Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
31 Cards in this Set
- Front
- Back
|
What is a thrombus? |
Pathologic formation of an intravascular blood clot.
|
|
|
Where can a thrombus be formed?
|
In arteries or veins.
|
|
|
What is the MC location of a venous thrombus?
|
Deep veins of the lower limb below the knee.
|
|
|
A thrombus is characterized by what?
|
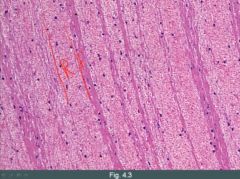
(1) Lines of Zahn
(2) Attachment to vessel wall R: RBC, F: PLT, fibrin |
|
|
On autopsy, you observe a blood clot in the left anterior descending coronary artery. How could you determine if this clot was formed after he died (postmorten clot) or was the cause of his death?
|
Lines of zahn and attachment to vessel wall is not seen in a postmorten clot.
|
|
|
What are the major risk factors for thrombosis?
|
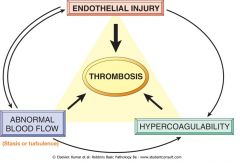
Virchow's triad
(1) Disruption in blood flow (2) Endothelial cell damage (3) Hypercoagulable state |
|
|
What is the normal healthy blood flow pattern called? What is the significance of this pattern of blood flow?
|
Laminar pattern (layered).
It helps keep clotting factors dispersed and inactivated. |
|
|
Provide three examples that abnormal blood flow (of Virchow's triad) can produce thrombosis.
|
(1) Stasis for example. Immobilization increases the risk via stasis of blood.
(2) Cardiac wall dysfunction. A-fib. Atrium is not moving properly and blood is gonna become more static. (3) Aneurysm. (Balloon-like dilatation of a portion of the blood vessel). The pocket is going to disrupt laminar flow, causing irregular flow and increase the risk of thrombus formation. |
|
|
Why does endothelial damage increase the risk for thrombosis?
|
Because the endothelium is highly protective against the formation of a thrombus.
|
|
|
What does the endothelium do to protect against the formation of thrombosis?
|
(1) It's a barrier, hiding away subendothelial collagen and tissue factor.
(2) PGI2 (prostacyclin) synthesis. Blocks PLT aggregation. (3) NO causes vasodilation. (4) Heparin-like molecules. Activate antithrombin III, inactivates thrombin. (5) tPA, converts plasminogen to plasmin. (6) Thrombomodulin, takes thrombin and modulates its activity to activate protein C, which inactivates V and VIII. |
|
|
Plasmin cleaves what?
|
(1) Fibrin, fibrinogen
(2) Clotting factors (3) Blocks platelet aggregation |
|
|
How is PGI2 and plasmin similar in their effect?
|
Plasmin has many roles, but one of them is to block PLT aggregation, which is the role of PGI2.
|
|
|
What are some examples of endothelial damage?
|
(1) Atherosclerosis.
(2) Vasculitis (3) High levels of homocysteine |
|
|
What inherited enzyme defect can cause an increase in the risk of thrombosis? What are its inheritance pattern?
|
Homocystinuria (Cystathionine beta synthase deficiency; CBS). AR. Deficiency of cystathionine synthase which combines homocysteine with serine to create cystathionine.
|
|
|
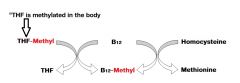
What are the ways by which we can have elevated homocysteine?
|

(1) Vitamin B12 or folate deficiency.
- Can no longer convert homocysteine to methionine |
|
|
Draw a simplified scheme of the role of B12 in the body (one of its roles).
|
|
|
|
What is the life expectancy for patients with CBS?
|
They usually die at a young age
|
|
|
CBS deficiency is characterized clinically by [...]
|
(1) Mental retardation
(2) Vessel thrombosis (3) Lens dislocation (4) Long slender fingers |
|
|
How can you achieve a hypercoagulable state?
|
Due to excessive procoagulant or defective anticoagulant proteins.
|
|
|
What is the classic presentation of a person with a hypercoagulable state?
|
They tend to have recurrent DVTs and DVTs at a young age.
|
|
|
In a person with a hypercoagulable state, what other sites than the deep veins of the legs would clots occur?
|
Hepatic and cerebral veins
|
|
|
Lack of what natural endogenous anticoagulants can create a hypercoagulable state? Elaborate.
|
Protein C and S deficiency.
(1) They normally inactivate V & VIII. (2) Decreased negative feedback on coagulation cascade. (3) Patients become hypercoagulable. |
|
|
In protein C and protein S deficiencies, there is an increased risk for what?
|
Warfarin skin necrosis.
- The transient initial window of hypercoagulation is more severe in these patients when they already have low levels of C and S and warfarin transiently makes it worse. |
|
|
In warfarin therapy, what are the first factors to be degraded due to their shorter half life? What is the consequence?
|
Protein C and protein S. A transient hypercoagulable state.
|
|
|
What is factor V leiden?
|
Patients have a mutated form of factor V. This makes it resistant to cleavage by protein C and protein S.
|
|
|
What is the MC inherited cause of hypercoagulable state?
|
Factor V leiden
|
|
|
This disease is caused by a point mutation in prothrombin. What is it?
|
Prothrombin 20210A. Results in increased gene expression. Promotes thrombus formation.
|
|
|
This disorder induces a hypercoagulable state. It is caused by a deficiency in an anticoagulant that is normally enhanced by heparin-like molecules from endothelial cells. What is it?
|
Antithrombin III deficiency. Decreases the protective effects of heparin-like molecules produced by endothelium, increasing the risk for thrombosis.
|
|
|
A patient has a hypercoagulable state. You administer heparin at standard dosing. Later you note that his PTT has not increased. What is going on?
|
Antithrombin III deficiency.
|
|
|
In ATIII deficiency you have to give ____________ (low/high) doses of heparin to increase PTT.
|
high
|
|
|
What drug used by sexually active women can cause a hypercoagulable state? Why does this happen?
|
Oral contraceptives.
Estrogen induces increased production of coagulation factors and increases the risk for thrombosis. |