation |
|
|
|
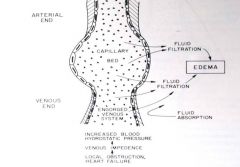
Diagram of Oedema formed due to increased intravascular hydrostatic pressure Increased pressure within the vessels pushes fluid out of the vessels Factors that increase venous pressure more important than those that increase arteriole pressure Local Oedema - vain or lymphatic occlusion Generalized oedema - congestive heart failure Transudate - Fluid passed through intact capillary walls due to imbalanced hydrostatic +/- oncotic pressures- Little or no protein or cells, low sg |
|
|
|
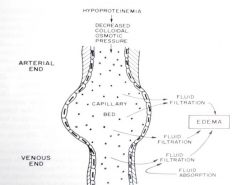
Diagram of oedema formed due to decreased oncotic pressure Fewer proteins within the vessels leading to the movement of fluid out of them Caused by nephro/enteropathies causing loss or decreased synthesis by liver disease Leads to generalized oedema Transudate - Fluid passed through intact capillary walls due to imbalanced hydrostatic +/- oncotic pressures- Little or no protein or cells, low sg |
|
|
|
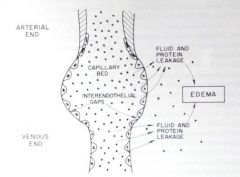
Diagram of oedema formed due to increased capillary permeability Caused by inflammatory or allergic responses Usually local Exudate - Fluid passed through injured/inflamed capillary wallsContains protein (straw coloured) & leucocytes (also known as inflammatory oedema) |
|
|
|
Oedema within trachea Fluid tends to be frothy due to air passing back and forth over it and it mixing with surfactant |

|
|
|
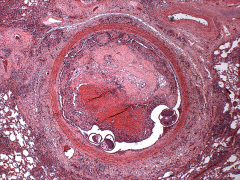
Macroscopic transsection of arteries showing thrombosis formation Can distinguish between post mortem clots by their attachment to the artery wall (PM clots dont attach) |

|
|
|
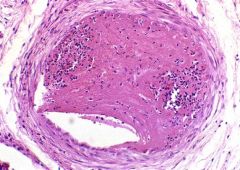
Arteriole thrombosis transsection Contains dense eosinophilic material containing fibrin and red and white blood cells Attached to the endothelial lining |
|
|
|
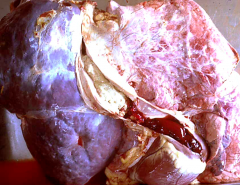
Pulmonary thrombosis (macro) Coagulation of blood in blood vessels during life Abnormal triggering of clotting mechanism |

|
|
|
Macroscopic image of Parasitic thrombus Strongylus vulgaris presence leads to damage to the endothelium resulting in thrombus formation Both intrinsic and extrinsic pathways are triggered Lead to hypoxic damage and thromboembolic colic |

|
|
|
Microscopic image of Parasitic thrombus Angiostrongylus vasorum presence leads to damage to the endothelium resulting in thrombus formation Both intrinsic and extrinsic pathways are triggered - clot filled entire vasculature |
|
|
|
Thrombus forming on the valve of the heart White head visible with black portion being the red tail White head is made up of the white constituents of the blood Red tail is the stagnation of red cells distal to the site of attachment of the white head - formed in the direction the blood is flowing |

|
|
|
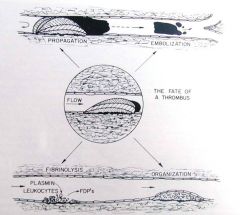
Diagram of the fate of thrombi Removal by Fibrinolysis: Plasminogen to plasmin allows fibrin to turn into FDPs breaking down the clot Propogation - Increase in size (in arteries form a white head and red tail) (in veins form a dark red cast of vein lumen) Organization - decrease in size and formation of fibrous scar within vessel wall Embolism - Before organization occurs, fragments break off and lodge in distant smaller vessels |
|
|
|
Thrombosis of the caudal (posterior) vena cava |
|
|
|
Organisation of blood vessel after thrombus Endothelial cells proliferate to seal off surface of thrombus New capillaries form through it - recanalisation |
|
|
|
Emboli lodged at the aortic bifurcation |

|
|
|
Fat embolism |
|
|
|
Fibrocartilaginous embolism |
|
|
|
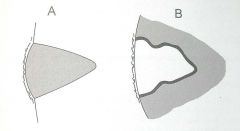
Infarction Diagram of Stages Obstructed arterial supply Initially swollen and poorly delineated After 48 hrs coagulation necrosis occurs - pale with hyperaemic border After 10 days organization occurs - indented Infarction red in loosely structured organisms Infarction pale in solid organs |
|
|
|
Renal Infarction (Macro) After 48 hrs coagulation necrosis occurs - pale with hyperaemic border |
|
|
|
Renal Infarction (Micro) After 48 hrs coagulation necrosis occurs - pale with hyperaemic border |
|
|
|
Renal Infarction Macro Organization have occurred (greater than 10 days) - indented |

|
|
|
Cardiac infarction Macro Solid organ so infarction appears white in color |

|
|
|
Splenic Infarction macro Loosely structured organism so red in color |

|
|
|
Intestinal Infarction do to small intestine volvulus Venous infarcts full of deoxygenated blood leading to very dark blue/black coloration |

2 |
|
|
Bracken Fern Toxin causing suppression of bone marrow Trilineage depression - suppression of red blood cells, white blood cells, and platelets |

|
|
|
Petechiae of mucus membranes (eye) of calves Bovine neonatal pancytopaenia - bleeding calf syndrome, haemorrhagic diathesis of neonatal calves, blood 'sweating' disease Thrombocytopaenic (increased consumption of clotting factors) and leucopaenic |

|
|
|
Liver failure Green hue to liver with rough bumpy surface, jaundice, and blood within the cavity (incapable of clotting) Acquired haemostatic disorder No ability to produce coagulation factors - inadequate synthesis Retention of bile may also interfere with vit K absorption |

