Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
177 Cards in this Set
- Front
- Back
|
Where is glucagon secreted?
|
From the alpha cells of the pancreas
|
|
|
What is the function of glucagon?
|
Increases hepatic glucose output -->increases blood glucose concentration
|
|
|
What triggers glucagon release?
|
Released in direct response to low blood glucose levels
|
|
|
What mechanism does glucagon use to increase blood glucose concentration?
|
Breaks down glycogen
|
|
|
What is the name of the area where alpha and beta cells occur in the pancreas?
|
Islets of Langerhans
|
|
|
What cells secrete insulin?
|
Pancreatic Beta Cells
|
|
|
What two circumstances is insulin secreted?
|
-Basally in small amounts between meals and overnight
-Boluses in response to food |
|
|
What is the function of insulin?
|
Promotes the uptake, utilization, and storage of glucose --> lowers plasma glucose concentration
|
|
|
What percentage of insulin is released from the pancreas as Basal?
As bolus? |
50% Basal
50% Bolus |
|
|
During fasting, is the insulin level in the body zero?
|
No, at no time is the insulin level at zero in the body
|
|
|
What is Basal Insulin?
|
Small amounts of the insulin are released by the body every 24 hours
|
|
|
How much insulin in released in adults every hour?
|
About 1 unit
-Basal Insulin |
|
|
What is Bolus Insulin?
|
-Used to limit postprandial hyperglycemia by stimulating glucose uptake by peripheral tissue
-In response to food. |
|
|
List the other names for Bolus Insulin.
|
-premeal
-mealtime -prandial -nutritional insulin |
|
|
What determines the resting membrane potential in pancreatic B-cells?
|
the ATP-sensitive K channels
|
|
|
What is the mechanism for insulin release?
|
-Glucose enter B cells Via GLUT-2
-K(atp) is blocked causing depolarization and Ca++ to rush in. -Ca++ signal induces insulin secretion. |
|
|
What is Type I DM?
|
Immune response or viral attack on Beta cells. Body does not produce insulin
-These pts will always require insulin injections |
|
|
Describe Type II DM?
|
-Pts produce insulin, but it is usually not enough
-Pts on oral anitbiotics and encouraged to diet and exercise |
|
|
Define hypoglycemia.
|
A pathologic state produced by a lower than normal amount of sugar (glucose) in the blood
|
|
|
What is the clinical term for a condition in which an excessive amount of glucose is in the blood?
|
Hyperglycemia
|
|
|
What two sources were used to create animal insulin?
|
beef or pork
|
|
|
Which technique is utilized in the production of human insulin?
|
recombinant DNA using E. coli or yeast
|
|
|
Why is human insulin preferred over animal insulin?
|
Human insulin is less likely to have antibodies, reaction or allergy
|
|
|
Can insulin be administered orally?
|
No`
|
|
|
How long is the half-life of insulin?
|
Only a few minutes due to rapid removal by the liver and kidneys
|
|
|
What is the administration route for all insulin medications?
|
Sub-Q
-Short acting can be given IV as well |
|
|
What location offers the most rapid absorption for insulin?
|
the abdomen
|
|
|
What is lipodystrophy?
|
Hardening of the injection site when a pt does not rotate sides between injections
|
|
|
If a pt is on insulin, but is still hyperglycemic, what is a possible reason?
|
Pt not rotating injection sites
|
|
|
List the 3 rapid acting insulin drugs.
|
-insulin aspart (Novolog)
-insulin lispro (Humalog) -Insulin glulisine (Aprida) |
|
|
What is the onset of action for rapid acting insulin?
|
2-15 mins
-very fast |
|
|
What is the duration of Rapid Acting Insulins?
|
1-5 hours
|
|
|
What is the peak for Rapid Acting insulin?
|
30 mins to 3 hours
|
|
|
When do you administer rapid acting insulin?
|
Immediately before meals
|
|
|
Give an example of a short acting insulin
|
Insulin Regular (Humulin R)
|
|
|
Which form of insulin can be administered via IV?
|
Short acting insulin
|
|
|
What is the onset and peak for short acting insulin?
|
onset: 1-2 hours
peak: 2-4 hours |
|
|
When should short acting insulins be administered and what are their duration of action?
|
-30 to 45 minutes before meals
-DOA: 8-12 hours |
|
|
What is an example of intermediate acting insulin?
|
NPH (Humulin N)
|
|
|
What is the onset of action and Duration for NPH?
