![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
301 Cards in this Set
- Front
- Back
|
What is a pediatric patient? |
From birth to 18 and sometimes to 21 |
|
|
Why are bones difficult to see on x-ray in the pediatric patient? |
bones grow from the epiphyseal plates which tend to be radiolucent (on x-ray - can’t see it on image) |
|
|
How do renals appear different on ultrasound in a pediatric patient? |
kidneys look very unique when dealing with a newborn or baby - up to age 10 you can see significant changes. |
|
|
What percentage of patient acquire an infection in the hospital (nosocomial)? |
10-15% |
|
|
How might someone acquire a nosocomial infection? |
Many microorganisms, patients weakenedimmune system, transmission train through thestaff, the equipment, therapeutic aids and foodservices can cause urinary tract infections, pneumonia, diarrhea, or a surgical wound infection. |
|
|
Why is tissue matching for transplant not as important in the pediatric patient? |
Matching tissue for transplant is not asessen6al in young infants or neonates basedon immature immune systems- but supressedchildren are highly susceptible to pathogens(gown, mask, glove and clean machine) |
|
|
Why is a child resistant to the same things that their mother is resistant to? |
Maternal antibodies can cross the placenta and therefore children tend to have more resistance to things that mom has been immunized for - protects the baby for a while |
|
|
What percentage of infants are affected by necrotizing entercoccus colitis? |
90 % Preterm infants weighing less than1500gms; 10% term infants |
|
|
What is the cause of NEC? |
Exact cause unknown but risk factors:asphyxia, UA catheterization, patent ductusarteriosus, polycythemia, enteral feeding,indomethacin (NSAID), vitamin e andxanthines (mild s6mulant and bronchodilator) |
|
|
What is NEC? |
Reduced perfusion of the intestinal wallleading to ischemia, hypoxia, necrosis andgangrene- mucosa or submucosa ->superficialinvolvement or through wall causingperforation can lead to peritonitis. |
|
|
What area of the bowel is most affected by NEC? |
Ileum most affected, then ascending colon,cecum, transverse colon and recto sigmoid |
|
|
What are the symptoms of NEC? |
Abdominal distention, gastric aspirates,bilious stools, lethargy, apnea and poorperfusion- infant appears septic |
|
|
What will the ultrasound of a NEC patient look like? |
Pneumatosis intestinalis-intramural air, gasless abdomen can indicateperitonitis, free air with a perforation,potentially hyperechogenic pericholecystic area,air in liver |
|
|
Why might a child require an urgent ultrasound? |
• Intussusception • Appendicitis • Inflamed bowel • Bowel obstruction • Ovarian/testicular torsion • Septic hip • Obstructive hydronephrosis • Acute bleed • thrombus • Pyloric Stenosis |
|
|
What kinds of tools can be used to help scan a baby? |
Special smaller transducers with high resolution, isolettes, cribs, strollers, or wheelchairs |
|
|
What are some red flags in blood work results? |
Drop in hematocrit, WBC increase, bilirubin increase, creatinine increase, increased or low BUN. |
|
|
What is the most common location for brain hemorrhage? Where would this bleed be found in the brain? |
The germinal matrix - involved in brain development (and gives rise to the choroid plexus) in the lateral ventricles - it is really vascular and extensive in early gestation (if any pressure in the area will cause a bleed)If this area bleeds the blood can be found in the ventricle or in the caudothalamic groove (area between caudate nucleus and thalamus) |
|
|
What does the lamboid suture separate? |
The occipital and parietal bones |
|
|
What are the fossae of the brain and what do they include? |
The anterior, middle, and posterior cranial fossa |
|
|
How many bones make up the skull? |
Made up of 8 bones: 2 temporal, 2 parietal, one frontal, one occipital, one sphenoid and one ethmoid. |
|
|
What is the petrous process? |
Petrous process is part of the temporal bone. |
|
|
What are the parts of the temporal bone? |
The left and right temporal bones are on the sides of the cranium. Each of them consists of several parts. The squamous portion of the bone extends upward to make up part of the cranial wall surrounding the brain. Projecting medially from the base of the temporal bone is the petrous portion. When writing out the name of the temporal bones, you should always include the side (right or left) as part of the name. |
|
|
What fontanelle is most commonly used for neonatal neuro imaging? |
The anterior fontanelle (posterior is used when there is flare - bright white matter tracks) |
|
|
For how long can the anterior fontanelle be used as an imaging window? |
Anterior fontanelle remains open through the first yr of life. RWC 4th ch 48 49. after the closure 3 windows can be used. Trans temporal, orbital, foramen magnum. |
|
|
What are the fontanelles of the cranium? |
Anterior (12-14 mths good scanning window), posterior, posterolateral (mastoid), and anterolateral (sphenoid/temporal). |
|
|
What are the sutures between the fontanelles? |
Metopic (frontal), lamboidal, coronal, sagittal, and squamosal. |
|
|
What is the term used to describe a premature fusion of thesutures in the skull? |
Craniosynostosis |
|
|
What are the meninges of the brain? |
Dura mater (outer - tough mother), arachnoid, and pia mater. |
|
|
Explain the dura mater. |
A double layer: periosteal and meningeal, that encases the veins (venous sinuses), which creates the falx cerebri, cerebelli, and tentorium. This is the strongest layer, and located between its two layers are meningeal arteries and dural sinus-venous drainage of the brain. Folds of dura provide cushioning for the brain and separate structures (cerebri and tentorium). |
|
|
Explain the arachnoid. |
This is spiderlike and creates the subarachnoid space, and contains the cisterns (CSF pools), and the arachnoid villi. This is a delicate, transparent membrane that is separated from the dura by a potential space (subdural space). The arachnoid follows the contour of the dura - vessels fill this space. |
|
|
Explain the pia mater. |
A highly vascular and delicate structure that touches the surfaces of the brain and adheres to its contour. The name means tender mother and it is separated from the arachnoid membrane by the subarachnoid space which is where the CSF circulates around the brain and the spinal cord - protection. |
|
|
What are the 4 locations where dura extends deep into the cranial cavity? |