|
|
|
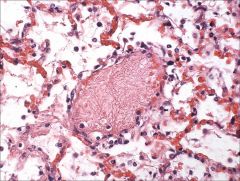
Lung of animal suffering DIC (Disseminated Intravascular Coagulation) Microthrombi within the venule of the lung (with alveoli surrounding) with platelets stuck between the meshwork |
|
|
|
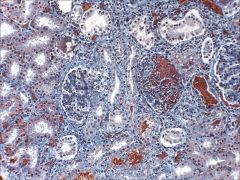
Kidney of animals suffering DIC (Disseminated Intravascular Coagulation) Thombus in glomerular tuft and microthrombi throughout the capillary loops - impair glomerular filtration |
|
|
|
Dark orange fibrin filling up glomerular tuft in animal suffering from DIC |
|
|
|
Lymph node During immune response to antigen a primary follicle, composed of re-circulating B cells and Follicular Dendritic Cells, forms a Germinal Center and becomes a secondary follicle Follicular Dendritic Cells take up antigen and can hold this on their surface for periods of >1 yr (antigen ‘depots’) |
|
|
|
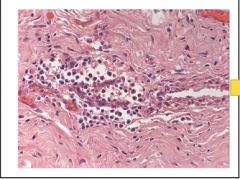
Lymph Node Intravascular lymphocytes migrate into paracortex via high endothelial venules Specialised cuboidal endothelium have receptors that bind passing lymphocytes facilitating their transmigration into node |
|
|
|
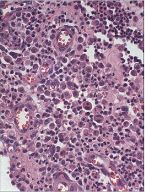
Medullary cords and sinuses of lymph node If very activated, medullary cords will contain large numbers of lymphocytes and plasma cells (many of the sinuses cells would be plasma cells) |
|
|
|
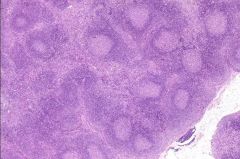
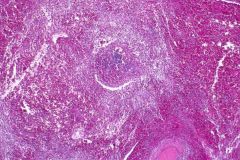
Reactive hyperplasia of lymph nodes (microscopic whole node section) Response to infection/immune-mediated disease (Draining/filtering antigens/immune complexes) Characterised by Nodal enlargement (hyperaemia/oedema) Enlarged & increased # of secondary follicles Possibly expanded paracortex (depends on antigen involved) Medullary cords distended with plasma cells Prominent sinus cell ‘traffic’ – sinus histiocytosis |
|
|
|
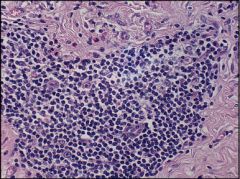
Reactive hyperplasia, Outer cortex of lymph node When follicles are antigenically stimulated (e.g. bacterial antigen) B lymphocytes in developing GCs undergo massive clonal expansion (hyperplasia) and hypermutation of their Ig-producing genes B lymphocytes with augmented affinity for the antigen selected and move to mantle zone (edges) of follicle. They then migrate to medullary cords as plasmacytes or memory cells Non-selected lymphocytes (>90%) undergo apoptosis |
|
|
|
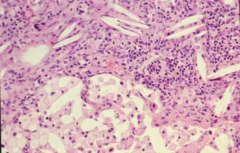
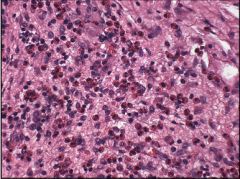
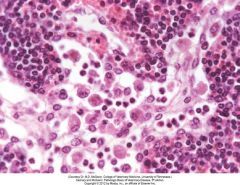
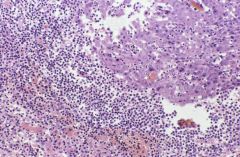
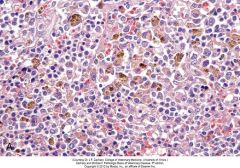
Reactive hyperplasia, medulla - sinus histiocytosis of lymph node Medullary sinusoids filled with macrophages & a few neutrophils (small dark nuclei) Most macrophages derived from perisinusoidal macrophages - some arrive via afferent lymphatics Medullary cords filled with lymphocytes and plasma cells Plasma cell precursors formed in GCs in follicles in cortex, mature into plasma cells, and migrate to cords. Their presence in large numbers in cords indicate ongoing Ig production following an antigenic stimulus |
|
|
|
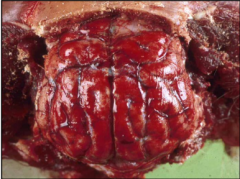
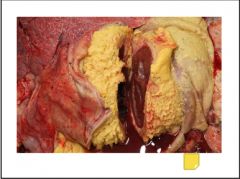
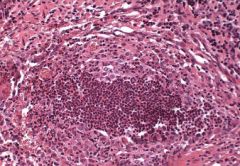
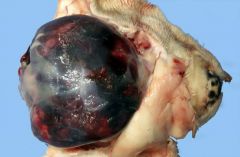
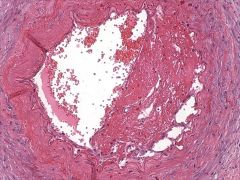
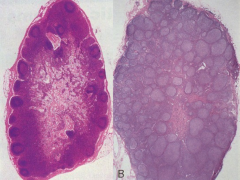
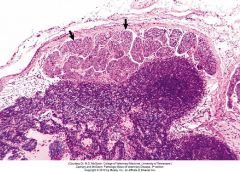
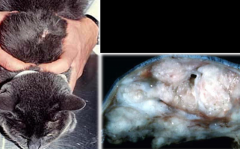
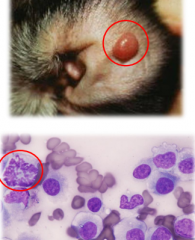
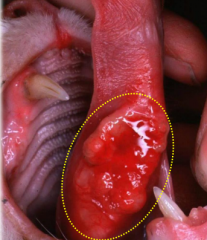
Caseous lymphadenitis - Clinical Presentation Caused by Corynebacterium pseudotuberculosis Enters skin by contaminated wound with soil, faeces, or discharge Bacteria drains to regional LNs Neutrophils and eosinophil rich inflammatory response (eosinophil = greenish tint) Has onion ring appearance due to sequential episodes of necrosis and repair Collagenous layer to wall off abscess and then another around it and around that |

|
|
|
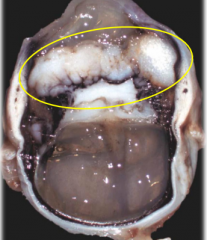
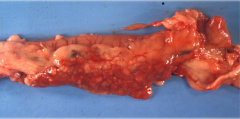
Caseous lymphadenitis - Lymph node cross section Caused by Corynebacterium pseudotuberculosis Enters skin by contaminated wound with soil, faeces, or discharge Bacteria drains to regional LNs Neutrophils and eosinophil rich inflammatory response (eosinophil = greenish tint) Has onion ring appearance due to sequential episodes of necrosis and repair Collagenous layer to wall off abscess and then another around it and around that |

