Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
148 Cards in this Set
- Front
- Back
|
describe the route of milk production and secretion.
is there just one hole for milk secretion? what is the dark circle around the nipple called |
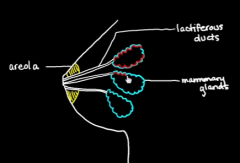
produced in mammary glands and head down via lactiferous ducts which open up into many holes
|
|
|
why do we have the areola?
|
to help babies find the breast
|
|
|
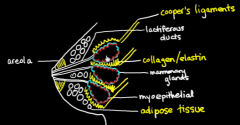
what cells help eject milk?
where are they? what embryonic layer are they from? |
myoepithelial cells lining the mammary glands
they are epithelial |
|
|
what forms the framework around the mammary glands and ducts?
support 3 padding 1 |
|
|
|
what is the most direct way that suckling facilitates milk to the baby?
|
suction power
|
|
|
What signals get sent to the mosther from suckling. What happens and where?
|
suckling --> hypothalamus -->
1. oxytocin to contract myoepithelium 2. inhibit dopamine --> increase prolactin --> lactogenesis |
|
|
what is an alternative route to the let down reflex that isn't suckling?
|
simply hearing a baby cry while you are lactating
|
|
|
NOW WE TALK ABOUT FETAL CIRCULATION!
What is the baby's lungs? |
amniotic fluid
|
|
|
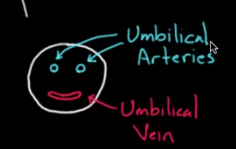
how many vessels are in the umbbilical cord? what are they called and are each carrying oxygenated or deoxygenated blood?
|
|
|
|
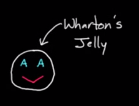
what substance suspends the vessels in the umbilical cord?
mnemonic for the 2 arteries and 1 vein? |
|
|
|
why is umbilican vein called a vein?
|
it carries blood TO the fetal heart
|
|
|
what structure does the uterine artery and vein run through?
what do they branch off of? |
the cardinal ligament
the internal iliac |
|
|
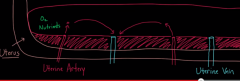
what happens on mom's side of the placenta?
|
|
|
|
what is the last area that the uterine vessels are whole within called?
|
basal plate
|
|
|
what is it like in the layer beyond the basal plate?
|
just like a hot tub with jets and drains where the water is blood
|
|
|
how does the fetus tap into all of this blood?
|
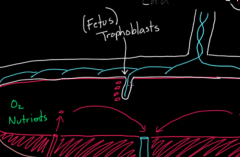
it invades trophoblasts to make villa to sample from the tub. each villi has a fetal vein.
|
|
|
are the RBC's of the mother being exchanged with the fetus?
|
no, they just pass off oxygen
|
|
|
what does the villus actually look like? why?
|
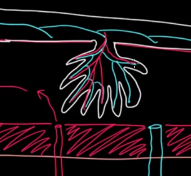
tree-like to maximize exchange
|
|
|
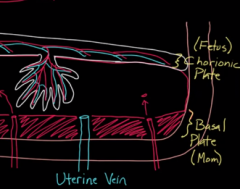
what is the plate holding all the fetal vessels called?
|
the chorionic plate
|
|
|
show how the two plates relate
|
|
|
|
who makes the contents of the tub?
|
both!
mom makes the pool baby makes the villi |
|
|
what is considered the placenta?
|
both plates and the pool between
|
|
|
where do the umbilical vessels enter the fetus?
|
the belly button!
|
|
|
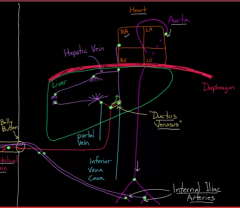
what are the two route from the umbilical vein to the fetal heart?
|
short cut to heart- ductus venosus under liver --> IVC
long way- join portal vein --> liver --> hepatic vein --> IVC |
|
|
why are there 2 paths for the umbilival vein blood?
|
1 to provide heart and thius rest of body with oxygen
another to provide nutrients fresh to the liver |
|
|
how does blood return to the mother? from what vessel?
why are there two umbilical arteries? |
from the internal arteries pair --> umbilical arteries
|
|
|
so describe the quality of the blood in the fetus?
|
it is neither fully oxygenated nor deoxygenated.. it's always mixed.
|
|
|
show the pic of the fetal circulatory system
|
|
|
|
what is the quality of the blood in the SVC and IVC for the fetus?