- Falx cerebri (separates cerebral hemispheres) - Tentorium cerebelli - Falx cerebelli - Diaphragma sellae |
|
|
What is the diaphagma sellae? |
Diaphragma sellae- lines sella turcica of the sphenoid bone. Dura attaches to the sella and ensheaths the pitutary gland. |
|
|
What is the falx cerebri? |
A fold of dura mater which projects between the cerebral hemispheres in the longitudinal fissure. It attaches to the crista galli inferiorly and the internal occipital crest and tentorium cerebelli posteriorly. Both the inferior sagittal sinus and superior sagittal sinus travel in this dural fold - largest fissure in the brain. |
|
|
What is the crista galli? |
Part of the ethmoid bone |
|
|
What is the cribiform plate? |
The cribriform plate is received into the ethmoidal notch of the frontal bone and roofs in the nasal cavities. Projecting upward from the middle line of this plate is a thick, smooth, triangular process, the crista galli, so called from its resemblance to a cock’s comb |
|
|
What is the tentorium cerebelli? |
Separates and protects the cerebellar hemispheres from those of the cerebrum. It extends across the cranium at right angles to the falx cerebri, and the transverse sinus lies within the tentorium cerebelli. |
|
|
Where is the straight sinus? |
The straight sinus (sinus rectus; tentorial sinus) is situated at the line of junction of the falx cerebri with the tentorium cerebelli. It is triangular in section, increases in size as it proceeds backward, and runs downward and backward from the end of the inferior sagittal sinus to the transverse sinus of the opposite side to that into which the superior sagittal sinus is prolonged. Its terminal part communicates by a cross branch with the confluence of the sinuses. Besides the inferior sagittal sinus, it receives the great cerebral vein (great vein of Galen) and the superior cerebellar veins. A few transverse bands cross its interior. |
|
|
What are the 2 main fissures of the cerebrum? |
The longitudinal fissure (falx and SupSagSin), and the lateral (sylvian) fissure |
|
|
What is the sylvian fissure? |
A deep furrow that separates thetemporal and the parietal lobes ofthe cerebrum. MCA located herealong with many other vessels |
|
|
When a child has a bleed in the brain- how can you tell if it issubdural or sub arachnoid in nature? |
Throw colour Doppler on- with a subarachnoid hemorrhage you willsee the small intricate vessels with, where a subdural hemorrhagewill compress the subarachnoid vessels |
|
|
What are gyri and sulci? |
Folds on the brain. Gyri are the areas that project out and sulci are the grooves. These develop as a brain matures and as brain tissue becomes more expansive. |
|
|
What is the largest portion of the brain? |
The cerebrum - original forebrain in development (right and left hemispheres) |
|
|
How many lobes are within the cerebrum? |
5: frontal, parietal, temporal, occipital, insula. |
|
|
What fissure is the first to be seen? |
the sylvian fissure |
|
|
What is the calcalrine fissure/when can it be seen? |
A straight line in the midline sagittal images seen at 20 weeks. |
|
|
When is the occipitoparietal fissure seen? |
24/25 weeks |
|
|
When is the callosomarginal sulcus seen? |
by 28 weeks seen over the corpus callosum |
|
|
When is the cingulate sulcus seen? |
by 28 weeks over the corpus callosum superior and lateral |
|
|
By what time will you see folds coming off of the cingulate sulcus? |
30 weeks, by 33-40 weeks we can see multiple bends and folds. |
|
|
What are the names of the main sulci of the brain? |
central, callosal, cingulate, calcarine, and parieto-occipital |
|
|
What is the cingulum? |
The cingulum is a collection of white matter fibers projecting from the cingulate gyrus to the entorhinal cortex in the brain, allowing for communication between components of the limbic system. |
|
|
What parts of the brain relate to the fore, mid, and hind-brain? |
• Cerebrum- forebrain • Midbrain- mid brain • Cerebellum, pons, and medulla - hindbrain |
|
|
What are the structures formed by the diencephalon? |
The thalamus, hypothalamus, and epithalamus |
|
|
What is the "Island of Riel"? |
Part of the insula - The insular cortex is a complex structure which contains areas that subserve visceral sensory, motor, vestibular, and somatosensory functions. The role of the insular cortex in auditory processing was poorly understood until recently. |
|
|
What is the operculum? |
The second part of the insula - covers the insula |
|
|
Where is the primary motor area? |
The frontal lobe |
|
|
Where is the sensory cortex? |
The parietal lobe (posterior to the central sulcus) |
|
|
Where are the auditory and olfactory areas? |
The temporal lobe |
|

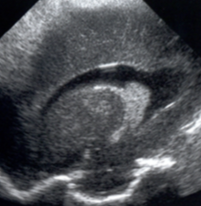
What would we be concerned with if we saw this image? |
A hypoxic event causing edema (brain draws fluid in) - the bright then hypoechoic appearance is not normal. |
|
|
What is white matter? |
White matter is brain tissue that glistens due to fat in the myelinated axons in a lipid and protein sheath. |
|
|
What does grey matter contain? |
neuron cell bodies and unmyelinated axons, neuroglia, etc. |
|
|
What are the 3 dimensions of white matter tracks? |
Commisures: from side to side (corpus callosum, ant/post commisures) Associations: longitudinal front to back (links cortical area within the hemispheres) Projections: Up and down (corticospinal tract, spinothalamic tract, internal capsule, and corona radiata - centrum semiovale) |
|
|
What is the fornix? |
A c-shaped pathway for the limbic system and connects to the hippocampus. The fornix is white matter that lines the lateral walls of the CSP. |
|
|
What is the internal capsule? |
A great projection tract that pierces the basal nuclei to for the corpus striatum. They are white matter tracts that run between the nuclei of the basal ganglia. |
|
|
What does the corpus callosum form with? |
The septum pellucidum and the fornix |
|
|
At what level does the falx stop, and why is this structure important? |
It stops at the corpus callosum and this is important because it is the largest neural commisure. |
|
|
What is the cavum septum pellucidum? |
Cavum is the space, the midline anechoic area which closes back to front, also includes the cavum vergae and the cavum veli interpositi. |
|
|
What is the cavum velum interpositi? |
Cavum Velum Interpositi: a small potential space that may be seen above the choroid plexus of the 3rd ventricle, below the columns of the fornices - it may look like an inverted helmet inferior to the splenium |