|
|
|
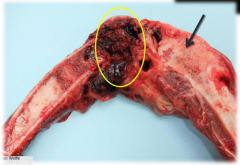
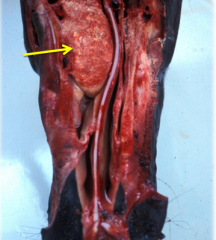
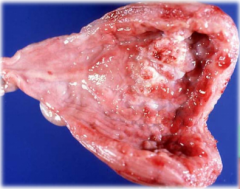
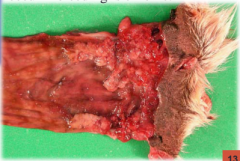
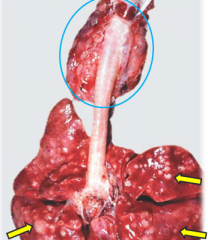
Lymphadenitis Dorsal view of opened larynx showing left and right retropharyngeal LNs grossly distended and effaced by pus Streptococcus equi causing inflammation of upper respiratory tract LNs which drain to regional retropharyngeal LNs Causes purulent lymphadenitis leading significant enlargement of periairway LNs and compression of trachea --> Strangles |

|
|
|
Lymphadenitis (Micro) Streptococcus equi causing inflammation of upper respiratory tract LNs which drain to regional retropharyngeal LNs Causes purulent lymphadenitis leading significant enlargement of periairway LNs and compression of trachea --> Strangles Greater hyperaemia/oedema Influx of leucocytes +/- necrosis |
|
|
|
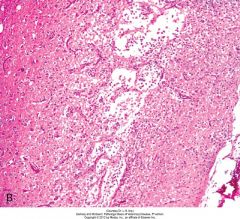
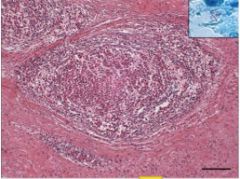
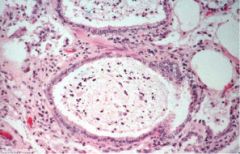
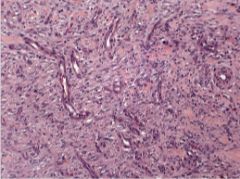
Granulomatous lymphadenitis with caseous/structureless necrosis and dystrophic mineralisation Caused by Mycobacterium bovis infection growing within macrophages Infected macrophages carry mycobacteria to draining LNs (bronchial/mediastinal) Multifocal to coalescing gritty pale abscesses |
|
|
|
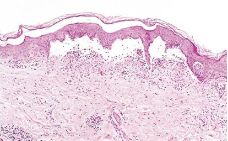
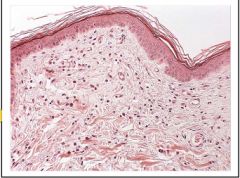
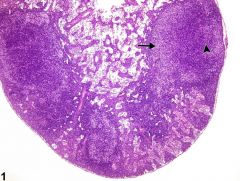
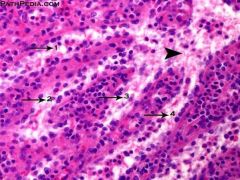
Lymph node atrophy (Micro big picture) # and size of follicles decreased (arrowhead) Paracortical lymphocytes depleted (arrow). Node reduced in size Hypocellular ‘ghost’ follicles and paracortical areas Potential Causes: Cachexia (starvation/malabsorption) cause decrease in T lymphocytes Ageing causes decrease in both T & B lymphocytes LN ‘exhaustion’ with some persistent infections |
|
|
|
Lymph node atrophy - Cloe up of ghost follicle Paracortical lymphocytes depleted Node reduced in size Hypocellular ‘ghost’ follicles and paracortical areas Potential Causes: Cachexia (starvation/malabsorption) cause decrease in T lymphocytes Ageing causes decrease in both T & B lymphocytes LN ‘exhaustion’ with some persistent infections |

|
|
|
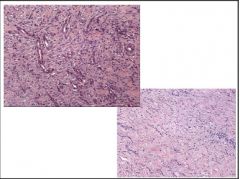
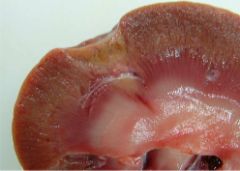
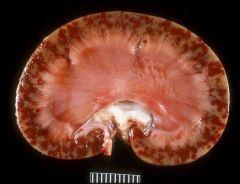
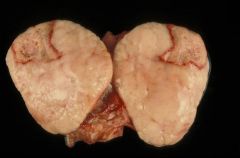
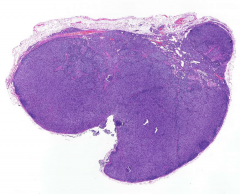
Primary Neoplasia of Lymph Node (lymphosarcoma) - Macro cross section Bulging soft white homogeneous ‘fish-flesh’ Cortex/medulla obliterated Note infarct as neoplastic lymphocytes cause vascular obstruction No difference between cortex and medulla |
|
|
|
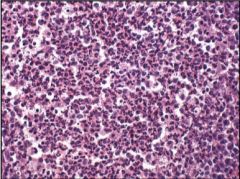
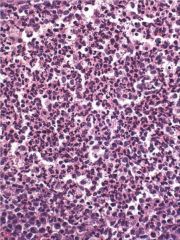
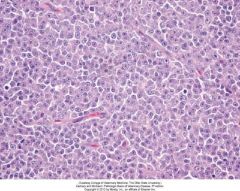
Primary Neoplasia of Lymph Node (lymphosarcoma) - Micro Monotonous sheets of often atypical neoplastic lymphoid cells Clones of cancerous lymphocytes that have taken over and are expanding the lymph nodes Lymph node architecture gone |
|
|
|
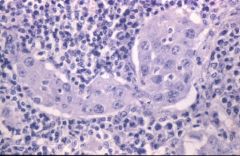
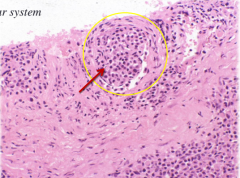
Secondary neoplasia of Lymph Node (metastatic carcinoma) Embolisation, lodgement, invasion, and growth of neoplastic emboli in subcapsular sinus (arrows) Lymph node filters emboli of metastatic neoplastic cells draining from neoplastic epithelium Cell type not normally found within the lymph node |
|
|
|
Secodary Neoplasia of lymph node Left are normal node lymphocytes while right side of section are large epitheliod cells which have metastasized from epithelial surface |
|
|
|
Close up of secondary neoplasia of lymphocyte Central cells neoplastic surrounded by normal lymphoid tissue Variation in nuclear size, cell shape, strange appearance to cell chromatin |
|
|
|
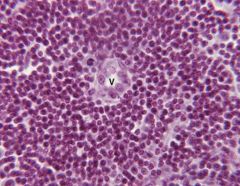
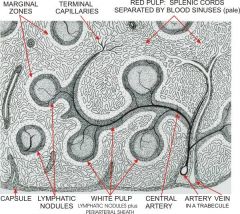
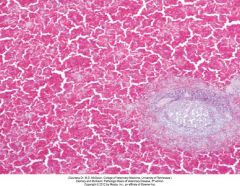
Normal Spleen with Activated Lymph Follicles C - splenic capsule WP - white pulp - Composed of B (follicles) and T (sheaths along arterioles) lymphocytes RP - red pulp - collection of erythrocytes within sinusoids being filtered for recycling and bacterial killing Ln - lymphoid nodule GC - germinal center CA - central arteriole TR - trabecula |