|
Onset: 1-1.5 hours
DOA: 12 to 16 hours |
|
|
Which insulin appears cloudy?
|
NPH (Humunlin N)
Intermediate acting Insulin |
|
|
Can you use NPH for emergency IV use?
|
NO, only Humulin R
|
|
|
How would you mix Humulin N and Humulin R in one syringe?
|
Add R first and then N
|
|
|
What are the long acting insulin drugs?
|
-Glargine (Lantus)
-Detemir (Levenir) |
|
|
What is the onset of action and duration of Long acting Insulin?
|
Onset: 1-2 hours
Duration: 24 hours |
|
|
Which insulin does not have a peak
|
Glargine
-It never gets to hypoglycemic point |
|
|
What is the peak time for detemir?
|
6-8 hours
|
|
|
How often are long acting insulins administered?
|
only Once daily
|
|
|
In general, what are rapid/short acting insulins used for?
|
-Used for mealtime coverage
-Bolus dose |
|
|
What determines the onset, peak and duration of each insulin drug?
|
The form of insulin administered
|
|
|
In general, when do we use intermediate and long acting insulins?
|
-Used to treat basal needs
-Not intended for mealtime use |
|
|
What insulin drug is considered a combination product?
|
-Novolin or Humulin 70/30
|
|
|
How would you describe the dosing for insulin?
|
It is really trial and error based on
-total body weight -Dosed in units |
|
|
What should you instruct your pt to avoid when administering insulin?
|
Avoid exercise close to administration period
-Do not rub injection site -heat accelerates absorption |
|
|
List the administration sites from best to worst
|
abdomen>buttocks>arm/leg
|
|
|
Which tool allows for more accurate and faster and easier dosing of insulin?
|
Portable pen injectors
|
|
|
Why is the insulin infusion pump considered invasive?
|
Because a needle is implanted in the skin for long periods of time
|
|
|
Which type of DM is most likely to use an Infusion pump?
|
Type I
|
|
|
What type of insulin is delivered with using the infusion pump?
|
short acting insulin
|
|
|
How should insulin not being used be stored?
|
in the refrigerator
|
|
|
How long can you use insulin at room temperature that has been opened?
|
28 days
|
|
|
What are the adverse effects of insulin?
|
*hypoglycemia*
-insulin allergy: rare -Lipohypertrophy |
|
|
What are the signs and symptoms of hypoglycemia?
|
-Tachycardia
-confusion -vertigo -diaphoresis |
|
|
What should you do for a conscious patient who is suffering from hypoglycemia?
|
you can give them juice or a chocolate bar.
|
|
|
If your patient is so hypoglycemic that they are unconscious, what should you do?
|
Treat them with 20-50mL of 50% dextrose by IV
-or 1mg glucagon either Sub Q or IM |
|
|
Should a nurse shake the vial before administering it?
|
No, never! They should roll it.
|
|
|
List the First generation of Sulfonylureases?
|
-Chlorpropramide (Diabinese)
-Tolbutamide (Orinase) -Tolazamide (Tolinase) |
|
|
List the Second Generation of Sulfonylureases?
|
-Glyburide (DIaBeta, MIcronase, Glynase Pres Tab)
-Glipizide (Glucotrol, Glucotrol XL) -Glimepiride (Amaryl) |
|
|
What types of patients can be perscribed sulfonylureases?
|
Only Type II.
-effective only in pts with functioning B cells. |
|
|
What is the primary effect of sulfonylureas?
|
Increases secretion of insulin from B-cells of the pancreas
|
|
|
What are two secondary effects of sulfonylureas?
|
1. Increases insulin receptor sensitivity
2. Decreases hepatic glucose output |
|
|
Where are sulfonylurea absorbed?
|
In the GI
|
|
|
How are sulfonylurea metabolized?
|
90-100% hepatic metabolism
|
|
|
What is unique about glyburide?
|
Unlike other sulfonylurea that have nearly 100% hepatic metabolism, glyburide is metabolised 50% by liver and excreted 50% by the kidneys
|
|
|
Which sulfa pts must you be cautious with?
|
-Hepatic or renal disease
-Elderly (kidney funciton is not as good) -Pts with a "sulfa" allergy. |
|
|
What should you educate your pt on sulfonlyureas to do?
|
Where SPF because sulfas cause sun sensitivity
|
|
|
What are the adverse effects of sulfonylureas?