|
|
What parts of the brain make up the grey matter? |
The cortex, and the basal nuclei |
|
|
What are the 4 types of basal nuclei? |
Caudate, lentiform (putamen and globus pallidus), amygdala, and claustrum - they are relays. |
|
|
What are basal nuclei? |
The term for grey matter deep in the cerebrum, also called basal ganglia. These support our motor control |
|
|
What is the corpus striatum? |

Has 3 parts: (1) Fibres of Internal capsule (2) Caudate Nucleus (3) Lentiform |
|
|
What are the parts of the caudate nucleus? |
![The head (inferolateral border of AH), body and tail - c-shaped which bends and tapers around the thalamus (ends in the amygdala near the hippocampus [red arrow]).](https://images.cram.com/images/upload-flashcards/59/75/70/18597570_m.png)
The head (inferolateral border of AH), body and tail - c-shaped which bends and tapers around the thalamus (ends in the amygdala near the hippocampus [red arrow]). |
|
|
What does the amygdala control? |
memory, emotional associations, fear, pleasure |
|
|
What is the lentiform nucleus? |
The globus pallidus (medial) and putamen - lens shaped. |
|
|
What is the claustrum? |
• Lateral to lentiform at insula • Thin layer of gray substance that is just belowthe insula • External capsule (white matter tracts) separates claustrum from the more medial lentiform |
|
|
Learn this image. |

|
|
|
What is the massa intermedia? |
The connection between the thalami and goes through the third ventricle - when third ventricle has fluid in it then we can see this really well indicating that we are in the middle of the third ventricle |
|
|
What are the parts of the forebrain - diencephalon? |
This is in-between brain buried grey matter 1. Thalamus(2 lobes, connected by massa intermedia)-relays sensory messages** 2. Hypothalamus- floor of the 3V, temp. Regulation ** 3. Epithalamus - roof of 3V. Membranous portion hastela choroidea (fold of pia mater). Pineal gland (body cycles, circadian rhythms) |
|
|
What makes up the midbrain? |
- Cerebral peduncles - "little feet" (paired white matter tracts, internal capsule above, pons below, the interpeduncular cistern lies btw toes) - Quadrigeminal bodies (colliculi - superior and inferior - sensory nuclei) - Cerebral aqueduct (3rd to 4th ventricle - narrowest part of the ventricular system - common for clot) |
|
|
What anatomy is anterior to the cerebral peduncles? |
Circle of Willis and the interpeduncular cistern |
|
|
What anatomy is posterior to the quadrigeminal bodies? |
The quadrigeminal cistern |
|
|
What makes up the hidbrain? |
(1)Pons (belly, pontine cistern anterior, 4th ventricle posterior) (2)Medulla Oblongata (decussation of projection tracts - continuous with spinal cord below) |
|
|
Explain the cerebellum. |
The little brain - white matter with grey cortex at the surface - two hemispheres divided by a falx cerebelli, covered by tentorium. Centrally there is an arbor vitae (tree of life), and a vermis. There are 2 tonsils (Chiari II malf), 3 pairs of cerebral peduncles, and the 4th ventricle within (*dandy walker malf) - foramen of lushka, and magendie to pontine cistern. Pons are for balance and coordinated movement. |
|
|
What are the cerebellar peduncles? |
3 pairs: superior (midbrain/thalamus), middle (pons, largest), and inferior (medulla oblongata). They function for posture and balance, plus skilled movements like scanning! |
|
|
What does the brainstem include? |
Midbrain, pons, and medulla oblongata. |
|
|
What are ventricles? |
Vessels that contain CSF |
|
|
What are the 4 ventricles? |
1. Lateral ventricles (2) – right/left – inter-ventricular foramen [of Monro] to 2. Third Ventricle – Aqueduct [of Sylvius] narrowest point (cerebral aqueduct) 3. 4th Ventricle – 3 Foramina [of LUSCHKA(2 lateral) &MAGENDIE(medial)] to cisterns & centralcanal of spinal cord – Foramina are Lateral and Median |
|
|
What are the parts of the lateral ventricle? |
anterior, temporal, and occipital horns. The trigone connects the 3 horns |
|
|
What is contained within the trigone? |
Contains the glomus of the choroid plexus - the most CSF is produced here - widest point of the ventricular system. |
|
|
Where do the choroids taper? |
Anteriorly at the caudothalamic grooves within the temporal horns. |
|
|
Where should we not see choroid? |
In the occipital horn (if seen here then it is a bleed) |
|
|
What are the borders of the anterior horns? |
Medial: septum pellucidum Lateral: head of caudate nucleus Superior: corpus callosum |
|
|
What are some possible pathologies of the anterior horns of the lateral ventricles? |
Frontal horn cysts, coarctation of the frontal horns, connatal cysts, or septations caused by the frontal horn folding in on itself |
|
|
What is the cavum septum pellucidum? |
A continuous cystic midline structure in the fetal life, which closes from back to front (back portion is called the cavum septum vergae). |
|
|
What is the cavum veli interpositi? |
This is above the roof of the 3rd ventricle and below the fornix. It is anechoic and helmet like inferior and posterior to the splenium. |
|
|
How big is the third ventricle? |
only 2mm - thin, but long and deep. |
|
|
What are the recesses of the third ventricle (4 + 1 area not a recess)? |
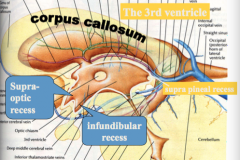
1. optic recess 2. infundibular recess 3. suprapineal recess 4.pineal recess plus - massa intermedia of thalamus |
|
|
When is the third ventricle seen well? |
Only in ventriculomegaly (hydrocephaly or brain atrophy) |
|
|
What connects the third to the fourth ventricle? |
The cerebral aqueduct or aqueduct of sylvius |
|
|
Explain the fourth ventricle. |
It is diamond-shaped and fits into the vermis of the cerebellum (echogenic choroids blend in and can't be seen). The 4th ventricle drains into the foramina of Luschka and Magendie, which allows CSF to flow into cisterns and sub-arachnoid spaces around the brain and cord. This is continuous with the spinal canal below. |
|
|
Where is the mastoid fontanelle? |
you mastoids are located right behind your ears (lump) - acts as a window in youth to look at the 4th ventricle and cerebellum, but you can sweep up and look at the occipital horns |
|
|
In what ventricles can you see the delicate vascular choroid plexus? |
The lateral and third, but not the fourth since it blends in. |
|
|
What covers the choroid plexus? |
A single layer of ependymal cells |
|
|
What are choroids an essential part of? |
The blood brain barrier - membrane permiability, prevents bacteria from crossing into the brain. |