|
|
|
Terminal Capillaries within spleen Connect directly into venous sinuses ‘closed system’ (97%) Terminate in splenic cords ‘open system’ (3%) Other capillaries release blood into marginal zone at periphery of white pulp Blood eventually reaches sinuses of red pulp which are continuous with venules which connectto veins returning to the surface of the spleen via vessels in trabeculae |
|
|
|
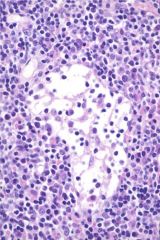
Normal Splenic Sinuses Four splenic sinuses (1-4) joining to form a larger sinus (arrowhead) ultimately empties into venous system Lined by discontinuous endothelial cells and surrounding framework of cellular splenic cords |
|
|
|
Splenomegaly (Macro) Can be caused by: Splenitis Haemolytic anaemia Torsion Chronic venous congestion Barbituates Splenic tumours |

|
|
|
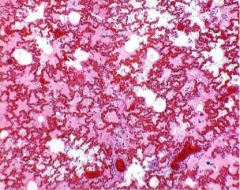
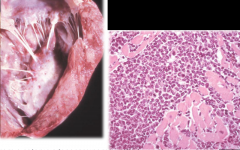
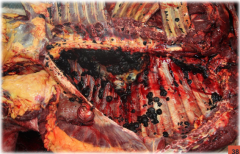
Peracute splenitis caused by anthrax - Macro slice into spleen Bacterial toxins inhibit platelet aggregation Necropsy shows splenomegaly with 'black berry jam' consistency |

|
|
|
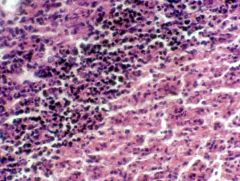
Peracute splenitis caused by anthrax - micro Extensive lymphoid necrosis and depletion within the white pulp Expansion of red pulp with increased clear space indicating oedema Chains of basophilic rods with very few neutrophils or macrophages in the area |
|
|
|
Splenomegaly, pig with haemolytic anaemia (macro) Extremely enlarged and diffusely congested Immune mediated haemolytic anaemia Causes: Babesiosis, Haemobartonellosis (mycoplasma haemofelis infection) |

|
|
|
Immune mediated haemolytic anaemia (micro) Common in dog - idiopathic Immune-mediated attack on rbcs Macrophages proliferate in spleen, remove portions of rbc membranes where Ig attached marked haemosiderin accumulation |

|
|
|
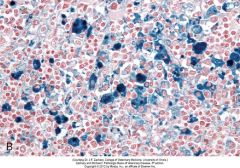
Haemosiderosis, spleen, dog (Not stained) Haemosiderin - golden brown granules in splenic macrophages - product of phagocytosis of large numbers of red blood cells Stain blue by Prussian blue reaction specific for Fe |
|
|
|
Haemosiderosis, spleen, dog (Prussian blue stain) Haemosiderin - golden brown granules in splenic macrophages results of phagocytosis of large numbers of red blood cells Stain blue by Prussian blue reaction specific for Fe |
|
|
|
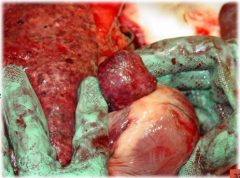
Neonatal isoerythrolysis, foal Immune-mediated haemolytic anaemia Enlarged spleen (S) and liver (L) & very slight jaundice Newborn foal ingested colostrum containing maternal abs which reacted against its own erythrocytes Macrophages in splenic red pulp proliferate & remove erythrocytes whose membranes have bound ab |

|
|
|
Splenic congestion following barbiturate euthanasia, horse (Macro) Spleen enlarged & congested from storage of blood Red pulp vascular spaces markedly distended by blood One focus of white pulp to lower right of microscopic image |

|
|
|
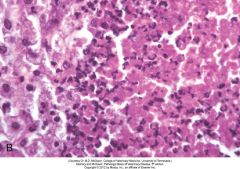
Splenic congestion following barbiturate euthanasia, horse (Micro) Spleen enlarged & congested from storage of blood Red pulp vascular spaces markedly distended by blood One focus of white pulp to lower right of microscopic image |
|
|
|
Hyperplastic nodules (aka nodular hyperplasia) of spleen Incidental - old dogs One or more bulging smooth hemispherical nodules 2-4 cm diameter Composed of both red & white pulp May occasionally rupture – haemoabdomen Cross-section of bulging mass shows intermixed red & white pulp areas composed of rbcs & proliferating lymphocytes |

|
|
|
Haemangioma of spleen Benign tumour of endothelial cells May grow to considerable size May haemorrhage → haematoma |

|
|
|
Haemangiosarcoma of spleen Highly malignant tumour of endothelial cells Solid & blood-filled regions Metastasise & can rupture→ haemoabdomen |

|
|
|
Haemangiosarcoma of spleen (micro) Histopathology reveals haphazardly arranged vascular channels lined by anaplastic endothelial cells. Mitotic figure (arrow). |
|
|
|
Haemic (haemopoietic) neoplasms in spleen (macro) Tumours of blood cell-forming cells arising in bone marrow & resulting in significant No.s of neoplastic cells in bloodstream - leukaemias Diffuse infiltration of sinuses of spleen → diffuse enlargement |

|
|
|
Lymphosarcoma in spleen cross section (macro) Spleen can get involved in lymphosarcoma Neoplastic lymphocytes can cause a multifocal distribution (expanding the white pulp) or more discrete nodules - often detected on ultrasound scan |

|
|
|
Secondary metastatic neoplasia Metastatic carcinoma, spleen, cow Lobulated white soft mass bulges from the cut surface |