|
SVC- deoxygenate
IVC- oxygenated |
|
|
what do the pulmonary capillaries look like in the fetus? why?
|
very constricted because the lungs are filled with fluid and this hypoxic vasoconstriction
|
|
|
so what is the BP in the pulmonary arteries? RV?
|
very high in both
|
|
|
how do we relive this pressure? 2
|
1. foramen ovale- 1 way flap from RA to LA
2. ductus arteriosus- duct shunting blood from the pulonary artery to the aorta |
|
|
describe the foramen ovale and how it works and it's two components.
|
septum primum has a flap that is one way that flips out to the LA when pressure is put on the foramen ovale, an opening in the septum secundum in the RA side
|
|
|
what is period prevalence vs lifetime prevalence?
|
period-% of people with a condition during a certain period
lifetime- % of people who have had a condition at some point in their lives |
|
|
describe the steps of the foramen ovale forming. include direction of growth and where the blood is passing through in each step)
|
1. septum primum grown down toward endocardial cushion (blood goes through unsealed foramen primum)
2. septum primum reaches endocarial cushion, foramen primum disappears, foramen secundum appears as a hole in the septum primum from the top (foramen secundum) 3. septum secundum starts growing toward endocardial cushion (foramen secundum) 4. septum secundum covers whole area, but leaves the foramen ovale over the septum primum (flap out the foramen ovale) |
|
|
show the image of the foramen ovale developing
|

|
|
|
What happens to the foramen ovale and the shunt at birth?
|
the increase LA pressure pushes the septum rpimum shut and it seals off the foramen ovale.
|
|
|
Does all fetal blood go through the foramen ovale? why is this necessary?
|
no, some goes to the ductus arteriosis to help the RV practice pumping
|
|
|
Does any blood go to the lung of the fetus?
|
yes, 10%
|
|
|
what are the 3 layers from top to bottom of spun blood?
|

plasma, WBC/buffy layer, hematocrit/RBC
|
|
|
normal hematocrit for mom and baby? implllications?
|
mom- 35%
baby- 55% baby will steal proportionately more oxygen from mom |
|
|
what is the oxygen distribution between mommy and baby? why?
|
more in baby to promote growth
|
|
|
what is another way for baby to get more oxygen from mom?
|
to have hemoglobin with a greater affinity for oxygen
|
|
|
what is adult vs fetal hemoglobin called and composed of?
|
HbA- for Adult - 2 alpha proteins, 2 beta
HbF- for fetal- 2 alpha, 2 delta |
|
|
what does 2,3 DPG look like? what is it made from?
|
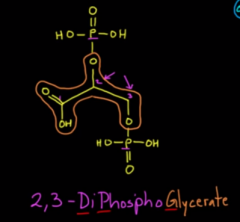
from 1,3 BPG from glycolysis
|
|
|
what does 2,3 DPG bind to? be specific? what does it do?
|
binds to the beta subunits in HbA to make them release oxygen
|
|
|
what are 3 conditions where you would have chronically elevated 2,3 DPG?
1 reason why? |
1. altitude
2. anemia 3. lung diseases these people chronically have low oxygen so are forced to use glycolysis a lot |
|
|
is both mother's and fetal blood in the pool?
|
no just mom
|
|
|
what is the bohr effect?
|
increase H+ makes oxygen fall off of hemoglobin
|
|
|
does mom or baby have higher oxygen concentration?
|
baby
|
|
|
what is the resistance of the placenta vessels? why?
|
low to make blood from the umbilical arteries go here
|
|
|
what happens to make the umbilical cord clamp down?
|
lowering of temperature makes wharton's jelly constrict
|
|
|
what causes the ductus arteriosus to close? 2
|
1. higher oxygen will cause the SM there to constrict
2. no more prostaglandin production from placenta keeping it open |
|
|
what happens to all the fetal vessel ducts?
|
they fibrose over and become ligaments
|
|
|
what does the following become?