|
|
What is the blood supply for the choroid plexus? |
A dual blood supply: anterior and posterior choroidal arteries |
|
|
What is the blood drainage for the choroid plexus? |
Vein of Galen, sinuses, and jugular vein |
|
|
Where do the right and left choroid join? |
The foramen of Munroe |
|
|
What is the tela choroidea? |
The "end" of the choroid, where choroid bends in - a thin delicate layer of pia mater on the roof of the third ventricle |
|
|
What is the germinal matrix? |
Consists of loosely arranged proliferating cells that give rise to neurons and glia of the cerebral cortex and basal ganglia. It develops below the ependymal lining of the ventricles. This is found near the foramen of Munroe and caudate nucleus (CT groove) |
|
|
When is there a high risk of hemorrhage to the germinal matrix? |
At 24-30 weeks, and the GM gradually recedes and there is lower risk >32 weeks. |
|
|
How do cisterns appear on ultrasound? |
They form echogenic landmarks, except the cisterna magna, which appears anechoic. |
|
|
What are the subarachnoid cisterns? |
Quadrigeminal cistern (superior) - vein of galen, Ambient and interpeduncular cistern, supracellar cistern (at sela turcica - COW), pontine cistern (ant to pons), lateral cisterns in sylvian fissure, and the lumbar cistern. |
|
|
What is cerebrospinal fluid? |
Extra-cellular fluid but with higher Na, lower glucose, and K |
|
|
How much CSF do people produce in a day? |
500-600 ml in adults, and there may be only 100 ml in an infant at any given time. |
|
|
What is the normal CSF pressure? |
130mm water/ 10mm Hg |
|
|
How is CSF reabsorbed? |
Through arachnoid granulations to return to venous flow in superior sagittal sinus. |
|
|
What is the function of CSF? |
Cushions and protects cortical surface, maintains stable ionic concentrations (synapses), and moves waste into the venous system. |
|
|
What are the types of ventriculomegally? |
(1) Hydrocephaly - under pressure from CSF from blocked aqueduct or arachnoid granulation (2) Colpocephaly - malformations cause enlarged lateral ventricles (occipital) - Chiari II, ACC, DW (3) Atrophy of the brain - passive expansion of the ventricles as the brain shrinks |
|
|
What might indicate that there is a blocked aqueduct? |
The absence of the 4th ventricle while the 3rd ventricle is well seen. |
|
|
What arteries supply the brain? |
Vertebral arteries (post supply), basilar arteries, and internal carotids (ant supply). |
|
|
Where do the vertebral arteries come from? What are their main branches? |
The vert arteries come from the subclavian arteries through the transverse processes of the vertebral bodies and enters the cranium through the foramen magnum. Notable branches include the spinal arteries and the cerebellar artery. |
|
|
Where does the basilar artery come from? What are its notable branches? |
Created by the right and left vertebral arteries. Notable branches include 2 more cerebellar arteries and the posterior cerebral arteries. |
|
|
Where does the internal carotid artery come from? What are its notable branches? |
The ICA is a branch off the CCA, and enters the cranium through the carotid foramen in the temporal bone. Notable branches include: ant cerebral arteries (lt and rt), and the MCA (largest branch that feeds the lateral lenticulostriate branches) |
|
|
What arteries do the anterior cerebral arteries branch into? |
Pericallosal, callosomarginal, and medial lenIculostriate arteries. |
|
|
What does the anterior cerebral artery supply? |
Frontal lobes, and medial surfaces |
|
|
What does the middle cerebral artery supply? |
The basal nuclei, lateral surface ofcerebrum, insula white matter tracts, cortex oftemporal & parietal lobes+ anterior choroidal artery |
|
|
What does the posterior cerebral artery supply? |
The occipital lobe, visual areacerebral peduncles and+ posterior choroidal artery |
|
|
Why is the circle of Willis so important? |
This is an incredibly important anastomosis that ensures that the brain is always receiving blood and allows collateral circulation between the hemispheres. |
|
|
What vessels form the circle of willis? |
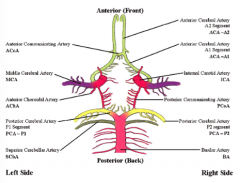
The anterior cerebral artery, posterior cerebral artery, ICA, and the ant/post communicating arteries. |
|
|
Where is the COW located? |
Mainly in the suprasellar cistern |
|
|
What is venous drainage of the brain like? |
(1) Cortex to the venous sinuses (superior or inferior sagittal sinus) (2) Deep - MCA territory to straight sinus via: - thalamostriate v. and choroid v. - Internal cerebral veins - Great cerebral vein (of Galen) - straight > transverse > sigmoid > internal jugular vein through the jugular foramen. |
|
|
On a mid-sagittal view, what vasculature can we see? |
– basilar art – internal caroId ICA– anterior cerebral – internal cerebral v’s– Vein of Galen– superior sag sinus– straight sinus |
|
|
On an anterior coronal view, what vasculature can we see? |
• ICA & branches• MCA• Lenticulostriate art’s• ACA branch intopericallosal art’s• Supra-sellar cistern |
|
|
What are some alternate windows for the vasc of the brain other than the anterior fontanelle? |
Sphenoid (ant-lat) fontanelle (MCA and COW), and the mastoid fontanelle (transverse sinus) |
|
|
During hydrocephalus what will perfusion to the brain look like? |
Increased PI due to decreased perfusion |
|
|
What might the brain hemodynamics look like when the patient is on mechanical ventilation? |
It is hard to get true arterial waveforms based on the fact that the pressure changes are being caused my mechanical ventilation , and not from its own body. Impeded venous return causes flow reversal. |
|
|
Why might extra-corporeal membrane oxygenation (ECMO) cause altered hemodynamics? |
This occurs in term infants with acute respiratory failure - cannulation and ligation of the CCA and jugular vein = non-pulsatile partial cardio-pulmonary bypass |
|
|
What will the waveforms look like in a patient undergoing ECMO (pt with CDH or cardiac dysfunction)? |
pump is pumping the blood through at a constant level, there is no systole or diastole - pulsatility disappears. Arterial shunting across the circle of willis and venous drainage is altered. |
|
|
What are ECMO patients at high risk for? |
Hemorrhagic Infarction - unsuitable for premature infants - heparin + germinal matrix = high risk. |
|
|
What does the nervous system develop from? |
The neural plate - derivative of the ectoderm |
|
|
When does neurulation begin? What is it? |