|
*Hypoglycemia*
-dermatologic reaction: rash, photosensitivity, hypersensitivity -GI disturbances: NV, abnormal liver function -weight gain (not ideal, want pt to lose weight) |
|
|
Which drug option is ideal for pts with sulfa allergies?
|
Meglitinides
|
|
|
What are the 2 drugs under the category of meglitinides?
|
-Repaglininde (Prandin)
-Nateglinide (Starlix) |
|
|
What is the MOA of meglitinides?
|
Increase secretion of insulin from B-cells
|
|
|
How are meglitinides like sulfas?
|
They are structurally related to sulfas but have no sulfa moiety
|
|
|
What is the onset of action and duration for repaglinide and nateglinide?
|
OOA: 15-30 mins
DOA: <4 hours |
|
|
Where are meglitinides metabolized?
|
CYP 3A4 and CYP 2C9
|
|
|
What are 3 potential advantages for meglitinides?
|
1. Rapid onset oand short duration of action
2. May be used in the elderly 3. May be useful to patients who skip meals |
|
|
What are the adverse effects of meglitinides?
|
-hypoglycemia
-weight gain |
|
|
Give an example of a Biguanide
|
metformin (glucophage)
|
|
|
What is the MOA of metformin
|
-Decrease hepatic glucose output
-increase peripheral glucose uptake and untilization |
|
|
What are the advantages of metformin (glucophage)?
|
-Does not cause hypoglycemia (doesn't effect insulin release)
-Weight loss |
|
|
How are biguanides excreted? Where are they metabolized?
|
100% through kidneys
-Not metabolized through the liver? |
|
|
What are the adverse effects of biguanides?
|
-Diarrhea
-lactic acidosis -increase lactate in the body |
|
|
What are the contraindications for metformin?
|
-Renal impairment
-men creatinine ≥1.5 -women creatinine ≥ 1.4 -Hepatic impairment |
|
|
What must you do if you must administer a biguanide with an iodinated contrast material?
|
-You must have pt stop the biguanide for 24 hours prior to ICM and stay off of meds 4 hours after
|
|
|
What drugs are known as α- Glucosidase inhibitors?
|
-Acarbose (Precose)
-Miglitol (Glyset) |
|
|
Which drugs are potent competitive inhibitors of the brush border cells?
|
α- Glucosidase inhibitors
-They stop the breakdown of carbohydrates |
|
|
Are α- Glucosidase inhibitors absorbed well in the body?
|
No
|
|
|
What is the onset of action for α- Glucosidase inhibitors and how are they metabolized?
|
-6 hours
-metabolized by intestinal bacteria |
|
|
What are the adverse effects of α- Glucosidase inhibitors?
|
-Abdonminal pain, flatulence, diarrhea
|
|
|
What can occur at high doses of Acarbose?
|
Hepatotoxicity
|
|
|
Patients suffering significant GI disorders are contraindicated from which drug class>?
|
α- Glucosidase inhibitors
|
|
|
Name 2 examples of Thiazolidinediones
|
-Rosiglitazone (Avandia)
-Pioglitazone (Actos) |
|
|
What the the MOA of Thiazolidinediones?
|
Binds to the NUCLEAR STEROID HORMONE RECEPTOR and promotes glucose uptake into skeletal and muscle/adipose tissue
|
|
|
What is the primary advantage of using drugs such as rosiglitazone?
|
There is no hypoglycemia!~
|
|
|
What are the adverse effects of Pioglitazone and Rosiglitazone?
|
--Thiazolidinediones
-Hepatotoxicity -Edema (which can worsen if combined with insulin) |
|
|
Which pts must you take caution with when administering Thiazolidinediones>
|
-Pts with hepatic disease or failure
-CHF because edema can worsen if combined with insulin!! |
|
|
What are incretins?
|
Intestinal hormones released in response to glucose
|
|
|
What is GLP-1 and when is it released?
|
-Glucagon-like peptide-1
-rapidly rises within minutes of food ingestion |
|
|
What is DDP-4 and what is its natural purpose in the body?
|
-dipeptidyl peptidase-4
-rapidly degrades GLP-1 in the body |
|
|
What actions do GLP-1s have in the body naturally?
|
-Enhance glucose-dependent insulin secretion (β)
-Suppress glucagon secretion (α) -Slow the rate of gastric emptying -Reduces appetite |
|
|
What class does Exenatide (Byetta) fall under?