|
|
|
Siderofibrosis of spleen (macro) Yellow colour grossly due to haemosiderin (blue microscopically) & bilirubin (orange microscopically) White colour due to presence of calcium & fibrosis Siderotic plaques - opaque pale yellow with roughened texture Typically over capsule and along tip Incidental, often seen on dog spleen Ongoing trauma to capsule – local haemorrhage – fibrous repair & breakdown of heme - haemosiderin & bilirubin |

|
|
|
Siderofibrosis of spleen (micro) Yellow colour grossly due to haemosiderin (blue microscopically) & bilirubin (orange microscopically) White colour due to presence of calcium & fibrosis Siderotic plaques - Incidental, often seen on dog spleen he plaque lies within the fibrous connective tissue of the capsule and consists of haemosiderin (purple) and bilirubin (orange) within fibrous scarring. Ongoing trauma to capsule – local haemorrhage – fibrous repair & breakdown of heme - haemosiderin & bilirubin |
|
|
|
Splenic rupture/ Haemotoma (macro) Subcapsular haematoma, spleen, dog Elevation of capsule from underlying parenchyma by a mass of blood Caused by trauma Sometimes observe fissures as incidental findings are necropsy |

|
|
|
Splenic amyloidosis When amyloidosis generalised (horses, dogs, cats and cattle) Splenomegaly and high fragility - risk of spontaneous rupture |

|
|
|
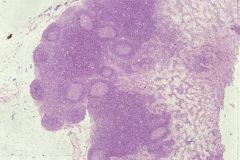
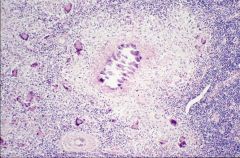
Normal Thymus Lobulated Clear corticomedullary differentiation Prothymocytes from bm ‘home’ to & colonize outer cortex Cortex - selection (proliferation/ apoptosis) and ‘training’ of T-lymphocytes - undergo rearrangement of T-cell receptor genes – ‘randomly shuffling gene segments’ – creates TCR diversity Medulla – removal of auto-reactive T-lymphocytes (thymic epithelial cells express proteins from elsewhere in body) Mature T-lymphocytes migrate to paracortical region of LNs, periarteriolar splenic white pulp & Peyer’s patches |

|
|
|
Lymphocytolysis of splenic lymphocytes in a dog with parvo Can see bits of broken nuclei |
|
|
|
Lymph node, dog (whole picture Micro) Nodal architecture replaced by monotonous sheets of neoplastic lymphoid cells Monomorphic population of atypical lymphocytes that disrupt normal tissue architecture |
|
|
|
Osteosarcoma (malignant osteoblasts) in the humerus of a retriever Mesenchymal tumors Bone, osteoblast, malignant |

|
|
|
Osteosarcoma (outlined) in the distal femur of a St. Bernard. This tumor does not cross the joint space. The proximal tibia (arrow) is unaffected. Mesenchymal tumors Bone, osteoblast, malignant |
|
|
|
Fibroma (fibroblasts) in the hind leg of a beagle Mesenchymal tumors Connective tissue, fibroblast, benign |

|
|
|
Fibroma (fibroblasts) in the subcutaneous tissues of the muzzle in a dog. This tumor is growing by expansion, compressing surrounding tissues, It is not invasive Mesenchymal Connective tissue, fibroblast, benign |

|
|
|
Mammary carcinoma in an Old English Sheepdog Epithelial tumors Malignant, does not form from glands |

|
|
|
Dermal papillomas (keratinocytes) in a cow Epithelial tumors Benign, does not form from glands |

|
|
|
Multiple well-demarcated non-infiltrative papillomas of the lips of a dog Epithelial tumors benign, dos not form from glands |

|
|
|
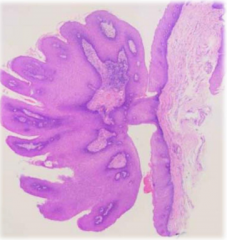
Histology from well demarcated non-infiltrative pailloma of the lips of a dog Shows a pedunculated, exophytic well-differentiated population of cells not arranged in glands |
|
|
|
A well-demarcated non-infiltrative mass developing on the eyelid of a dog is most likely either a sebaceous gland adenoma or a benign dermal melanoma Adenoma = benign, form from glands |

|
|
|
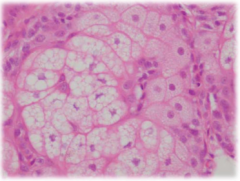
Histology from a well-demarcated non-infiltrative mass developing on the eyelid of a dog Shows a sebaceous gland adenoma with well-differentiated sebaceous cells arranged within well-formed glands |
|
|
|
A well-demarcated non-infiltrative mass in the ventricles of a dog Mmost likely a choroid plexus papilloma |
|
|
|
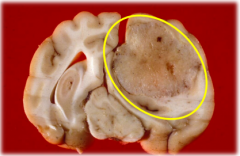
An expansile non-infiltrative mass in the cerebrum of a dog A possible astrocytoma |
|
|
|
A canine oral melanoma is infiltrating into overlaying maxillary bone Most neoplasms initially spread this way Direct invasion |
|
|
|
Canine lung with multifocal metastases from an osteosarcoma originally located in a femur Sarcomas typically spread this way Spread via the vascular system |

|
|
|
Malignant cells (arrow) from an osteosarcoma in the blood vessel of a dog (outlined) Spread via the vascular system |
|
|
|
A prostatic carcinoma has spread to the subinguinal lymph nodes in this dog. Arrow highlights necrotic lymph node Epithelial tumors often metastasize via the lymph to regional lymph nodes Spread via the lymph system |
|
|
|
Enlargement of lymph nodes in this Weimaraner (arrows) In this case the enlargement is due to lymphosarcoma, but they can also be enlarged due to the spread of epithelial tumors Epithelial tumors often involve regional lymph nodes Spread via the vascular system |

|
|
|
Transcoelomic spread Examples: Hemangiosarcomas Ovarian carcinomas Mesotheliomas |
|
|
|
Abdominal mesothelioma in an adult cow Transcoelomic spread |
|
|
|
Abdominal mesothelioma in an adult ewe Note multifocal variably sized nodules and plaques covering most serosal surfaces (arrows) |
|
|
|
Transcoelomic spread of an ovine small intestinal adenocarcinoma Note numerous white metastases overlying the peritoneum of the mesentery and overlying the intestinal serosa |

|
|
|
Histology of transcoelomic spread of an ovine small intestinal adenocarcinoma Shows numerous poorly formed glands adhered to, and infiltrating through, the peritoneum |
|
|
|
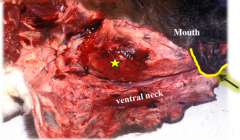
An invasive thyroid carcinoma (star) in-situ a dog |
|
|
|
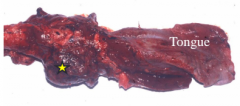
An invasive thyroid carcinoma (star) of a dog after excision |
|
|
|
An invasive hemangiosarcoma in the leg muscle of a dog Note that it would be impossible to locally excise the neoplasm |