early in the 4th week (~22-23 days) Neurulation-formation of neural plate and neural tube. |
|
|
How does fusion of the neural folds proceed? |
In cranial and caudal directions until only small openings remain at both ends (cranial opening = rostral, caudal = caudal). |
|
|
What does closure of the neuropores coincide with? |
The establishment of a blood circulation for the neural tube (cranial neuropore closes at the 25th day, and caudal closes at the 27th day). |
|
|
What is the diagnostic checklist for a neonatal head scan? |
(1) Establish gestational age (2) Go over diagnostic checklist: ventricles, parenchyma, pulsation, and extra-axial spaces. |
|
|
If we note sulci and gyri but can't see them very well, what may be wrong? |
The brain cortex is very echogenic |
|
|
Do sulci and gyri patterns change with age? |
Yes, they develop more as the child ages. |
|
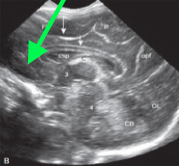
What is the green arrow pointing too? |
The sela tursica (the cow surrounds it) |
|
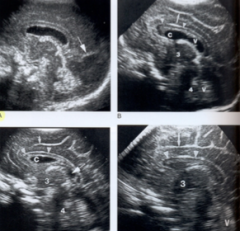
What's the difference in these images? |
A- 25 wks gestation. No sulci. CC lies above completely cystic csp and cavum vergae. Arrow pointing to occipito-parietalfissure. B- 27 wks. Cingulate just developed C- 30 wks cingulate sulcus has few branches. Cavum velum interpositum long arrow. Cavum velum int=potential space above the roof of 3V and below the columns of fornices -anechoic space inferior and post to splenium in the pineal region D- 40 wks cingulate sulcus has many branches CSP no longer cystic |
|
|
Why does peritrigonal blush occur? |
Because of anisotropy. Peritrigonal blush- echogenic whiter matter tracts coursing from the deep white matter towards the cortex and also could be due to the blood vessels. |
|
What is wrong with this image? |
Bulky Choroids |
|
|
What is the calcar avis? |
a projection on the medial wall of the posterior horn of the lateral ventricle of the brain. It is associated with the lateral extension of the calcarine fissure. |
|
|
What is the operculum? |
It hides the insula - Opercula means= a lid formed by growth and elongation of the cerebral lobes forming a lid or flap which covers the insula. Lack of opercularization associated with lissencepahly. |
|
|
When can the insula be visualized? |
In premature infants, before the growth and proliferation of sulci and gyri, insula may be viualized. However, it term infants-it is not visualized. |
|
|
How many coronal images should be taken? |
Minimum 6-8 using the anterior fontanelle window - for symmetry |
|
|
What is the centrum semiovale? |
A portion of the white matter tracts deep to the grey matter. |
|
|
What are the normal variants of the ventricles? |
Bulky choroids, lobulated choroids, or a clot indicating intraventricular hemorrhage. |
|
|
In what percent of infants can the cavum velum interpositum be seen? |
21% - uncommon by 2 years |
|
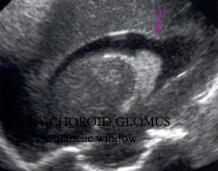
What is the purple arrow pointing too? |
The calcar avis |
|
|
How many Chiari malformations are there? When were they discovered? |
In 1890 Chiari identified malformations I - IV |
|
|
What is the etiology for Chiari II? |
Abnormal neural tube closure may result in a spinal defect such as a myelomeningocele* - decompresses ventricles and a small posterior fossa developes. |
|
|
Which Chiari malformation is the most common? |
II |
|
|
What is Chiari I? |
Chiar-1-downward displacement of tonsil without the displacement of 4 V or medulla. |
|
|
What is Chiari III? |
Chiari 3- associated with a high cervical encephalocele in which medulla, 4th ventricle and entire cerebellum reside. |
|
|
How will Chiari II malformation affect the ventricles? |
- 4th ventricle is not visible: compressed - 3rd ventricle is very visible but the massa intermedia is enlarged - lateral ventricles have a classic shape: colpocephaly-occipital horns, batwings-frontal horns - Hydrocephaly especially after meningomyelocele repair (98% have progressive communicating hydro that gets worse after closure of the spinal defect - may be fenestrated) |
|
|
What are some other sonographic appearances of Chiari II? |
- Parenchyma: herniated cerebellar tonsils, meningomyelocele - Inferior displacement of brainstem & vermis ofcerebellum (dysplastic/displaced cerebellum - banana sign, and tentorium) - Hypoplastic corpus callosum (wide longitudinal fissure, esp after shunting) |
|
|
When is normal development of the corpus callosum? |
8-18 (20) weeks |
|
|
Is ACC complete or partial? |
It can be either |
|
|
Why is fetal diagnosis of ACC important? |
Because 80% of patients will have other anomalies such as Chiari II, DW, lipoma, holopros, hydro, arachnoid cysts, etc. |
|
|
What chromosomal anomalies are associated with ACC? |
8, 13, and 18 (also teratogens are associated) |
|
|
What part of the corpus callosum develops first? |
The genu and anterior body, the rostrum and the splenium develop late - so if ACC is partial these two will be missing |
|
|
When is the corpus callosum completely formed? |

at 22 weeks |
|
|
What are the sonographic appearances of ACC? |
The Ventricles - widely spaced (parallel choroids),narrow anterior horns, abs septi pellucidi – colpocephaly - large occipital horns (teardrops)– dilated 3rd ventricle may rise between lat vent’s The Parenchyma - “sunburst” radial sulci– absent cingulate gyrus– CFD may help Diagnosis - Ant Cerebral Art is missing! • Probst bundles - callosal fibres remain inlongitudinal “bundles”, no migration across midline • Lipoma - echogenic mass replaces CC |
|
|
What percentage of all lipomas do ACC lipomas constitute? |
30-50% - may have associated calcification |
|
|
Where are ACC lipomas found? |
The interhemispheric fissure |
|
|
What are dandy walker malformation? |
Abnormal neural tube closures, with 4th ventricle malformation |
|
|
What percent of DW patients also have ACC or other anomalies? |
70% |
|
|
What percent of DW patients also have a chromosomal anomaly? |
20-50% are also trisomy 13, 18, 21 |
|
|
What do the ventricles look like in Dandy Walker? |
- Dilated 4th ventricle that communicates with the cisterna magna (cystic post. fossa) [cause: atresia of the foramina of M & L] - Cyst compresses aqueduct, causing hydro: above and below 4th ventricle (or may develop later in 80% of cases) |
|
|
How might we treat hydro in the ventricles for DW? |
Shunts may need to be placed separately (in lateral ventriclesand cyst) to ensure effective drainage |
|
|
What will the parenchyma of a DW patient look like? |