1. umbilical vein 2. ductus venosum 3. foramen ovale 2 4. ductus arteriosus 5. umbilical arteries |
1. umbilical vein - ligamentum teres hepatis
2. ductus venosum - ligamentum venosum 3. foramen ovale - fossa ovale or patent foramen ovale 4. ductus arteriosus- ligamentum arteriosus 5. umbilical arteries- medial umbilical ligaments |
|
|
why are PFO's not really an issue?
|
pressure on the left is usually always higher than the right
|
|
|
what becomes of the more proximal part of the umbilical arteries?
|
internal iliac branches to the bladder.
|
|
|
START WITH DIT PREGNANCY
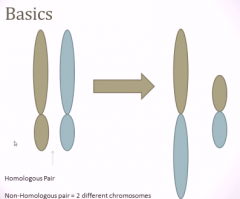
what is gravidity vs parity? |
gravid- # of pregnanciies
parity- # of types of deliveries |
|
|
what are the 4 types of parity? mnemonic?
|
TPAL
Term deliveries Preterm deliveries Abortions Living children |
|
|
what is considered term and preterm?
|
term- 37- 42 weeks
preterm- 20-37 weeks 3 weeks before 10 months is preterm |
|
|
define abortion?
|
anything ended before 20 weeks for any reason
|
|
|
give the numbers for a women who had term twins and thats it
|
G1P1002
only had 1 term pregnancy and delivery technically |
|
|
will dizygotic or monozygotic twins share placentas?
what are the 2 structures that can be split? |
dizygotic won't
monozygotic won't if they split early enough chorion and amnion |
|
|
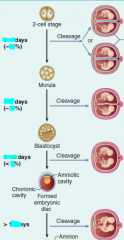
so give the timeline for the formation of each to decide if twins will share structures
1. chorion 2. amnion how do you remember this? |
1. chorion- 4 days
2. amnion- 8 days first priority is to tap into mother's blood supply |
|
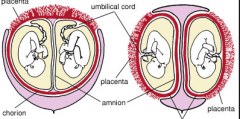
name what types these two are and some possibilities for what they could be
|
lelft- monozygotic diamnionic, monoplacental - 4-8 days - 75% of identical twins
right- dichorionic, diamnionic either 8-12 days for monozygotic (1%) or fraternal (100%) |
|
|
what % of twins are identical vs fraternal
|
identical- 20%
fraternal- 80% |
|
|
if identical twins split after 13 days, what happens?
|
siamese twins- baby has already started devleoping
|
|
|
what is the most common location for siamese twins to be connected?
|
the chest
|
|
|
|
|
|
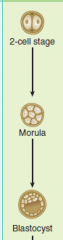
mnemonic for blastocyst?
|
cyst- a hole inside
|
|
|

|
|
|
what is the mnemonic for what is in the branchial arches?
|
The motor functions of each of the mixed CN's
1- 5- chewing 2- 7- facial muscles 3- 9- stylopharyngoal 4 and 6- 10- speaking and swalowing |
|
|
mnemonic for branchial pouch derivatives?
|
I have a POUCH of Ears, Tonsils, from Bottom To Top
1st- inner ear linings 2nd- lining over palatine tonsils 3rd- dorsal wings- bottom parathyroids 3rd- ventral wings- thymus 4th- upper parathyroids |
|
|
mnemonic for pharyngeal arches?
name the nerves and muscles. |
At the golden arches, kid will chew, smile, swallow stylishly, simply swallow, and then speak.
1st- Chew - V2, V3 - muscles of mastications, tensor tympani 2nd- Smile- CN7 - facial muscles 3rd- swallow stylishly- back of tongue and stylopharyngeus 4th - swallow- CN 10- superior laryngeal- everything above larynx. also back of tongue 6th- speak- CN10- recurrent laryngeal- larynx |
|
|
Now for cartilage... which of the ear bones are formed from which arches? mnemonic?
|
1st arch- chew- all cartilages begin with M
2nd arch- smile - all cartilages begin with S 1st- incus, malleus 2nd- stapes (only one that begins with S) |
|
|
Mnemonic for all cartilage in the 1st arch?what are they called collectively?
|
Meckel's cartilage- all begin with M(ish)
incus, Malleus, Mandible, spheno-Mandibular ligament |
|
|
Mnemonic for all cartilage in the 2nd arch? what are they called collectively?
|
Reichert's cartilage
Stapes, Styloid process, Stylopharyngeal ligament, plus lesser horn of hyoid bone (this is where the stylopharyngela ligament kind connects) JUST THINK OF S CARTILAGE AND THE STYLOPHARYNHEAL LIGAMENT |
|
|
Mnemonic for all cartilage in the 3rd arch?
|
no collective name
just the great horns of the hyoid |
|
|
Mnemonic for all the cartilage in the 4th-6th arch?
|
this is for speaking so all the ones involved in the larynx
crichoid, aretenoids, thyroid, corniculate, cuneform |
|
|
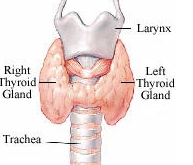
how does the thyroid cartilage and gland sit?