|
|
|
Ovine small intestine adenocarcinoma showing anaplasia, poor differentiation and the presence of a cluster of neoplastic cells within a lymphatic vessel (arrow) Microscopic Degree of differentiation |
|
|
|
A leiomyosarcoma of the pulmonary artery found invading the heart Note nuclear atypia, bizarre mitoses, high mitotic rate etc. Smooth muscle, myocyte, malignant |
|
|
|
Osteoma in the nasal cavity of a horse Note that not all benign tumors are clinically silent |
|
|
|
Hemangioma in the skin of a dog Note the reddened areas which are due to the presence of neoplastic blood vessels |

|
|
|
Bovine papilloma virus BPV-1: Papillomas of the skin BPV-2: Papillomas of the urinary bladder BPV-3: Papillomas of the upper GIT Viral oncogenes can initiate tumor formation Factors involved in tumor transformation: intrinsic |

|
|
|
Vaccine induced sarcoma in a cat due to chronic inflammation Macro view and cut-surface of tumor Factors involved in tumor transformation: intrinsic |
|
|
|
Trauma (and chronic inflammation) induced ocular sarcomas are seen in cats Chronic inflammation Factors involved in tumor transformation: intrinsic |
|
|
|
Squamous cell carcinoma on the nose of a cat UV Light - Radiation Factors involved in tumor transformation: extrinsic |

|
|
|
Squamous cell carcinoma removed from the ear pinna of a cat UV Light - Radiation Factors involved in tumor transformation: extrinsic |

|
|
|
Squamous cell carcinomas in the eyes of cattle UV light - radiation Factors involved in tumor transformation: extrinsic |

|
|
|
Cutaneous and genital lesions in water buffalo due to infection with BPV-1 Viruses Factors involved in tumor transformation: extrinsic |
|
|
|
Dermal and genital papillomas and carcinomas in badicoot due to a papilloma virus Viruses Factors involved in tumor transformation: extrinsic |
|
|
|
Cutaneous and corneal fibro-papillomas in a green sea turtle due to CFPHerpes V Viruses Factors involved in tumor transformation: extrinsic |

|
|
|
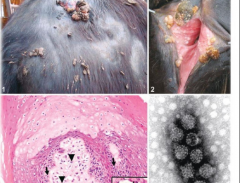
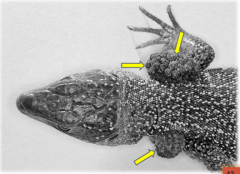
Dermal papillomas in a green lizard due to an as yet unnamed herpes virus Viruses Factors involved in tumor transformation: extrinsic |
|
|
|
Severe fibropapillomas in a cottontail rabbit due to Shope papilloma virus Viruses Factors involved in tumor transformation: extrinsic |

|
|
|
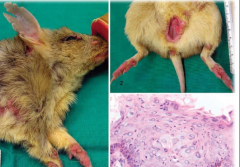
Despite all these tumors being benign, the bulk and weight of these mammary gland fibroadenomas severely affected this rat Effects of neoplasia Disruption of normal tissue |

|
|
|
Even benign neoplasms of the CNS can have severe clinical effects due to compression of the brain or spinal cord Effects of neoplasia Disruption of normal tissue |
|
|
|
Intestinal lipomas in horses can result in intestinal obstruction and death if the pedunculated lipoma becomes wrapped around a segment of intestine The necrotic intestine is dark red Disruption of normal tissue |
|
|
|
Metastases from a colonic adenocarcinoma in the liver of a dog Disruption of normal tissue |

|
|
|
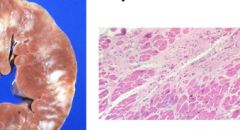
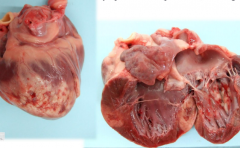
Bovine cardiac lymphosarcomas can infiltrate the myocardium (pale areas) resulting in congestive heart failure or dysrhythmias and death Macro and Micro Disruption of normal tissue |
|
|
|
Lymphosarcoma (pale areas) in a dog's heart Disruption of normal tissue Macro only |
|
|
|
Dog skin Although cutaneous lymphosarcoma rarely spreads from the skin to other organs, the ulcerative lesions become repeated infected, severely decreasing quality of life for the patient Ulceration, haemorrhage, infection Disruption of normal tissue |

|
|
|
Ulcerated mammary tumor in a bitch. Note also the non-ulcerated mammary masses (circled) Mammary carcinomas can have rapid growth, necrosis, and ulceration Disruption of normal tissue |

|
|
|
Sheep skin. Squamous cell carcinomas often result in ulceration, haemorrhage and secondary infection Ulceration, haemorrhage, infection Disruption of normal tissue |

|
|
|
Transitional cell carcinomas of the canine bladder (left) often bleed resulting in hematuria Ulceration, haemorrhage Disruption of normal tissue |
|
|
|
Rectal adenocarcinomas can lead to hematochezia Anemia can occur if bleeding is chronic Ulceration, Haemorrhage Disruption of normal tissue |
|
|
|
An adenoma of pancreatic beta-cells (insulinoma) can result in greatly increased insulin levels and sometimes fatal hypoglycemia even when barely visible Increased function Altered hormone production Disruption of normal tissue |
|
|
|
Thyroid adenomas in cats are common tumors and often result in increased levels of thyroid hormone with resultant clinical effects Increased function Altered hormone production Disruption of normal tissue |
|
|
|
Adenocarcinoma (circled) in a dog's thyroid gland is unlikely to produce thyroid hormone Instead it's more likely ti result in hypothyroidism due to infiltration and destruction of surrounding thyroid gland notice the numerous white metastases (arrows) in the lungs Reduced function Altered hormone production Disruption of normal tissue |
|
|
|
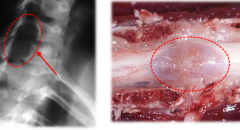
Hypertrophic pulmonary osteopathy in the distal radius of a dog
Circle indicates region of extra osseous growth Paraneoplastic syndromes |

|
|
|
Radiograph of Hypertrophic pulmonary osteopathy in the distal radius of a dog Circle indicates region of extra osseous growth Paraneoplastic syndromes |