• hypoplastic cerebellar hemispheres, displaced laterally • absent vermis (normal vermis seen @ 17-18 wks) • elevated tentorium (straight and trans sinuses elevated) |
|
|
What are the differentials for DW? |
- Large (mega) cisterna magna - Arachnoid cyst (but cysts are usually symmetrical) |
|
|
What is Dandy Walker Variant? |

• cerebellum “normal” • cisterna magna communicates w/ 4th Vent • mildly hypoplastic vermis; not hydrocephalic (3v, 4Vaqueduct big) This is more difficult to diagnose sonographically but occurs 2x more often. 30% of cases are associated with CNS or extra-CNS anomalies. |
|
|
Name the 6 diagnostic findings of Dandy Walker Malformation? |
(1) Enlarged 4th ventricle connecting to the cisterna magna (2) Large Posterior Fossa (3) Hypoplastic Vermis (4) Hypoplastic cerebellar lobes displaced laterally (5) Hydro (80%) above and below the 4th ventricle (6) Absent Corpus Callosum (70%) |
|
|
What 2 disorders are associated with Dandy Walker? |
(1) Joubert's Syndrome: absent vermis, like ACC of the cerebellum, white matter is unable to migrate rt to lt. (2) Meckel-like syndrome: DW, polycystic kidneys, hepatic fibrosis, hand, and genital anomalies. |
|
|
Which is the most severe form of holoprosencephaly? |
Alobar |
|
|
What is the best imaging examination for holoprosencephaly? |
MRI |
|
|
Explain the ventricles appearance for all types of holoprosencephaly? |
• Alobar - single ventricle • Semi-lobar - single ventricle, but occipital horns • Lobar-near normal occ & temp horns, 3rd Ventricle, fused anterior horns with no septi pellucidi |
|
|
Explain the parenchymal appearance for all types of holoprosencephaly? |
• Alobar - minimal brain tissue • Semi-lobar-more occipital tissue w/falx & longitudinal fissure, single thalamus, part ACC • Lobar-quite normal!! Shallow anterior falx/fissure, abssepti pellucidi, fused frontal lobes (and horns), partialACC (genu and rostrum only) |
|
|
What type of holoprosencephaly does septo-optic dysplasia face resemble? |
Looks like lobar |
|
|
What is septo-optic dysplasia? |

Optic nerve is dysplastic = limited vision, may be associated with holoprosencephaly, ACC, or Chiari I. There is an absent septum pellucidum |
|
|
What is the mildest form of holoprosencephaly? |
Septo-optic dysplasia - absent CSP, optic tract hypoplasia (MRI to confirm since not seen on US). |
|
|
Explain semilobar holoprosencephaly. |
Semi-lobar specimen with occipital lobes, fused thalamus and choroids (U-shaped). There is a partial corpus callosum, a partially separated thalamus with mid-facial anomalies such as hypotelorism or cleft lip. |
|
|
Explain alobar holoprosencephaly. |
Single midline crescent shaped ventricle with a thin layer of cerebral cortex. No interhemispheric fissure, no falx, no corpus callosum. Fused thalami, choroid plexus, and basal ganglia. No 3rd ventricle and a large dorsal cyst. |
|
|
What is schizencephaly? |
A destructive process, in utero, clefts, ventricle to lateral fissure, lined with dysplastic grey matter, unlike porencephaly. Can be uni or bi lateral and is associated with an absent CSP and/or optic-nerve hypoplasia. |
|
|
When will schizencephaly happen? |
pre-migration - in the second trimester |
|
|
What is Lissencephaly? |
Smooth brain, without sulci (may be caused by infection in utero - 3-4 months along). There is also absent opercularization in the lateral fissures. |
|
|
What is hydranencephaly? |
Complete destruction of normal brain tissue. |
|
|
What is the cause of hydranencephaly? |
Occlusion of the ICA after 14 weeks gestation |
|
|
What structures of the brain are not affected by hydranencephaly? |
The posterior cerebral artery suppliesthalamus, choroids, brain stem &cerebellum – these structures are OK! |
|
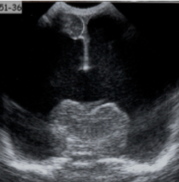
What pathology is this? |
Hydranencephaly, it is not holoprosencephaly because the falx and the thalamus are present |
|
|
What is porencephaly? |
Destruction of normal brain parenchyma - the cysts always connects with the ventricles but not to cortex. |
|
|
What causes porencephaly? |
hemorrhage, infection (TORCH), or trauma |
|
|
What type of tissue is the healed brain tissue from porencephaly? |
Gliotic White Matter |
|
|
What is cystic encephalomalacia? |
Focal brain damage (softening) - glial tissue may form septa, and neurons are destroyed. |
|
|
What is the difference between cystic encephalomalacia and porencephaly? |
with cystic encephalomalacia the cysts are not connected to the ventricles |
|
|
What are the causes of cystic encephalomalacia? |
• LARGE cysts - from diffuse causes - infection, birth asphyxia • focal cystic areas - secondary to thrombus |
|
|
What can an increased intracranial pressure cause? |
It can obstruct blood flow, destroy brain cells, and cause herniation. |
|
|
What is acquired hydrocephaly secondary to? |
hemorrhage, infection, etc. |
|
|
What is the incidence of hydrocephaly congenitally? |
5-25% per 10,000 births |
|
|
What are the contents of the cranial cavity and what are their relative amounts? |
Blood (10%), Tissue (80%), and CSF (10%) |
|
|
Where is the majority of intracranial blood? |
Venous Circulation |
|
|
Where can CSF flow to compensate for increased ICP? |
To the lumbar cistern |
|
|
What are the 3 main causes for a CSF increase? |
(1) Obstruction (2) Decreased absorption (3) Over production |
|
|
What can treat increased ICP? |
A shunt can decrease the risk of infection and hemorrhage and also decrease the need for endoscopic surgery. |
|
|
What are the clinical signs and symptoms of hydrocephalus? |
Increased head circumference and bulging fontanelles. |
|
|
What can be done to measure the pressure of the CSF? |
A lumbar puncture (manometer) - can also drain CSF |
|
|
What are the potential clinical outcomes of hydrocephaly? |
• Developmental delay – Edema may cause delayed myelination – Ischemia: compression of vessels • Rapid Increases in ICP can compress brain stem, vital functions– may cause herniation of brain (through the foramen of munroe) ... death |
|
|
What is the risk of shunt placement? |
Infection, hemorrhage, or rapid decompression (leads to slit like ventricles) |
|
|
What is thirdventriculostomy? Choroid Plexus cauterization? |
ETV - hole put into the third ventricle to drain into the subarachnoid space (when cerebral aqueduct is obstructed) CPC = done when the choroid is overproducing CSF |
|
|
What are the sonographic findings of hydrocephalus? |