What is its function? |
Incretin Mimetics
-GLP-1 AGONIST! |
|
|
How is exenatide administered?
|
Pre-filled pens for Sub-Q injeciton
|
|
|
List some adverse effects of INCRETIN MIMETICS
|
-Hypoglycemia (esp is combined with sulfa)
-Nausea and diarrhea -headache -Pancreatitis |
|
|
List the DPP4-Inhibitors
|
--Sitagliptin (Januvia)
-Saxagliptin (Onglyza) |
|
|
MOA of DPP4 INHIBITORS?
|
Stops the breakdown of GLP-1 by inhibiting DPP4
|
|
|
What adverse effects are associated with DPP4 inhibitors?
|
-GI effects
-NO evidence of HYPOGLYCEMIA -(This medicine is new) |
|
|
What drug falls under Amylin Analogue?
|
Pramlintide (Symlin)
|
|
|
What is the MOA for Amylin Analogues?
|
-Slows gastric emptying
-Suppresses glucagon secretion -Decreases glucose output by the liver |
|
|
Which patients can be give Pramlintide?
|
Both Type I and II
-Those that have failed other types of meds |
|
|
What are the adverse effects of Pramlintide and why are they odd?
|
-Severe hypoglycemia
*this is odd because the drug doesn't actually alter the insulin concentration, but drops the blood sugar* -GI disturbances |
|
|
List all the classes of meds that cause hypoglycemia!!
|
-Amylin Analogues
-Incretin Mimetics -Meglitinides -Sulfonlyurea -Insulin |
|
|
Which DM drugs do not cause Hypoglycemia?
|
-Biguanides
-Thiazolidinediones -DPP4-inhibitors |
|
|
What hormones are released by the Thyroid Gland?
|
T3-active form
T4 (thyroxine)-inactive form |
|
|
What element is essential in Thyroid Hormone production?
|
Iodine
|
|
|
How often is T3 and T4 created and stored?
How often are they released? |
T3 and T4 are constantly formed and stored.
Not a constant release |
|
|
What % of T4 and T3 is secreted from the Thyroid gland?
|
T4= 100%
T3= <20% is secreted from Thyroid Gland |
|
|
Where can we find Thyroid Hormone regulation?
|
Hypothalamus: neg feedback on TRH
-Anterior pituitary: neg feedback on TSH |
|
|
What is Thyrotoxicosis?
|
Hyperthyroidism
-excessive amount of thyroid hormone |
|
|
What general class of drugs are used to treat Hyperthyroidism?
|
Anthithyroid medications
|
|
|
What drugs fall under Thioamides?
|
-Antithyroid Meds
-Propylthiouracil (PTU) -Methimazole (Tapazole) aka MMI |
|
|
What is the MOA of Thioamides?
|
Inhibits the iodination of tyrosine and the coupling of iodotyrosines
|
|
|
What additional mechanism does PTU have on T4 and T3?
|
it inhibits the peripheral conversion of T4 to T3
|
|
|
Thioamides do NOT?
|
effect the release of performed T4 and T3
|
|
|
What are the adverse effects of Thioamides?
|
-Rash
-Edema -Decreased WBC count; reverses on discontinuation if caught early |
|
|
What must you do as a nurse if your pt on thioamides has a drop in WBC?
|
conduct a CBC on the pt every 6 months
|
|
|
How long does thioamides require for a pt to become euthyroid?
|
1-2 months
|
|
|
What is the duration for Thioamides?
|
They have a short half life but accumulate in the thyroid gland to exert longer effects
|
|
|
What is hypothyroidism?
|
Under active thyroid: does not produce enough TH
|
|
|
List the Natural Thyroid Hormones.
|
-Thyroid (Armour Thyroid)
-Thyroglobulin |
|
|
Why is Armour Thyroid not used as much?
|
Because it is derived from desiccated hog, beef or sheep thyroid it can cause a lot of ALlERGIES!
|
|
|
Where does thyroglobulin come from?
|
Purified hog gland extract that contains a standard amount of T4 and T3 in ration of 25:1
|
|
|
In general, why are Natural Thyroid hormones not readily used?
|
-Bioavailability is unpredictable
-Allergies |
|
|
List the Synthetic Thyroid Hormones
|
-Levothyroxine (T4)
-Liothyronine (T3) -Liotrix (T4 and T3 ratio of 4:1) |
|
|
Which of the synthetic TH is used most often?
|
Levothryoxine
|
|
|
Which Synthetic TH is considered a prodrug?