|
|
|
Hypertrophic pulmonary osteopathy in P1 of a horse Arrow indicates extra osseous growth Paraneoplastic syndromes |

|
|
|
Section through a dog's kidney which has a lone of calcification at the cortico-medullary function (circled) Hypercalcemia of malignancy Mediated through an osteoclast activity factor or PTH-rP Paraneoplastic syndromes Muscle weakness, anorexia, vomiting Neuropathy (decreased ADH sensitivity) |
|
|
|
Cancer cachexia Likely due to cytokines such as TNF-alpha Not due to increased metabolic demands of the tumor Disproportionately greater loss of muscle mass than loss of body fat Animal anorexic and depressed In veterinary medicine cachexia onset often indicates the appropriate time for eithanasia |

|
|
|
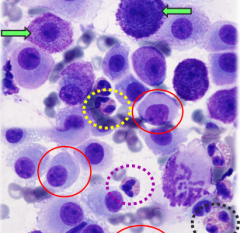
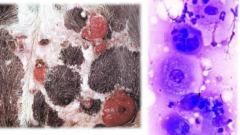
Cytological preparation of an FNA from a Boxer skin lump Note the strongly staining purple granules in the cytoplasm of mast cells (green arrows) Also note that cytoplasmic granules in less well-differentiated mast cells (solid circle) may not stain well Abundant eosinophils are also present (dashed circles) Gross exam: breed Boxers have a strong predisposition in developing mast cell tumors. These can be diagnosed cytologically |
|
|
|
German shepherds are more likely to develop hemangiosarcomas than other breeds Gross exam: breed |

|
|
|
A histiocytoma should always be suspected if a lump develops on a young dog, especially around the head and feet. Cytology should allow for diagnosis An aspirate from a skin lump on a dog shows numerous histiocytes some with mitotic figures (circled) Gross exam: age |
|
|
|
Skin leukosis with generalized lymphadenopathy A lymph node form of sporadic bovine leukosis in cattle usually affects animals <6 months old while the cutaneous form of sporadic bovine leukosis presents mostly in animals 1-3 years old Gross exam: age |

|
|
|
Pituitary pars intermedia dysfunction (PPID) a pituitary tumor which affects horses mainly in their late teens Gross exam: age |

|
|
|
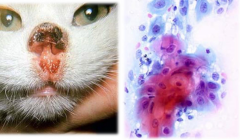
Squamous cell carcinomas commonly develop on the nose and ears of cats (left) The presence of an anaplastic population of keratinizing cells can be confirmed by impression smear (right) Gross exam: location |
|
|
|
Squamous cell carcinomas are the most common tumor in the feline oral cavity |
|
|
|
Melanoma of dog oral cavity Melanomas in the oral cavity of dogs are frequently malignant compared to those in the skin which are more likely to be benign Gross exam: location |

|
|
|
This benign follicular tumor has been traumatized and ruptured resulting in inflammation The inflammatory response may be interpreted as 'rapid growth' Gross exam: Growth rate |

|
|
|
Nasal squamous cell carcinoma which grew faster than the blood supply could sustain resulting in necrosis and ulceration of the tumor Necrosis often due to rapid growth and outstripping of blood supply by malignant tumors. Benign tumors are less likely to have necrosis Gross exam: necrosis |

|
|
|
Canine right atrial hemangiosarcoma with extensive metastases to the lungs If there is a single mass in one organ and lots of masses in another organ then they are likely to be due to malignant/ metastatic tumors Gross exam: number of masses |
|
|
|
Multiple metastatic malignant melanomas in the thoracic cavity of a horse If there is a single mass in one organ and lots of masses in another organ then they are likely to be due to malignant/ metastatic tumors Gross exam: number of masses |
|
|
|
White sun-bathing dogs often develop squamous cell carcinomas on the ventrum (left) Anaplastic keratinocytes are visible cytologically (right) Gross exam: Other factors: Amount of Pigment |
|
|
|
Periocular sqaumous cell carcinomas are much more common in white faced cattle Gross exam: Other factors: Amount of Pigment |