- Dilated 3rd ventricle or open wide 4th ventricle - Rounded frontal horns - lateral ventricles that rise above the corpus callosum - dilated temporal horns and 4th ventricle |
|
|
What are the possible etiologies of hydrocephaly? |
- Intraventricular Obstruction (non-communicating) - Extraventricular Obstruction (communicating) - subarachnoid space or cisterns - Choroid plexus Papiloma - Venous obstruction - Vascular malformation (AVM) - Non-obstructive, as a result of brain atrophy |
|
|
What causes ventriculomegaly? |
Brain atrophy |
|
|
What can cause intraventricular obstructive hydro? |
Infection, hemorrhage, or congenital abnormalities such as aqueductal stenosis, DW, fibrosis of the foramen of monro, tumour, cyst, AVM, or Chiari II. |
|
|
What can cause extraventricular obstructive hydro? |
Hemorrhage, infection, fibrosis of cisterns/arachnoid villi. |
|
|
How do you determine the level of obstruction? |
Look at what parts of the system are dilated |
|
|
What is colpocephaly? |
A term used to describedispropor=onate prominenceof the occipital horns of thelateral ventricles (eg. ACC) |
|
|
What causes ventriculomegaly/brain atrophy? |
• Hypoxic-ischemic injuries – Severe cases result in brain atrophy – 2-4 weeks arer global ischemia – Passive expansion, not due to pressure • “Glutaric aciduria type 1”- unusual cause – Macrocephaly at birth – atrophy later - Bilateral widening of the Sylvian fissures |
|
|
Who is at risk for a hypoxic ischemic event in premature infants? |
Infants of moms with: - Chronic cardiac or lung diseases - Cardio-respiratory arrest during delivery - Placental insufficiency - Shock - Placental Abruption (assoc. with cocaine and alcohol abuse) Also, infants who are on mechanical ventilation or suction (causing venous obstruction), tension pneunothorax, exchange transfusions, immature hypothalamus that distorts BP. |
|
|
What are special issues of premature infants? |
(1) Hypothalamus: will not function until term (2) Germinal Matrix: risk of hemorrhage (3) Arterial Watersheds: deep white matter (lacks proper perfusion) |
|
|
Where might we find the germinal matrix? |
The dense layer below the ependyma of the lateral ventricle, whose job it is to create brain tissue. |
|
|
Why is there such a high risk of hemorrhage to the germinal matrix? |
There is no autoregulation and it is very fragile. |
|
|
What does hypertension lead to? |
Focal hemorrhage in the germinal matrix |
|
|
What does hypotension lead to? |
Focal or diffuse infarct to the watershed areas. |
|
|
What is a cast? |
A portion of the ventricular system that is filled with clot |
|
|
Where is the watershed? |
The age of the patient determines where the watershed area is: Premature Infants > Periventricular/subcortical regions (white matter) Term Infants > Para sagittal cortical/subcortical regions (grey/white border) |
|
|
Other than watershed areas, what other factors affect HIE? |
- Metabolically Active areas are more susceptible to HIEs like white matter tracks, oligodendrocytes, or babies in the 2nd trimester - Length of time: focal infarct=partial obstruction with short time, and global/profound infarct (lengthly hypoxic event) |
|
|
What might the brain look like with a global infarct? |
Edema of the cerebrum and development of cystic structures. |
|
|
What is damaged in various aged infants when there is an infarct? |
In premature infants – born at 24 to 30 weeks: • GMH - germinal matrix hemorrhage, also called subependymal hemorrhage – SEH • PVL - periventricular leukomalacia (infarc&on and necrosis of the periventricular white matter) In term infants: • Parasagittal infarction, edema • Thalamus, basal ganglia (rare) At 3 months: • Thalamus, basal ganglia, & cortex At 1 yr: • just like adults - cortex |
|
|
Will subependymal hemorrhages resolve? |
Most will with no complications, but the most common complication will be subependymal cysts |
|
|
How long will it take following a bleed for porencephalic cysts to develop? |
About 7 days |
|
|
What fraction of GMHs occur in the first 24 hours? By day 7? |
Only 1/3 of GMHs occur in the first 24 hours and 90% occur by day 7 |
|
|
When is the best time then to screen for GMH? |
Between day 10-14 with follow-up at 1 month for all babies less than 32 weeks, and 1500 grams. |
|
|
How common did GMH used to be? Why are they not as common now? |
They were once as common as 55%, but this has decreased because of prenatal steroids and respiratory therapies like surfactant being used. |
|
|
What are we looking for in the 10-14 day scan versus the 1 month scan? |
10-14 day: GMH or Post-hemorrhagic hydro 1 month: PVL or ventricular enlargement |
|
|
What are the grades of bleeds? |
I - GMH, small hemorrhage at caudate area II - Intraventricular, hemorrhage spills into ventricles, but they are not dilated III - Larger hemorrhage with dilated ventricles (hydro) IV - Intraparenchymal hemorrhage due to hemorrhage or infarct |
|
|
Other than grading how else may we describe a bleed? |
Where is it? subependymal, intraventricular, intraparenchymal, sub-arachnoid, intracisternal, etc. |
|
|
What will a subependymal hemorrhage look like? |
Homogenous, echogenic, seen at caudothalamic groove under the ependyma, swelling at the head of the caudate, and possible involvement of the ventricles - grade II (inflammed ventricle walls). |
|
|
What will intraventricular hemorrhage look like? |
Echogenic, especially in the dependent lateral horns, possibly a ventricular cast or bulky choroids, or CSF with echoes, or a change in the CSF-blood fluid levels. |
|
|
What can blood do to the ventricles? |
Blood is an irritant and can cause chemical ventriculitis - thick, echogenic ventricular walls. |
|
|
What is the same as intraparenchymal hemorrhage? |
Hemorrhagic venous infarction - when there is a germinal matrix bleed there can be obstruction of the terminal veins causing congestion in the tissue and this leads to infarction. |
|
|
What are the sonographic features of intraparenchymal hemorrhage? |
Usually unilateral and echogenic in the frontal, parietal, and/or occipital lobes. Causes a mass effect. 1-7 days: echogenic 2-5 weeks: echogenic rind, liquefy, retraction (porencephalic cysts created) >4 weeks: porencephaly with ventriculomegally and atrophy with widened sulci. |
|
|
What happens when the clot resolves? |
It will leave porencephaly |
|
|
What is the outcome of intraparenchymal hemorrhage? |
80-100% of children will have motor defects - permanent spastic hemiparesis on the contralateral side. |
|
|
How will the appearance of an intraventricular clot evolve?