|
Levothyroxine
|
|
|
What is the onset for Levothyroxine and how does it benefit the pt?
|
2-3 week onset
-gives the body time to adjust |
|
|
What are the adverse effects of LEVOTHYROXINE?
|
-Heart Failure
-Angina -MI -Hyperthyroidism |
|
|
How should the nurse administer Levothyroxine?
|
-Consistently every morning before meals
-With a large glass of water |
|
|
What is the function of osteoblasts?
|
To encourage bone deposit
-To build bone |
|
|
Which cells are responsible for breaking down bone?
|
Osteoclasts
|
|
|
Which hormones are involved in the control of calcium?
|
-Vitamin D
-Parathyroid Hormone PTH -Calcitonin |
|
|
Vitamin D has what effect on the body?
|
It stimulates Ca absorption from the GI tract
|
|
|
What is the positive method that PTH uses to increase Ca?
|
-Decreases Ca excretion by the kidneys
|
|
|
Which method used by PTH to increase Ca is not favorable?
|
-Increasing bone resorption by stimulating osteoclast activity
|
|
|
Calcitonin has what effect on Ca levels?
|
Released in response to increased plasma calcium levels and it acts to inhibit bone resorption
|
|
|
In general, what medications are used to treat Bone Disorders?
|
-Ca and Vit D suppliments
-Bisphosphonates -Calcitonin |
|
|
How is Ca absorbed?
|
Absorption from the gut is incomplete even in the presence of Vit D
|
|
|
Which for of Calcium supp requires stomach acid?
|
Calcium carbonate
|
|
|
What is unique about Calcium citrate?
|
It does NOT require stomach acid for absorption
|
|
|
If a pt is on multiple medications, when would you want to administer their Ca suppliment?
|
2 hours before or after their other meds
|
|
|
What is the adverse effect of Ca?
|
Constipation
|
|
|
Which pts have the highest likelihood for Vit D deficiency?
|
Those with malabsorption syndrome
-Those not exposed to sunglight |
|
|
How do we get Vit D?
|
-Through our Diet
-Through direct UV sunlight |
|
|
What is an adverse effect of Vit D?
|
Increased levels of Calcium
|
|
|
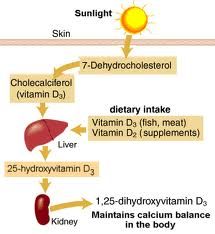
Which form of Vit D is obtain from diet and the sun?
Is this active? |
D3 or cholecalciferol
-No it is not active until it goes through the liver and kidney |
|
|
What is the active form of Vit D?
|
1,25-dihydroxyvitamin D3 or calcitriol
converted in the kidney |
|
|
Which form of Vit D is obtain from diet and the sun?
Is this active? |
D3 or cholecalciferol
-No it is not active until it goes through the liver and kidney |
|
|
What is the active form of Vit D?
|
1,25-dihydroxyvitamin D3 or calcitriol
converted in the kidney |
|
|
Which form of Vit D is obtain from diet and the sun?
Is this active? |
D3 or cholecalciferol
-No it is not active until it goes through the liver and kidney |
|
|
What is the active form of Vit D?
|
1,25-dihydroxyvitamin D3 or calcitriol
converted in the kidney |
|
|
Describe the Conversion of inactive Vit D from sunlight to the active form.
|
|
|
|
List all the Bisphosphonates.
|
-Pamidronate (Aredia): IV
-Alendronate (Fosamax): oral -Risedronate (Actonel): oral -Ibandronate (Boniva): oral |
|
|
What is the mechanism of action for Bisphosphonates?
|
Prevents bone resorption by inhibiting osteoclast activity
|
|
|
How do the pharmokinetics of bisphosphonates dictate its administration?
|
Because only 5% are absorbed on an empty stomach, the pt must take med in morning 30-45 mins prior to eating.
-Take with a big glass of water |
|
|
What should you as a nurse instruct your pt that is on bisphosphonates to do?
|
Sit upright or stand for 30-45 mins after taking becuase it causes esophageal erosions
|
|
|
What are some adverse effects of bisphosphonates?
|
-esophogeal erosion
-GI disturbances -Constipation -Diarrhea |
|
|
What is the MOA of calcitonin?
|
Inhibits Osteoclasts
|
|
|
Why is calcitonin not given as much?
|
Its admin routes cause pain
Nasal: sores Inj: painful |
|
|
Adverse effects of calcitonin?
|
GI upsets and pain at injection site
|