|
|
|
|
At what development stage will you get dichorionic, diamnionic?
|
before the mrula stage
|
|
|
At what development stage will you get monochorionic, diamnionic?
|
after morula, before blastocyst
|
|
|
SO WHAT CAN YOU SAY HAPPENS at the morula and blastocyst stage?
|
morula- will attach itseld to the placenta
blasticyst- will divide up the sac into amnions |
|
|
what kind of pregnancy do you have if you see a yolk sac with 2 fetal poles?
when did they divide? |
monozygotic, monochorionic, monoamniotic
split after 13 days and after the blastocyst stage |
|
|
what is one test for lung function we can get from an amniocentesis?
normal value? |
a lecithin:sphingomyelin test for lung maturity
should be greater than 2:1 |
|
|
what is a lecithin?
|
a phospholipid
|
|
|
what is usrfactant made of? be specific?
|
lecithins, but mainly dipalmitoylphosphatidylcholine
|
|
|
main role of cyto and syncitiotrophoblasts?
|
cyto- making main aoart of villi on iside
syncitio- inading into endometrium and producing b-hCG |
|
|
another name for the basal blate?
|
decidua basalis
|
|
|
what happens if a fetus manages ti implant in an area with no decidua basalis?
|
placenta accreta
|
|
|
what is the allantois?
|
the duct connecting the urogenital sinus and the ______
|
|
|
differnce between allantois and urachus and median umbilical?
|
the urachus is the allantois after birth and fibrosis
the median umbilical ligament is the urachus after final obliteration |
|
|
where does the urachus dump and what?
how do you know? |
it dumps fetal urine into the placenta
because it goes up the abdomen into the umbilical cord |
|
|
so how does the fetus pee out what it swallows into the amnion?
|
the regular urogenial opening (urethra)
|
|
|
where does the vitelline duct connect? 2
|
the midgut to the yolk sac
|
|
|
why may you see preeclampsia in the first trimester?
|
mplar pregnancy
|
|
|
tx and monitoring for molar pregnancy?
|
D&C and follow b-hCG to 0 to make sre you got all of it
|
|
|
what is the tx if the choriocarcinoma or molar pregnancy has spread? why?
|
chemotherapy because it has spread through blood to many places. chemo spreads through blood.
|
|
|
which type of molar pregnancy will have more b-hCG?
|
complete
|
|
|
most common cause of miscarriage?
be specific mnemonic? |
chromosomal abnormality- robertsonisn translocation
Robert likes to punch pregnant women in the stomach and make them miscarriage |
|
|
which chromosomes are involved usually in robertsonian translocations and why?
|
13, 14, 15, 21, and 22
they are acrocentric |
|
|
what does acrocentric mean? dissect
|
acro- tip (thing acrid sharp asstes)
chromosomes with the contromere very close to one tip |
|
|
Describe a robertsonisn translocation
|
when the chromosomes are translocating information, they accidentally pair the two long and two short arms up.
the short pair kind just disappears |
|
|
what is the long and short arm of the chromosome called? ,mnemonic?
|
p arm - short- Petite arm
q arm- longer arm |
|
|
what is held in the short arms usually?
|
repeated genes that are common and present in other chromosomes
|
|
|
when does the robertsonian translocation cause problems?
all the time? |
onlt when they are imbalanced (like happening between different chromosomes) and lose genes or add extra ones
|
|
|
are robertsonisn translocations genetic?
|
no, it;s just bad mluck
|
|
|
what kind of anatomical defect can lead to recurrent miscarriages?
|
bicornuate uterus
|
|
|
3 biggest things to investigate first when checking for infertility?
|
1. is she ovulation?
2. are the tubes in place? 3. what is the quality of ther sperm? think about the players and the most trecherous path |
|
|
what is IUI, IVF, and ICSI/
|
IUI- intrauterine insemination - put sperm in the uterus
IVF- put sperm and egg in a petri dish ICSI- intracytoplasmis sperm injection- put sperm directly into egg |
|
|
what is the typical procedure for surrogacy?
|
IVF and implantation into new woman
|
|
|
what is the single biggest predictor of pregnancy rates and how smooth it is?
|
the age of the egg
|
|
|
what happens to total blood volume and RBC content in pregnancy?
what is happening overall? |
total blood volume- up 50%
RBC- up 30% a physiologic anemia |
|
|
WHY may the blood become so dilute in pregnancy? 2
|
1. to give more oxygen to fetus
2, to lose less RBC's when we give birth and bleed |
|
|
what happens to BP throughout pregnancy if it is normal?