|
From echogenic, to centrally echolucent, to shrinking and dissolving over several weeks. |
|
|
Where will intraparenchymal hemorrhage happen in term infants? |
The posterior fossa and the subarachnoid/dural space. |
|
|
Where will we be looking for infarction and cerebral edema in term infants? |
- Diffuse Cerebral edema (profound infarct) - Focal infarction (watershed regions - partial infarct) - Cerebellar infarction - Basal ganglia vasculopathy |
|
|
Is cerebral edema and infarction common in premature infants? |
No, it is rare except for PVL |
|
|
Who is at risk for hypoxic ischemic events in term infants? |
Infants of the MOMS with: – chronic cardiac or lung diseases – cardio-respiratory arrest – placental insufficiency – shock – abruption – rare assoc w. cocaine, alcohol abuse • Babies with meconium aspiration, birth asphyxia– Affects their ability to auto-regulate blood pressure |
|
|
What is vasogenic edema? |
The integrity of the blood brain barrier is disrupted allowing fluid to escape into the extra-cellular fluid surrounding the brain cells. This is due to prolonged ischemia, hemorrhage and infection. AFFECTS THE WHITE MATTER |
|
|
What is cytotoxic edema? |
Swelling of the cells due to hypernatremia caused by severe ischemia. If severe this can lead to infarction and necrosis. GREY MATTER AFFECTED. |
|
|
What type of edema does arterial occlusion lead to? |
Both Vasogenic and cytotoxic (grey and white matter affected) |
|
|
What will diffuse edema look like sonographically? |
Slit-like ventricles from compression of edema, echogenic parenchyma abscures landmarks such as the sulci (silhouetting). |
|
|
Within 2 weeks of a child acquiring diffuse edema, what may happen? |
Atrophy of the brain tissue and ventriculomegaly. The head circumference will be normal and progressively get smaller. |
|
|
Where is the most common location for a focal infarction? |
The MCA circulation (often a single area impacted) so structures supplied by the MCA are affected. |
|
|
What are the sonographic appearances of a focal infarct? |
Echogenic parenchyma with sharp borders |
|
|
2 Weeks following a term-infant's focal infarction what may happen? |
Focal cystic encephalomalacia (softened brain tissue) and later atrophy and ventriculomegaly. |
|
|
What are the risk factors for focal infarcts? |
– severe birth asphyxia – prematurity – congenital heart (irregular beats cause clots) – meningitis – emboli – polycythemia – trauma |
|
|
What are the signs and symptoms of focal infarcts? |
Asymmptomatic, seizures, lethargy, or coma |
|
|
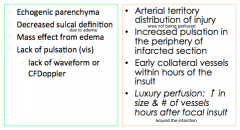
What are the sonographic signs of cerebral infarction? |
|
|
|
What is luxury perfusion? |
An increase in the number of vessels and the size of existing vessels in response to a focal infarct often occurring hours after the insult. |
|
|
Why is it difficult/uncommon to diagnose cerebellar infarction? |
This is a very uncommon pathology, and also the vermis is very echogenic so it is hard to pick up a small infarct or hemorrhage here. |
|
|
What is lenticulostriate vessels? |
A basal ganglia vasculopathy characterized by echogenic linear echoes around the vessels of the thalamus and basal ganglia - can sometimes be demonstrated under colour Doppler |
|
|
What pathologic conditions are lenticulostriate vessels associated with? |
Viral infections, trisomy 13/21, and twin-twin transfusions |
|
|
What is a non-hemorrhagic focal infarct? |
A stoke caused by the vessels being walled of in some way. 90% of children become handicapped from this. |
|
|
What children are at risk for having a non-hemorrhagic stroke? |
Those with sickle cell anemia. |
|
|
What are the risk factors for cerebellar hemorrhage? |
- Traumatic Birth - ECMO - Coagulopathy - Germinal matrix within the 4th ventricle (premies) |
|
|
What will a cerebellar hemorrhage look like sonographically? |
Echogenic when it is acute, and as it becomes chronic, cysts will form. |
|
|
What may be the only type of hemorrhage in full term infants? |
subarachnoid hemorrhage |
|
|
What children are at risk for developing a subarachnoid hemorrhage? |
Birth asphyxia, trauma, DIC, or premies with intraventricular hemorrhage. |
|
|
What are the sonographic appearances of a subarachnoid hemorrhage? |
Enlarged sylvian and IH fissure with thickened and echogenic sulci. You can see the cisterns in the posterior fossa view. |
|
|
With colour Doppler what will the subarachnoid hemorrhage look like? |
Vessels will be seen crossing into the subarachnoid space. |
|
|
What children are at risk of developing a subdural hemorrhage? |
Term infants with birth trauma like SBS (massive in children with bleeding disorders) |
|
|
With colour Doppler what will the subdural hemorrhage look like? |
We will see the vessels compressed into the brain surface |
|
|
Subdural hemorrhage is the most common cause of what clinical finding? |
increased head circumference after 2 weeks of age (since it is so superficial) |
|
|
What are the differential diagnoses for subdural hematoma? |
Meningitis (check S&S) or non-accidental trauma (SBS - if subdural fluid is seen after neonatal period) |
|
|
What is periventricular leukomalacia? |
The infarction and necrosis of the perventricular white matter (including the corpus callosum) |
|
|
What type of history will a PVL patient have? |
Hx of cardio-respiratory compromise>hypotension>ischemia |
|
|
What is an associated finding of PVL? |
GM hemorrhage and 80% are associated with IVH. Chorioamnionitis is also associated. |
|
|
What treatment has decreased the incidence of PVL? |
Antenatal steroids |
|
|
What are the sonographic appearances of PVL? |
Often bilateral, supero-lateral to the trigones, edema and hemorrhage causes increased echogenicity of the white matter tracts that appears patchy and brighter than the choroid. Infarct leads to coagulation necrosis (cysts). |
|
|
What are the 3 special issues regarding the pathogenesis of PVL? |
Deep white matter is a watershed zone (1) hypothalamus-will not function till term (2) Immature vasculature (watershed) (3) Immature oligodendroglial cells (vulnerable to hypoxic episodes) |
|
|
What does the appearance of acute PVL mimic? |
Normal periventricular blush so it is important to screen for PVL (cystic stage is obvious after 2-3 weeks) |
|
|
What can PVL eventually lead to? |
Subtle atrophy and ventriculomegaly - gliosis eventually fills the cysts and sonographically appears normal |
|
|
What is the sonographic progression of PVL? |
Day 1-3: patchy echogenicity Week 1-2: Decreasing echoes Week 2-3: Cystic (bilateral and symmetric) Month 1-3: Return to "normal" but with atrophy and ventriculomegaly |
|
|
Are PVL cysts connected to the ventricles? |
No - unlike porencephalic cysts caused by IPH |
|
|
What percentage of cerebral palsy patients had PVL? what did this cause? |
84% which caused absent and delayed myelination. |
|
|
What modality is best for PVL follow-up? |
MRI is better than CT to diagnose glial scarring. |
|
|
What are the late complications of PVL? |
Decreased myelination causing spastic diplegia of the legs or quadriplegia if severe. This is a feature of cerebral palsy |
|
|
What is ventriculitis? |
Large ventricles with echogenic debris, developed in patients with meningitis (60-95%) - shaggy bright ependyma with fibrous septations. Abscess is rarely seen, but if it is present it will have a mass effect, echogenic walls, with an anechoic cavity. |