|
|
|
Pancreatic adenocarcinoma The cells are arranged in poorly-formed glands that have little resemblance to normal pancreatic architecture. Microscopic features: differentiation How similar to a normal cell is the neoplastic cell? (better differentiation = less mutation = more likely to be benign) |
|
|
|
Anaplastic sarcoma showing marked variation in cell appearance and size Microscopic features: anaplasia How much variation is there between individual tumor cells? (More variation (anaplasia) = more genetic diversity = more likely to be malignant) |
|
|
|
Anaplastic rhabdomyosarcoma (muscle tumor). Cells dont resemble normal muscle cells at all Microscopic features: anaplasia How much variation is there between individual tumor cells? (More variation (anaplasia) = more genetic diversity = more likely to be malignant) |
|
|
|
Physiological causes of pre-analytical variation Stress produces neuroendocrine changes |
Hemoconcentration (horse, dog) Physiological lymphocytosis (high) (young cats, horses) Mild mature neutrophilia (high), slight monocytosis (high), eosinopenia (low), and lymphopenia (low) |
|
|
Physiological causes of pre-analytical variation Exertion |
Increases CK, LDH, ALT, and AST |
|
|
Biochemistry Profiles: Relations Protein |
Total protein (TP) Albumin (A) Calculated globulins (G = TP - A) Calculated A/G ratio (1/G) |
|
|
Biochemistry Profiles: Relations Renal parameters |
Urea Creatinine |
|
|
Biochemistry Profiles: Relations Metabolites |
Glucose Cholesterol Triglycerides |
|
|
Biochemistry Profiles: Relations Muscle |
Creatine Kinase (CK) Aspartate aminotransferase (AST) (Not specific) Alanine aminotransferase (ALT) (Not specific) |
|
|
Biochemistry Profiles: Relations Liver disease |
Alanine aminotransferase - ALT Aspartate aminotransferase - AST Alkaline phosphate - ALP Glutamate dehydrogenase - GLD Bile acids Bilirubin |
|
|
Biochemistry Profiles: Relations Pancreas |
Amylase Lipase Pancreatic lipase TLI = trypsin-like immunireactivity |
|
|
Biochemistry Profile High Values: ALP, ALT, Bilirubin, Bile acids, Ammonia Low Values: Urea, Cr, Total Protein, Albumin, A/G ratio, Glucose, Ca, Cholesterol |
Severe liver disease - aquired porto-systemic shunt Hypoproteinemia due to hypoalbuminemia, hypoglycemia, hypocholesterolemia, andlow urea indicate marked reduction in biosynthetic function (likely marked decrease in liver mass) Low Cr likely reflects low muscle mass. Low Ca due to low albumin, a major carrier of Ca (free Ca probably ok) Slight to mild hepatocellular injury with cholestasis (ALT, ALP, TB) Markedly impaired detoxification / excretion ammonium Markedly impaired metabolism / excretion of bile acids |
|
|
History: Lethargy, depression, ataxia,vomiting,oliguria Biochemistry Profile High Values: hematocrit, hemoglobin, erythrocytes, leukocytes, neutrophils, phosphate, potassium, glucose, urea, creatinine, total protein, albumin, anion gap Low Values: lymphocytes, calcium, sodium, chloride, A/G ratio, Total CO2 Presence of: Calcium oxalate monohydrate crystals in urinalysis |
Ethylene glycol poisoning (antifreeze) - producing oxalate nephrosis with marked azotemia, hemoconcentration and mild metabolic acidosis Mild hypocalcemia due to hyperphosphatemia and possibly some chelation (by oxalate) Market azotemia (elevated blood urea nitrogen), marked hyperphosphatemia, moderate hyperkalemia due to decreased GFR. With urine unconcentrated this indicates the azotemia is renal Mild hyperglycemia due to stress with mild glucosuria due to exceeding renal threshold Mild hyperproteinemia due to mild hyperglobinemia and slight hyperalbuminemia Mild hyponatremia and moderate hypochloremia likely due in part to renal losses and for Cl, vomiting as well Very high AG due to metabolic acidosis, uremic acids, and possible oxalate crystals or some other related metabolite Mild proteinuria likely due to renal tubular injury as there is no inflammation nor haemorrhage and no evidence for glomerular loss Oxalate crystalluria with renal injury and failure, and high AG, suggest ethylene glycol Mild metabolic acidosis with partial respiratory compensation |
|
|
History: lymph nodes seem enlarged Biochemistry Profile High Values: leukocytes, neutrophils, monocytes, calcium, urea, creatinine, albumin Low Values: Hematocrit, hemoglobin, erythrocytes Presence of: 1-2 granular cats/ high power field (sediment - urinalysis) |
Lymphoma causing psuedohyperparathyroidism with secondary anaemia of chronic disease and renal tubular nephrosis and mild dehydration Mild anaemia Mild leukocytosis due to mild mature neutrophilia with mild monocytosis Marked hypercalcemia Marked azotemia due to decreased GFR. With urine unconcentrated this indicates the azotaemia is renal in origin, likely due to impaired renal tubular concentration by hypercalcemia Mild hyperalbuminemia which can only occur due to dehydration Mild hyperglycemia likely due to renal tubular injury and impairment of glucose absorption Mild hyperglycemia likely due to renal tubular injury and impairment of glucose absorption |
|
|
History: diarrhea, anorexia, weakness, pyrexia, dehydration, hypernea Biochemistry Profile High Values: Hematocrit, hemoglobin, erythrocytes, neutrophil bands, calcium, urea, creatinine, total protein, fibrinogen Low Values: Leukocytes, neutrophil segs, lymphocytes, sodium, Total CO2, Anion Gap, pH, HCO3-, pCO2 |
Salmonellosis causing mild dehydration, moderate to marked inflammation, moderate metabolic acidosis Mild polycythemia & hyperalbuminemia due to dehydration Mild leukopenia due to marked neutropenia with degenerative left shift. Neutrophilia and marked lymphopenia due to stress& azotemia and enteritis Markedhypercalcemia Marked hyponatremia and hypobicarbonatemia due to intestinal fluid loss Moderate to markedazotemia due to decreased GFR Marked hyperfibringoenemia and mild hyperglobulinemia Moderatemetabolic acidosis with partial respiratorycompensation |
|
|
History: anorexia,weakness, pyrexia, clinical dehydration of 7%, circling, ataxia, yawning, pushesagainst objects, muscle quivers, icterus Biochemistry Profile High Values: Leukocytes, neutrophil bands and segments, GGT, AST, SDH, GLDH, LDH, Bilirubin, Bile acids, Ammonia Low Values: None |
Hepatic encephalopathy due to liver failure with moderate inflammation. Mild leukocytosis due to mild neutrophilia with mild left shift, likely associated with hepatocellular injury. Marked cholestasis Marked to moderate hepatocellular injury Marked to moderate hepatocellular and hepatobiliary dysfunction (bilirubin and bile acid uptake and excretion and ammonia detoxification by urea production |
|
|
History: hematuria, clinical dehydration of 8% Biochemistry Profile High Values: Neutrophil segs, total protein, urea, creatinine, firbinogen, sodium, glucose, total CO2, Anion Gap, AST, CK, pH, HCO3- Low Values: lymphocytes, A/G ratio, potassium, chloride Presence of: red, cloudy, protein, glucose, RBC, 1-2 granular casts in urinalysis |
Tubular nephrosis with mixed metabolic alkalosis due to abomasal stasis and metabolic acidosis due to uremia, and hematuria, mild to moderate neutrophilic inflammation, and general systemic stress Mild mature neutrophilia Mild lymphopenia due to stress & azotemia Marked hyperfibringoenemia and mild hyperglobulinemia likely due to renal disease Marked azotemia due to decreased GFR. With urine unconcentrated this indicates the azotemia is renal Moderate to marked hyponatremia and profound hypochloremia likely due in part to renal losses and for Cl, gastric sequestration as well Mild hypochloremic metabolic alkalosis with hypokalemia Mild muscle injury Moderate to marked hematuria. Moderate hyperglycemia and glucosuria due to stress and exceeding renal threshold Moderate renal tubular injury |
|
|
History: anorexia, depression, vomiting, unable to urinate, tense,enlarged abdomen Biochemistry Profile High Values: Neutrphil (segs), phosphate, potassium, glucose, urea, creatinine, ALP, Anion Gap, pH, urine protein Low Values: Sodium, chloride, total CO2 Presence of: reddish brown, cloudy, protein, occult bloodm RBC, 15-20 WBC, triple phosphate crystals, 3+ bacterial rods |
Feline urologic syndrome with hemorrhagic cystitis, mild neutrophilic inflammation, general systemic stress, and mild metabolic acidosis Mild mature neutrophilia Moderate hyperglycemia due to stress Marked azotemia, marked hyprphosphatemia, moderate hyperkalemia due to decreased GFR Mild hyponatremia and moderate hypochloremia likely due in part to sequestration in abdomem and for Cl, vomiting as well. Mild metabolic acidosis causing increased anion gap along with accumulation of uremic acids Moderate to marked hematuria Mild paradoxic alkaluria Moderate septic neutrophilic inflammation |