|
first decreases then returns back to normal
|
|
|
what is a twin-twin transfusion?
|
when twins share a umbilical cord blood supply and one twin gets more
|
|
|
if a pregnant woman who had HTN returns to the same HTN in second trimester, is that preeclampsia?
|
nope
|
|
|
theory behind why preeclampsia happens?
|
there is some sort of defect in the placenta that reveals dad's DNA and mom's immune system rushes to go attack it, creating clotting and vasospasms throughout the body
|
|
|
if a woman has swelling in feet, do they likely have preeclampsia?
what does? |
no, most pregnant women have this
but hands and face are less common |
|
|
what kind of visual changes would women get with preeclampsia? why>
|
scotomata or something else
vasospasms in head or too much BP up there |
|
|
what can you give a fetus to prepare it for preterm delivery?
|
a cortisol anlog
|
|
|
what are some effects of magnesium toxicity?
|
hyporeflexia
|
|
|
When would sx of ectopic pregnancy show/be on US?
|
7 weeks
|
|
|
what 3 thing sdo you look for to assess the gestational develpoment?
|
US findings
b-hCG gestational age should allcorrespond closely |
|
|
how often is ectopic in the fallopian tube?
|
99% of the time
|
|
|
dx for ectopic?
|
elevated b-hCG and abdominal pain/bleeding
|
|
|
is the b-hCG more or less than in a normal preg for ectopic? why?
|
less because not as much room to grow trophoblasts, which are normal
|
|
|
what would cause some vs a lot of uterine bleeding in ectopic?
|
when the ectopic placenta isn't producing enough b-hCG to support the endometrial lining and it sheds
OR the fallopian tube uptures |
|
|
treatment of light vs severe ectopic pregnancy?
|
light- methrexate to stem cell multiplication
severe- surgery to remove tube |
|
|
what are some risk factor for placenta abruption? what do they have in common?
|
all cause vasoconstriction or disturbance
smoking, cocaine, trauma (MVC) |
|
|
is it mom's blood ot baby's that bleeds with placental disruptions?
|
mom's (pool)
|
|
|
what should you do first when a pt comes in with painless vaginal bleeding in the 3rd trimester?
most likely what? |
placenta previa
do a US before a physical exam so you don't disturb the placenta |
|
|
normal amount of amniotic fluid?
|
1 L
|
|
|
differential for polyhydraminos? 2
|
esophageal or duodenal atresia
anencephaly (spina bifida, holoprosencephaly) |
|
|
differential for oligohydraminos2
|
placental insufficiency- not enough fluid going to baby
renal agenesis |
|
|
what syndrome can cause bilateral renal agenesis?
|
Potter Syndrome
|
|
|
describe pathophysiology of Potter Syndrome
|
nonfunctional kidneys --> oligohydraminos --> compression of fetus because no cushioning --> nothing can grow and expand including the lungs, face, and limbs especially
|
|
|
mnemonic for Potter SYndrome?
|
Kids that can't PEE will get POTTERS syndrome
|
|
|
what are the categories of all medicines?
what is it based on? |
Based on how much evidence there is, but C can be safer than B still etc.
A- Proven to be safe in humans B- Proven to be safe in animals C- No conclusive evidence in animals or humans, but likely safe. D- Demonstrated human risk X- |
|
|
mnemonic for maniffestations of potter syndrome?
|
|
|
|
What type of drug is used to start labor? siffix?
mnemonic? |
-prostones (sounds like prostaglandin)
PGE analogs to dilate cervix and create contractions |
|
|
what types of drugs are used to inhibit labor?
|
B2 agonists (relaxation)
|
|
|
examples of these B2 agonists?
|
Ritodrine and Tertbutaline
|
|
|
what is mifepristone?
mnemonic? |
p-one- has to do with progesterone
a progesterone competitive antagonist to terminate a pregnancy |
|
|
what is mifeprostone normally given with? be specific? why?
|
a -prostone like misoprostol to induce labor
|
|
|
what are you at increased risk for if you have had a c-section before?
during pregnancy? 2 why? during labor? 1 |
pregnancy- placenta previa and accreta because good soace is scarred
labor- uterine rupture |
|
|
what is a medication that inhibits labor called?
|
tocolytic
|
|
|
3 meds for tocolytics? why for each
|
magnesium sulfate- limit any kind of muscle contraction
tertbutaline and ritodrine- B2 agonist for relaxation |